
Abstract
Summary
In a simulated population of older women, we demonstrate that an upward shift in the population distribution of BMD by approximately 0.3SD may decrease the risk of incident fractures to the same extent as an intervention targeted to those with T-score less than −2.5.
Introduction
To investigate the impact of population level or targeted alterations to BMD on the incidence of fractures.
Methods
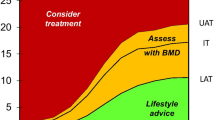
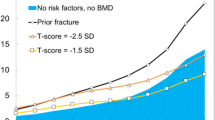
We used a simulated cohort of 49,242 women with age and body mass index distribution from the UK, and prevalence of other clinical risk factors based on European FRAX® cohorts. Using FRAX probabilities of major osteoporotic fracture (MOF: hip, clinical vertebral, distal forearm, proximal humerus) and hip fracture, calculated with femoral neck BMD, we determined the expected number of fractures over 10 years, stratified by 10-year age band from 50 years. We then investigated the effect of (i) uplifting all individuals with T-score below −2.5 to be exactly −2.5 (high-risk strategy) and (ii) shifting the entire BMD distribution upwards (population strategy).
Results
Overall, the high-risk strategy prevented 573 MOF including 465 hip fractures. Moving the BMD T-score distribution upward by 0.27SD gave an equivalent reduction in numbers of MOF; for hip fractures prevented, this was 0.35SD. A global upward 0.25SD BMD shift prevented 524 MOF including 354 hip fractures, with corresponding figures for an increase of 0.5SD being 973 MOF prevented and 640 hip fractures prevented. The ratio of hip fracture to MOF prevented differed by the two approaches, such that for the high-risk strategy, the ratio was 0.81, and for the population strategy was 0.68 (0.25SD BMD uplift) and 0.66 (0.5SD BMD uplift). The numbers of fractures prevented by the high-risk strategy increased with age. In contrast, the age-related increase in numbers of fractures prevented with the population strategy rose with age, but peaked in the 70–79-year age band and declined thereafter.
Conclusions
Both strategies reduced the numbers of expected incident fractures, with contrasting relative impacts by age and fracture site. Whilst the current analysis used UK/European anthropometric/risk factor distributions, further analyses calibrated to the distributions in other settings globally may be readily undertaken. Overall, these findings support the investigation of both population level interventions and those targeted at high fracture risk groups.



Similar content being viewed by others

References
Kanis JA, Oden A, Johnell O, Johansson H, de Laet C, Brown J, Burckhardt P, Cooper C, Christiansen C, Cummings S, Eisman JA, Fujiwara S, Glüer C, Goltzman D, Hans D, Krieg MA, la Croix A, McCloskey E, Mellstrom D, Melton LJ III, Pols H, Reeve J, Sanders K, Schott AM, Silman A, Torgerson D, van Staa T, Watts NB, Yoshimura N (2007) The use of clinical risk factors enhances the performance of BMD in the prediction of hip and osteoporotic fractures in men and women. OsteoporosInt 18:1033–1046
Harvey N, Dennison E, Cooper C (2010) Osteoporosis: impact on health and economics. Nat Rev Rheumatol 6:99–105
Kanis JA (1994) Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporos Int 4:368–381
Harvey N, Dennison E, Cooper C (2014) Osteoporosis: a lifecourse approach. J Bone Miner Res 29:1917–1925
Kanis JA, Cooper C, Rizzoli R, Reginster JY (2019) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 30:3–44
Hernandez CJ, Beaupre GS, Carter DR (2003) A theoretical analysis of the relative influences of peak BMD, age-related bone loss and menopause on the development of osteoporosis. Osteoporos Int 14:843–847
Riggs BL, Melton LJ 3rd (1986) Involutional osteoporosis. N Engl J Med 314:1676–1686
Kanis JA (1999) The use of calcium in the management of osteoporosis. Bone 24:279–290
Cooper C, Melton LJ 3rd (1992) Epidemiology of osteoporosis. Trends Endocrinol Metab 3:224–229
Cooper C (1996) Rationale and clinical indications for bone density measurements. Osteoporos Int 6 Suppl 2:6–8
Kanis JA, Johansson H, Odén A, McCloskey EV (2012) The distribution of FRAX(®)-based probabilities in women from Japan. J Bone Miner Metab 30:700–705
Dawson-Hughes B, Looker AC, Tosteson AN, Johansson H, Kanis JA, Melton LJ 3rd (2010) The potential impact of new National Osteoporosis Foundation guidance on treatment patterns. Osteoporos Int 21:41–52
Johansson H, Kanis JA, Oden A, Compston J, McCloskey E (2012) A comparison of case-finding strategies in the UK for the management of hip fractures. Osteoporos Int 23:907–915
Kanis JA, McCloskey EV, Johansson H, Oden A, Melton LJ 3rd, Khaltaev N (2008) A reference standard for the description of osteoporosis. Bone 42:467–475
Looker AC, Wahner HW, Dunn WL, Calvo MS, Harris TB, Heyse SP, Johnston CC Jr, Lindsay R (1998) Updated data on proximal femur bone mineral levels of US adults. Osteoporos Int 8:468–489
McCloskey E, Kanis JA, Johansson H, Harvey N, Odén A, Cooper A, Cooper C, Francis RM, Reid DM, Marsh D, Selby P, Thompson F, Hewitt S, Compston J (2015) FRAX-based assessment and intervention thresholds-an exploration of thresholds in women aged 50 years and older in the UK. Osteoporos Int 26:2091–2099
Kanis JA (1997) Strategies therapeutiques dans l’osteoporose. Med Ther 3:35–43
Odén A, McCloskey EV, Johansson H, Kanis JA (2013) Assessing the impact of osteoporosis on the burden of hip fractures. Calcif Tissue Int 92:42–49
Kanis JA, Oden A, Johansson H, McCloskey E (2012) Pitfalls in the external validation of FRAX. Osteoporos Int 23:423–431
Kanis JA, Harvey NC, Cooper C, Johansson H, Oden A, McCloskey EV (2016) A systematic review of intervention thresholds based on FRAX: A report prepared for the National Osteoporosis Guideline Group and the International Osteoporosis Foundation. Arch Osteoporos 11:25
Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, Moore L, O'Cathain A, Tinati T, Wight D, Baird J (2015) Process evaluation of complex interventions: Medical Research Council guidance. BMJ 350:h1258
Compston J, Cooper A, Cooper C et al (2017) UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos 12:43
Javaid MK, Kyer C, Mitchell PJ et al (2015) Effective secondary fracture prevention: implementation of a global benchmarking of clinical quality using the IOF Capture the Fracture(R) Best Practice Framework tool. Osteoporos Int 26:2573–2578
Johnell O, Kanis JA, Oden A, Johansson H, de Laet C, Delmas P, Eisman JA, Fujiwara S, Kroger H, Mellstrom D, Meunier PJ, Melton LJ III, O'Neill T, Pols H, Reeve J, Silman A, Tenenhouse A (2005) Predictive value of BMD for hip and other fractures. J Bone Miner Res 20:1185–1194
Kanis JA, Harvey NC, McCloskey E et al (2020) Algorithm for the management of patients at low, high and very high risk of osteoporotic fractures. Osteoporos Int 31(1):1–12
Nilsson AG, Sundh D, Bäckhed F, Lorentzon M (2018) Lactobacillus reuteri reduces bone loss in older women with low bone mineral density: a randomized, placebo-controlled, double-blind, clinical trial. J Intern Med 284:307–317
Clynes MA, Harvey NC, Dennison EM (2018) Early growth, bone development and risk of adult fracture. In: Harvey N, Cooper C (eds) Osteoporosis: a lifecourse epidemiology approach to skeletal health. CRC Press, Boca Raton, pp 33–42
Javaid MK, Eriksson JG, Kajantie E, Forsen T, Osmond C, Barker DJ, Cooper C (2011) Growth in childhood predicts hip fracture risk in later life. Osteoporos Int 22:69–73
Javaid MK, Lekamwasam S, Clark J, Dennison EM, Syddall HE, Loveridge N, Reeve J, Beck TJ, Cooper C (2006) Infant growth influences proximal femoral geometry in adulthood. J Bone Miner Res 21:508–512
Cooper C, Harvey NC, Bishop NJ, Kennedy S, Papageorghiou AT, Schoenmakers I, Fraser R, Gandhi SV, Carr A, D'Angelo S, Crozier SR, Moon RJ, Arden NK, Dennison EM, Godfrey KM, Inskip HM, Prentice A, Mughal MZ, Eastell R, Reid DM, Javaid MK, MAVIDOS Study Group (2016) Maternal gestational vitamin D supplementation and offspring bone health (MAVIDOS): a multicentre, double-blind, randomised placebo-controlled trial. Lancet Diabetes Endocrinol 4:393–402
Brustad N, Garland J, Thorsen J, Sevelsted A, Krakauer M, Vinding RK, Stokholm J, Bønnelykke K, Bisgaard H, Chawes BL (2020) Effect of high-dose vs standard-dose vitamin D supplementation in pregnancy on bone mineralization in offspring until age 6 years: a prespecified secondary analysis of a double-blinded, randomized clinical trial. JAMA Pediatr 174:419–427
Barker M, D'Angelo S, Ntani G, Lawrence W, Baird J, Jarman M, Vogel C, Inskip H, Cooper C, Harvey NC (2017) The relationship between maternal self-efficacy, compliance and outcome in a trial of vitamin D supplementation in pregnancy. Osteoporos Int 28(1):77–84
Funding
This work was supported by grants from Medical Research Council (MRC) (4050502589 (MRC LEU)), National Institute for Health Research (NIHR) Southampton Biomedical Research Centre, University of Southampton and University Hospital Southampton NHS Foundation Trust, and NIHR Oxford Biomedical Research Centre, University of Oxford, and supported by the International Osteoporosis Foundation and the UK Royal Osteoporosis Society Osteoporosis and Bone Research Academy.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 21 kb).
Rights and permissions
About this article

Cite this article
Harvey, N.C., Kanis, J.A., Liu, E. et al. Impact of population-based or targeted BMD interventions on fracture incidence. Osteoporos Int 32, 1973–1979 (2021). https://doi.org/10.1007/s00198-021-05917-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-021-05917-3