
Abstract
Summary
This study built a micro-simulation Markov model to determine the treatment threshold of osteoporosis in postmenopausal women in Mainland China. Treatment with zoledronate is cost-effective when FRAX-based (Fracture risk assessment tool) fracture probability is over 7%.
Introduction
The purpose of this study is to estimate FRAX-based fracture probabilities in Mainland China using real-world data, at which intervention could be cost-effective.
Methods
We developed a micro-simulation Markov model to capture osteoporosis states and relevant morbidities including hip fracture, vertebral fracture, and wrist fracture. Baseline characteristics including incidences of osteoporosis and distribution of risk factors were derived from the Peking Vertebral Fracture study, the largest prospective cohort study of postmenopausal women in Mainland China. We projected incidences of fractures and deaths by age groups under two treatment scenarios: 1) no treatment, and 2) zoledronate. We also projected total quality-adjusted life-years (QALY) and total costs including fracture management and osteoporosis drugs for cost-effectiveness analysis. Cost-effective intervention thresholds were calculated based on the Chinese FRAX model.
Results
Treatment with zoledronate was cost-effective when the 10-year probability of major osteoporotic fracture based on FRAX was above 7%. The FRAX threshold increased by age from 51 to 65 years old, and decreased in elder age groups, ranging from 4% to 9%.
Conclusions
Using real-world data, our model indicated that widespread use of zoledronate was of both clinical and economic benefit among Chinese postmenopausal women. Using a FRAX-based intervention threshold of 7% with zoledronate should permit cost-effective access to therapy to patients and contribute to reducing the disease burden of osteoporosis in Mainland China.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Background
Osteoporosis is a major public health concern in Mainland China. It was estimated that there were up to 70 million osteoporotic patients, and over 200 million patients with osteopenia in China in 2006 [1]. Osteoporotic fracture is the most severe complication of osteoporosis and results in hospitalization, disability, and mortality. The prevalence of vertebral fracture in postmenopausal Chinese women increased from 13.4% at ages 50–59 years, to 58.1% at age 80 years or older [2]. The overall major osteoporotic fracture in Chinese population was estimated to be 2.69 million cases in 2015 [3], indicating an enormous disease burden of osteoporotic fractures in China.
Osteoporosis treatment beforehand exhibits efficacy in fracture risk reduction. Of all treatment regimens, bisphosphonate is the most commonly used drug and was predicted to be cost-effective in other models [4]. In one of our previous studies (unpublished), alendronate was dominated by zoledronate in cost-effectiveness analysis, suggesting zoledronate a better option for treating Chinese postmenopausal women. In Mainland China, there is no universally accepted policy for treating patients at high risk, and only a minority of osteoporotic people receive proper treatment due to lack of evidence-based guidelines and recommendations [5]. Fracture risk assessment tool (FRAX) is a popular tool worldwide, used to predict 10-year probability of osteoporotic fracture based on clinical risk factors and femoral neck bone mineral density (BMD) [6]. Several cost-effectiveness analyses based on Western settings suggest that osteoporotic treatment should be initiated when the 10-year major fracture probability, based on FRAX, is over 7-15% [7,8,9,10]. Previous studies on estimating the FRAX threshold for the Chinese population were only limited to clinical observations or expert consensus [11,12,13,14].
We introduced real-world data from the Peking Vertebral Fracture (PK-VF) study into modeling to improve the robustness of cost-effectiveness analysis. The PK-VF study is currently the largest prospective cohort study of postmenopausal osteoporotic women in Mainland China, which involved 1100 women and follow-up from 2008 to 2013, to capture baseline epidemiological data of osteoporosis and osteoporotic vertebra fracture [2, 15,16,17]. The epidemiological data of the cross-sectional survey in 2008 has been published, including prevalence of osteoporosis and osteoporotic vertebra fracture and the distribution of risk factors of osteoporosis in the population [2].
In this study, we built a micro-simulation Markov model based on the PK-VF study. We aim to estimate the intervention threshold of FRAX in Mainland China, at which treatment with zoledronate could be cost-effective.
Methods
Model approach
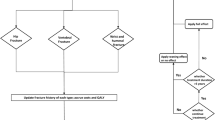
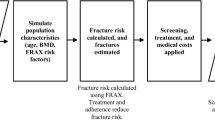
We developed an individual-based micro-simulation Markov model in NetLogo 5.3.1 (Evanston, IL) to evaluate cost-effectiveness of osteoporotic treatment with zoledronate under different initiation thresholds. Subjects in the model were simulated on the following aspects: age, BMI, osteoporosis status, fracture status, risk factors of fracture (including previous fracture, parent fracture, smoking, alcohol, use of glucocorticoid, and the history of rheumatoid arthritis and secondary osteoporosis), and medical costs (including drug costs and fracture management costs) (Fig. 1a). Subjects in the model could transit between different states, including states of non-fracture, fracture, and postfracture, as shown by arrows (Fig. 1b). We simulated 20,000 people representing Chinese postmenopausal women as a closed cohort with a lifelong time horizon. A discount rate was set as 3% per year for both costs and effectiveness. Cost-effectiveness was considered as ICER less than 3 times of per capita GNP, which was $20,000/QALY for 2018 China.

Schematic of the model structure. a Subjects in the model were simulated on the aspects of demographic feature, health feature, risk factor feature, and treatment feature. b Subjects could transit between different states, including states of non-fracture, fracture, and postfracture, as shown by arrows. Multiple fractures were allowed to happen in the same subjects during the lifetime. All states would also be absorbed into death state. c The anti-osteoporosis treatment would be initiated to subjects when FRAX score was higher than the threshold, or when fracture happened in the subject. Once initiated, we treated those subjects for five years under each of the two treatment scenarios, including (1) no treatment and (2) zoledronate. Subjects might drop-off during the 5-year treatment, and the remaining effect would decrease linearly in the next 5-year posttreatment
Baseline population from real-world data
We incorporated characteristics from the PK-VF study into the model with a stochastic sampling method for baseline population setup. By initial setting up the population, individuals’ characteristics were distributed according to the PK-VF study, including eight risk factors related to osteoporotic fracture in FRAX that is body mass index (BMI), previous fracture, parent fracture hip, current smoking, glucocorticoid use, rheumatoid arthritis, secondary osteoporosis, and alcohol use. For each age group, we randomly selected a number of individuals of the same age, together with their osteoporotic status, accompanied risk factors and treatment histories, from PK-VF participants. The percentage of each clinical risk factor based on PK-VF cohort was listed in Supplementary Table 1. As most of the risk factors (e.g., parent fracture hip, current smoking, glucocorticoid use, rheumatoid arthritis, BMI, secondary osteoporosis, and alcohol use) may have sustained impact on the osteoporosis-related fractures, we assumed that the risk factors of individuals simulated in the model remain unchanged except for previous fractures, which is updated if osteoporotic fractures occurred. For example, we assumed the effect of smoking on the increased risk of osteoporosis remains sustained no matter the individual stopped smoking or not.
Fracture risks and mortality
Our model began with women in the no-fracture state and simulated yearly transition till death. Osteoporosis developed with a yearly probability by age derived from the age-specific incidence of osteoporosis from PK-VF study (Table 1). The incidence of vertebral fracture, hip fracture, and wrist fracture were from pooled data of the Hong Kong Osteoporosis Study, the Hefei osteoporosis project, and a Norwegian study (multiplied by 0.72 to adjust for the Chinese population) [18,19,20] (Table 1). Osteoporotic subjects were more likely to experience fractures, with the relative risks published by Melton et al. [21]. The risk of a subsequent fracture increased when a prior fracture occurred [22]. Age distribution and natural mortality rate were from the 2012 National Sample Survey on Population Changes [33]. Standardized mortality ratios (SMR) of vertebral fracture, hip fracture, and wrist fracture were set as 1.82, 2.43, and 1.42 respectively [23] (Table 1).
Treatment strategies
We incorporated the treatment of zoledronate into the model, dosed as 5 mg a year, combined with calcium and vitamin D3 supplement (calcium 600 mg + vitamin D3 125IU per tablet), dosed once a day. The effect of zoledronate on reducing fracture risks was taken from clinical trials [26, 34, 35].
We calculated the 10-year major fracture probability (FRAX score) for each subject based on FRAX equation [6], which incorporated covariates including age and risk factors. Those with an estimated FRAX score higher than the threshold set were eligible for treatment. The antiosteoporosis treatment was initiated for subjects when FRAX score was higher than the threshold, or when fracture occurred in the subject (Fig. 1c). Once initiated, those subjects would be treated for five years under each of the two treatment scenarios: (1) no treatment or (2) zoledronate. The remaining effect was assumed to decrease linearly in the next 5 years after the treatment was over [36].
Imperfect adherence and persistence may affect the cost-effectiveness of the treatment and were thus incorporated in the model (Table 1) [27, 37]. Adherence was defined as the extent to which the subject acted in accordance with the prescribed drug, with respect to dosage and timing [30]. We set the adherence of zoledronate to be 1, as zoledronate was injected once a year. Subjects in the model may also drop out during the 5-year treatment, and persistence was defined as the duration from initiation until discontinuation of the treatment with a certain drug [30].
Cost assumptions
Costs of vertebral, hip, and wrist fracture referred to all direct medical costs and direct nonmedical costs reported by Qu et al. in 2012 [31]. Direct medical costs included costs of outpatient and inpatient care, examination, medication, rehabilitation, and physical therapy after fracture; direct non-medical costs included traffic fee, preventive care foods, and specific equipment. All fracture costs (data collected in 2012) were converted to 2018 RMB by a total inflation rate of 1.1466 reported by inflation.eu [32]. Costs of zoledronate (100 ml: 5 mg per year) and calcium + vitamin D supplement (calcium 600 mg + vitamin D3 125IU per tablet per day) was obtained from the Chinese market drug price database (access date Feb 07, 2019) [28]. RMB was converted to US dollars at the exchange rate of 6.7426 (Feb 07, 2019).
Utilities
Quality-adjusted life year (QALY) is a measurement of both quality and quantity of life lived, varying from 0 to 1, where 0 referring to death and 1 referring to perfect health. The age-specific QALY for the general population (Table 1) was based on the National Health Services Survey 2008 in China [24]. The QALY of different fracture types in the general population and osteoporotic population (Table 1) were obtained from a meta-analysis [25].
Presentation of results
We projected QALY, as a measurement of health and total costs of both fracture management and osteoporosis drugs for the cost-effectiveness analysis. The incremental cost-effectiveness ratio (ICER) was calculated as (cost A–cost B)/(QALY A–QALY B). The willingness to pay (WTP) was assumed to be 3 times of per capita GNP, which was $20,000/QALY for 2018 China.
Sensitivity analysis
To test the robustness of the model to uncertainties of input data, one-way sensitivity analysis comparing the treatment of zoledronate to no treatment was performed on key model parameters, including fracture incidence, incidence of osteoporosis, standard mortality ratio, relative risk of subsequent fracture following a prior fracture, QALY by age, QALY by fracture types, relative risk of fracture with treatment, persistence, treatment year, adherence, drug cost, and annual discount. The upper and lower limits of each key parameter are listed in Table 1 and Appendix.
Results
Validation
Face validation was done by consulting experts on osteoporosis prevention and treatment. Internal validation was performed on comparison of annual fracture incidences from model prediction to those from input data (Supplementary Table 2). The projected incidences were all within ± 5% of the reference value. External validation was performed on comparison of life expectancy, prevalence of osteoporosis, and lifetime fracture risk predicted from model to those from literature (Supplementary Table 3) [38,39,40]. Cross-model validation was not performed, as no modeling work has been done on estimating the intervention threshold of Chinese mainland population.
Intervention FRAX threshold estimation
Comparing the no-treatment scenario to treatment with zoledronate, the total costs increased from $1407.4 to $1822.9 per person, and the corresponding QALYs increased from 9.232 to 9.269. The ICER was $26637.3, $22129.7, $20338.4, $19285.0, $18181.0, $16680.2, $15047.7, and $14447.7 per QALY at FRAX threshold 0.02, 0.06, 0.07, 0.08, 0.09, 0.1, 0.5, and 1, respectively. As Fig. 2 indicated, the overall treatment threshold was 7% for treatment with zoledronate to be cost-effective in comparison to no treatment.

FRAX threshold for zoledronate. Treatment with zoledronate for patients with 10-year major fracture probability by FRAX over 0.07 was cost-effective in comparison with no treatment
Furthermore, we conducted cost-effectiveness analysis by age groups. As Fig. 3 and Supplementary Table 4 indicated, FRAX thresholds in different age groups ranged from 0.040 to 0.090. The threshold increased by age from 51 to 65 years old, and decreased in elder age groups.

Heatmap of incremental cost-effectiveness ratio (ICER) for zoledronate by age-group and by FRAX threshold. Red lines indicated the willingness to pay (WTP) as $20,000/QALY
We also performed a subgroup cost-effectiveness analysis on subjects all with previous fracture history (Supplementary Table 5, Fig. 4). By comparing Supplementary Table 5 to Supplementary Table 4, treatment with zoledronate was found to be cost-saving in the youngest and oldest age groups with previous fracture, while in other age groups, the treatment threshold based on FRAX was similar between people with and without previous fracture.

Heatmap of incremental cost-effectiveness ratio (ICER) for zoledronate in subjects with previous fracture by age-group and by FRAX threshold. Red lines indicated the willingness to pay (WTP) as $20,000/QALY
Sensitivity analysis
We performed sensitivity analysis on key model parameters, comparing the treatment of zoledronate to no treatment (Supplementary Table 6). As shown in the tornado plot (Fig. 5), the drug cost of zoledronate, incidence of vertebral fracture in osteoporosis, and QALY by age and persistence were the most sensitive parameters, but ICERs for all parameters remain below $23,000/QALY.

Tornado plot of one-way sensitivity analysis on key model parameters, comparing treatment with zoledronate to no-treatment scenario. The upper and lower limits of all key model parameters run for the sensitivity analysis were listed in Table 1. ICER, incremental cost-effectiveness ratio; RR, relative risk; QALY, quality-adjusted life year
Discussion
In this study, we built an individual-based Markov model of osteoporosis simulating postmenopausal women in Mainland China, based on real-world data from the PK-VF study. We predicted the intervention threshold of FRAX in Mainland China at which treatment with zoledronate could be cost-effective and calculated the variation of the threshold in different age groups.
In Mainland China, there is no accepted criterion for initiating the treatment of osteoporosis. Current expert consensus in China is that anti-osteoporosis treatment should begin in any of the following conditions: (1) the occurrence of vertebral fragile fracture or hip fragile fracture; (2) BMD of femoral neck, whole hip, lumbar vertebrae, or distal radius < − 2.5; (3) − 2.5 < BMD < − 1 plus (1) occurrence of the proximal humerus, distal forearm, or pelvis fragile fracture or (2) 10-year hip fracture probability > 3% or 10-year major fracture probability > 20% predicted by FRAX [41]. However, there has been no cost-effectiveness analysis to determine a Chinese-specific threshold to initiate osteoporosis treatment based on FRAX. Thus, building a cost-effectiveness model that predicts FRAX thresholds for the Chinese population is both important and urgent.
Several cost-effectiveness analyses have been performed on predicting the disease burden of osteoporosis in postmenopausal women in Mainland China [3, 42,43,44,45], but none of them were based on real-world data of osteoporotic cohorts in the Chinese population. This study, however, was based on our previous Peking Vertebral Fracture (PK-VF) [2, 15,16,17], in which 1100 Chinese postmenopausal women were followed up from 2008 to 2013, and data were collected on the incidence and prevalence of osteoporosis and osteoporotic vertebra fracture, and the distribution of risk factors of osteoporosis in the population [2]. Introducing real-world data into modeling would significantly improve the simulation.
The determination of cost-effectiveness FRAX intervention threshold should be country-specific, considering the large variation of epidemiology and economic conditions across countries. For example, osteoporosis treatment was predicted to be cost-effective when 10-year major fracture exceeded 7% in UK [7], 15% in Switzerland [8], 10% in Greece [9], 8.8% in Portugal [10], and when 10-year hip fracture exceeded 3% in USA [46]. There have been a few studies estimating the intervening threshold of osteoporosis for Chinese population based on FRAX, but they were only limited to clinical observations or expert consensus without the evaluation of the economic and disease burden of osteoporosis [11,12,13,14].
No cost-effectiveness analysis has been done on estimating FRAX threshold in China so far. One of the reasons was that real-world data of the distribution of clinical risk factors were not available in China before [45]. There were eight clinical risk factors in FRAX model to determine a 10-year probability of major fracture and hip fracture of an individual, including age, sex, BMI, previous fracture, parent fracture hip, current smoking, glucocorticoid use, rheumatoid arthritis, secondary osteoporosis, and alcohol use (with or without the addition of femoral neck BMD). As risk factors of osteoporosis were always not independent of each other, it would lead to potential bias if we were to bring each risk factor separately into the model. For example, current smokers are more likely to be a regular alcohol drinker. To solve this issue, we generated a sampling table of risk factors based on our PK-VF cohort, and randomly sampled a group of risk factors as a whole from the sampling table for each subject simulated in the model.
There are various anti-osteoporosis drugs among which bisphosphonate is the most widely used one. Bisphosphonate functions in inhibiting the bone reabsorption process of osteoclasts. Alendronate, an oral bisphosphonate, is dosed once per week, and zoledronate is dosed once a year intravenously. Alendronate and zoledronate reduced the risk of vertebral fracture by 48% and 70% respectively in clinical trials [26, 47], and in one of our previous studies (unpublished), alendronate was dominated by zoledronate in cost-effectiveness analysis, suggesting zoledronate a better option for treating Chinese postmenopausal women.
As indicated in Fig. 2, FRAX threshold for the whole Chinese population was predicted to be 7%. FRAX thresholds differed in different age groups (Fig. 3 and Supplementary Table 4), as the number first increased in age groups younger than 65 years, and decreased in elder age groups. The reason behind this phenomenon is the bidirectional effect of aging on the resultant gain of QALYs, and thus on the ICERs, in a treatment-as-prevention mode, (1) early intervention with low FRAX threshold among younger patients, who have longer expected lifetime, resulted in more cumulative QALYs gained. (2) Intensive intervention with low FRAX threshold among older patients, who have higher fracture risk, resulted in a marked reduction of osteoporotic fractures and related deaths and thus in more QALYs gained. Therefore, we suggested additional resources and attentions shift to the middle aged or advanced aged.
In the external validation table (Supplementary Table 3), a gap was found between the projected life expectancy (16.49) and the reference life expectancy (16.9) in the age group of 65–69 years. We think the reason for the gap was that we used the overall death rate by age from a national survey [33], and applied osteoporosis, fractures, and deaths due to fractures to the simulated population additionally. Therefore, the simulated population presented a slightly higher death rate and thus a shorter life expectancy, especially among the elders. However, such an overestimated death rate would result in an underestimated benefit of anti-osteoporosis treatment, because it relies on long-term follow-up to observe the benefit of treatment of osteoporosis in preventing fractures, and overestimation of the death rate tends to underestimate the preventive gain of QALYs and the cost-effectiveness of treatment. Currently, treatment of osteoporosis in clinical practice was rather insufficient. With such a conserved estimation, we put forward a FRAX-based intervention threshold as 7%.
There are certain limitations to this study. First, not all data needed for modeling were available for the Chinese population. For example, the incidence of wrist fracture was adopted from the Norwegian population, and multiplied by 0.72 to adjust to the Chinese population [20]. And we generally stratified transition-probabilities to osteoporotic status from healthy status by age, regardless of those listed risk factors such as BMI, parent fracture, current smoking. Since only 67 new cases of osteoporosis were observed in the 5-year follow-up of PK-VF study, the impact of these covariates on the incidences was not available. And for the same reason, we took only age, previous fractures, treatment, and osteoporotic status as impact factors on transition probabilities of fractures but did not considered the impact of all listed risk factors above. Second, our real-world data were collected in Beijing population, which may not represent the complete picture of the Chinese population. Our group is now performing an ongoing national-wide epidemiological study on osteoporosis with over 20,000 people recruited, and will attempt to incorporate these data into modeling in the future. Third, side effects of zoledronate, such as osteonecrosis of the jaw and atypical femoral fracture, were not considered in the model. The reason is that the health state utility of these side effects was unclear for Chinese population, and these effects occur rarely at the dose of treating osteoporosis. Fourth, one-way sensitivity analysis was performed in the study, which may not be as robust as probabilistic sensitivity analysis. However, we found ICERs tested on all variables in the current sensitivity analysis fell below $23,000, suggesting the results were not sensitive to the uncertainty of those input data. Fifth, we used visual analogue scale (VAS)-based QALY by fracture types as the input data of the model. Though a trade time-off (TTO)-based QALY model was available for Chinese population [48], we were unable to use it to calculate QALY by fracture types, as we did not collect the information in 5 dimensions (i.e., mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and 3 levels (i.e., 1 = no problems, 2 = some/moderate problems, and 3 = extreme problems) for each individual in PK-VF study. As an alternative, we used the VAS-based QALY data by fracture types in the model [25], which has also been used in other previous cost-effectiveness analysis [43, 45].
Conclusions
This study is the first cost-effectiveness analysis simulating osteoporosis and osteoporotic fractures in Chinese postmenopausal women based on real-world data. The study indicated that widespread use of zoledronate was of clinical and economic benefit to Chinese postmenopausal women with a 10-year major fracture probability by FRAX over 7%.
References
Chinese health promotion fundation editorial board of Chinese White Papers of osteoporosis (2009) Chinese White Papers of osteoporosis. Chin J Health Manag 3:148–154
Cui L, Chen L, Xia W et al (2017) Vertebral fracture in postmenopausal Chinese women: a population-based study. Osteoporos Int 28:2583–2590
Si L, Winzenberg TM, Jiang Q, Chen M, Palmer AJ (2015) Projection of osteoporosis-related fractures and costs in China: 2010-2050. Osteoporos Int 26:1929–1937
Kanis JA, Adams J, Borgstrom F, Cooper C, Jonsson B, Preedy D, Selby P, Compston J (2008) The cost-effectiveness of alendronate in the management of osteoporosis. Bone 42:4–15
Chinese Medical Association the Branch of Osteoporosis and Bone Mineral Disease (2017) Guideline of diagnosis and treatment of primary osteoporosis. Chin J Osteoporos Bone Miner Res 10:413–444
FRAX (2017) WHO fracture risk assessment tool. . https://www.sheffield.ac.uk/FRAX/tool.aspx?country=2. Accessed 07/10 2017
Kanis JA, McCloskey EV, Johansson H, Strom O, Borgstrom F, Oden A (2008) Case finding for the management of osteoporosis with FRAX--assessment and intervention thresholds for the UK. Osteoporos Int 19:1395–1408
Lippuner K, Johansson H, Borgstrom F, Kanis JA, Rizzoli R (2012) Cost-effective intervention thresholds against osteoporotic fractures based on FRAX(R) in Switzerland. Osteoporos Int 23:2579–2589
Makras P, Athanasakis K, Boubouchairopoulou N, Rizou S, Anastasilakis AD, Kyriopoulos J, Lyritis GP (2015) Cost-effective osteoporosis treatment thresholds in Greece. Osteoporos Int 26:1949–1957
Marques A, Lourenco O, Ortsater G, Borgstrom F, Kanis JA, da Silva JA (2016) Cost-effectiveness of intervention thresholds for the treatment of osteoporosis based on FRAX((R)) in Portugal. Calcif Tissue Int 99:131–141
Zhang Z, Ou Y, Sheng Z, Liao E (2014) How to decide intervention thresholds based on FRAX in central south Chinese postmenopausal women. Endocrine 45:195–197
Cheung E, Cheung CL, Kung AW, Tan KC (2014) Possible FRAX-based intervention thresholds for a cohort of Chinese postmenopausal women. Osteoporos Int 25:1017–1023
Chang AJ, Ying Q, Chen XN, Wang WM, Chen N (2016) Evaluation of three risk assessment tools in discriminating fracture status among Chinese patients undergoing hemodialysis. Osteoporos Int 27:3599–3606
Cheung EY, Bow CH, Cheung CL, Soong C, Yeung S, Loong C, Kung A (2012) Discriminative value of FRAX for fracture prediction in a cohort of Chinese postmenopausal women. Osteoporos Int 23:871–878
Zhao J, Xia W, Nie M et al (2012) A haplotype of MATN3 is associated with vertebral fracture in Chinese postmenopausal women: Peking Vertebral Fracture (PK-VF) study. Bone 50:917–924
Li N, Wang X, Jiang Y et al (2014) Association of GALNT3 gene polymorphisms with bone mineral density in Chinese postmenopausal women: the Peking Vertebral Fracture study. Menopause 21:515–521
Zhao J, Xia W, Nie M et al (2011) The levels of bone turnover markers in Chinese postmenopausal women: Peking Vertebral Fracture study. Menopause 18:1237–1243
Bow CH, Cheung E, Cheung CL et al (2012) Ethnic difference of clinical vertebral fracture risk. Osteoporos Int 23:879–885
Wang J, Wang Y, Liu WD, Wang F, Yin ZS (2014) Hip fractures in Hefei, China: the Hefei osteoporosis project. J Bone Miner Metab 32:206–214
Lofthus CM, Frihagen F, Meyer HE, Nordsletten L, Melhuus K, Falch JA (2008) Epidemiology of distal forearm fractures in Oslo, Norway. Osteoporos Int 19:781–786
Melton LJ 3rd, Thamer M, Ray NF, Chan JK, Chesnut CH 3rd, Einhorn TA, Johnston CC, Raisz LG, Silverman SL, Siris ES (1997) Fractures attributable to osteoporosis: report from the National Osteoporosis Foundation. J Bone Miner Res 12:16–23
Kanis J, Brazier J, Stevenson M, Calvert N, Lloyd Jones M (2003) Treatment of established osteoporosis: a systematic review and cost-utility analysis. Health Technol Assess 6:146
Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR (2009) Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA 301:513–521
Sun S, Chen J, Johannesson M, Kind P, Xu L, Zhang Y, Burstrom K (2011) Population health status in China: EQ-5D results, by age, sex and socio-economic status, from the National Health Services Survey 2008. Qual Life Res 20:309–320
Si L, Winzenberg TM, de Graaff B, Palmer AJ (2014) A systematic review and meta-analysis of utility-based quality of life for osteoporosis-related conditions. Osteoporos Int 25:1987–1997
Black DM, Delmas PD, Eastell R et al (2007) Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 356:1809–1822
Tremblay E, Perreault S, Dorais M (2016) Persistence with denosumab and zoledronic acid among older women: a population-based cohort study. Arch Osteoporos 11:30
Pharmcube: Market drug price database of China. http://db.pharmcube.com/database/drugib/index Accessed Feb 07 2019
China Center for Health Economic Research (2011) China Guidelines for Pharmacoeconomic Evaluations. Beijing.
Cramer JA, Roy A, Burrell A, Fairchild CJ, Fuldeore MJ, Ollendorf DA, Wong PK (2008) Medication compliance and persistence: terminology and definitions. Value Health 11:44–47
Qu B, Ma Y, Yan M, Wu HH, Fan L, Liao DF, Pan XM, Hong Z (2014) The economic burden of fracture patients with osteoporosis in western China. Osteoporos Int 25:1853–1860
Inflation: current and historic inflation by country. http://www.inflation.eu. Accessed Feb 07 2019
National Bureau of Statistics (2016) Status of deaths by age and sex (2011.11.1-2012.10.30). 2012 National Sample Survey on Population Changes. China Statistics Press
Chung M, Lee J, Terasawa T, Lau J, Trikalinos TA (2011) Vitamin D with or without calcium supplementation for prevention of cancer and fractures: an updated meta-analysis for the U.S. Preventive Services Task Force. Ann Intern Med 155:827–838
Wells GA, Cranney A, Peterson J, Boucher M, Shea B, Robinson V, Coyle D, Tugwell P (2008) Alendronate for the primary and secondary prevention of osteoporotic fractures in postmenopausal women. Cochrane Database Syst Rev Cd001155
Nayak S, Roberts MS, Greenspan SL (2011) Cost-effectiveness of different screening strategies for osteoporosis in postmenopausal women. Ann Intern Med 155:751–761
Cheng TT, Yu SF, Hsu CY, Chen SH, Su BY, Yang TS (2013) Differences in adherence to osteoporosis regimens: a 2-year analysis of a population treated under specific guidelines. Clin Ther 35:1005–1015
Cheng XG, Yang DZ, Zhou Q et al (2007) Age-related bone mineral density, bone loss rate, prevalence of osteoporosis, and reference database of women at multiple centers in China. J Clin Densitom 10:276–284
Park C, Ha YC, Jang S, Jang S, Yoon HK, Lee YK (2011) The incidence and residual lifetime risk of osteoporosis-related fractures in Korea. J Bone Miner Metab 29:744–751
WHO (2019) Life expectancy: life tables by country China. World Health Organization. . http://apps.who.int/gho/data/view.main.60340?lang=en. Accessed 06-24 2019
Chinese medical associaton branch of osteoporosis and bone mineral disease (2017) Guideline of prevention and treatment of primary osteoporosis. Chin J Osteoporos Bone Miner Res 10:413–443
Jiang Y, Ni W (2016) Expected lifetime numbers, risks, and burden of osteoporotic fractures for 50-year old Chinese women: a discrete event simulation incorporating FRAX. J Bone Miner Metab 34:714–722
Ni W, Jiang Y (2017) Evaluation on the cost-effective threshold of osteoporosis treatment on elderly women in China using discrete event simulation model. Osteoporos Int 28:529–538
Si L, Winzenberg TM, Chen M, Jiang Q, Neil A, Palmer AJ (2016) Screening for osteoporosis in Chinese post-menopausal women: a health economic modelling study. Osteoporos Int 27:2259–2269
Si L, Winzenberg TM, Jiang Q, Palmer AJ (2015) Screening for and treatment of osteoporosis: construction and validation of a state-transition microsimulation cost-effectiveness model. Osteoporos Int 26:1477–1489
Tosteson AN, Melton LJ 3rd, Dawson-Hughes B, Baim S, Favus MJ, Khosla S, Lindsay RL (2008) Cost-effective osteoporosis treatment thresholds: the United States perspective. Osteoporos Int 19:437–447
Liberman UA, Weiss SR, Broll J, Minne HW, Quan H, Bell NH, Rodriguez-Portales J, Downs RW Jr, Dequeker J, Favus M (1995) Effect of oral alendronate on bone mineral density and the incidence of fractures in postmenopausal osteoporosis. The Alendronate Phase III Osteoporosis Treatment Study Group. N Engl J Med 333:1437–1443
Liu GG, Wu H, Li M, Gao C, Luo N (2014) Chinese time trade-off values for EQ-5D health states. Value Health 17:597–604
Hiligsmann M, Reginster JY, Tosteson ANA et al (2019) Recommendations for the conduct of economic evaluations in osteoporosis: outcomes of an experts’ consensus meeting organized by the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) and the US branch of the International Osteoporosis Foundation. Osteoporos Int 30:45–57
Husereau D, Drummond M, Petrou S, Carswell C, Moher D, Greenberg D, Augustovski F, Briggs AH, Mauskopf J, Loder E (2013) Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. Pharmacoeconomics 31:361–367
Funding
This study was supported by grants from China Postdoctoral Science Foundation Grant (2018M631396), National Natural Science Foundation of China (No. 81070687, 81170805 and 81670714), Beijing Natural Science Foundation (No. 7121012), National Key Program of Clinical Science (WBYZ2011-873) and Collaborative Innovation Team Project of Medical and Health Science and Technology Innovation Project of Chinese Academy of Medical Sciences (No. 2016-I2M-3-003).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Cui, L., He, T., Jiang, Y. et al. Predicting the intervention threshold for initiating osteoporosis treatment among postmenopausal women in China: a cost-effectiveness analysis based on real-world data. Osteoporos Int 31, 307–316 (2020). https://doi.org/10.1007/s00198-019-05173-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-019-05173-6