
Abstract
Purpose
Although the development of digital mental health support for people with psychosis has been increasing, the development and opportunities to access this have been more limited compared to other mental health conditions. Qualitative research exploring the experiences of using digital interventions amongst people with psychosis is even less well developed; however, such research is crucial in capturing the experiences of using digital interventions to ensure they are meeting the needs of people with psychosis. This paper aimed to synthesise qualitative data related to the experiences of people with psychosis who have used digital interventions.
Methods
A systematic literature search was conducted of articles published between 1992 and October 2023 using PubMed, MBase, PsycINFO, & OVID Medline. Two reviewers independently reviewed and screened 268 papers. Papers that met inclusion criteria were quality assessed using The Critical Appraisal Skills Programme (CASP) qualitative studies checklist. The Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) checklist was used to guide the structure of the report.
Results
A thematic synthesis of 19 studies revealed six overarching themes which related to different aspects and features of the digital interventions: participants’ relationship with technology; the accessibility of the interventions; how the interventions could impact on individuals’ awareness and management of mental health; enhanced communication and relationships; and opportunities for reflection.
Conclusions
Benefits of using digital interventions are discussed. Areas for development and improvements are highlighted. Finally, recommendations for stakeholders who develop and implement digital interventions for psychosis are made.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Recent research has documented the potential benefits of digital interventions in overcoming barriers to accessing health care [1]. The term ‘digital intervention’ encompasses a wide range of interventions including mobile health (M-Health) interventions that can be delivered via a smartphone or mobile application, via websites or wearable devices, as well as through virtual reality or avatars [2,3,4,5,6].
Smartphone usage among people with psychosis is now at equivalent levels to the general population, with greater interest in developing digital interventions targeting psychosis [7,8,9]. Previous research has shown that digital interventions for people with psychosis are acceptable and can result in benefits including increased access to services, reduced stigma around receiving mental health treatment, and accommodating difficulties arising from cognitive impairments and/or low levels of motivation [10,11,12,13,14,15,16]. However, concerns about security and privacy when accessing support digitally have also been highlighted [17]. Although the growing interest in digital interventions for psychosis is promising, this literature is still relatively sparse in comparison to that concerning other mental health and physical health conditions [18,19,20].
Currently, qualitative research evaluating digital interventions are lacking in comparison with quantitative studies [21,22,23,24]. Existing reviews including qualitative insights have yielded important information regarding how people with psychosis engage with digital interventions [25, 26]. For example, digital interventions tailored to the individual increase the likelihood of people engaging, whilst severe mental health symptoms and technical issues serve as barriers to engagement [26]. It is worth highlighting that Bell et al. did not complete a systematic review of the literature, instead providing an overall synthesis of types of digital interventions and how these can support and benefit people with psychosis. Another review suggested that symptom monitoring and medication adherence tracking were useful features of digital interventions [25]. Although Batra et al. did complete a systematic review, the studies included were a mixture of quantitative or mixed method designs which were then presented through a narrative synthesis [25]. This highlights that previous reviews have provided valuable information, however they did not systematically capture the qualitative experiences of people with psychosis who have completed a specific digital intervention over an extended period of time. Qualitative studies enable us to get an in-depth understanding of participants’ experiences of interactions with, and attitudes and beliefs towards, a particular intervention or phenomenon. Gaining an increased understanding of the experiences of people with psychosis using digital interventions can ensure that they are meeting the needs of those using them and that they can be harnessed as a sustainable way of accessing support.
This review provides a synthesis of studies that adopted qualitative methods to examine the experiences of people with psychosis who have used digital interventions. It aims to provide a comprehensive understanding of how people with psychosis experience using digital interventions including features that may increase engagement and those that act as barriers. Further, it aims to answer the question, how do people with psychosis experience using digital interventions?
Methods
Design
This systematic review follows Cochrane guidance on conducting reviews and the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) guidelines [27, 28]. Specifically, the Cochrane guidance for qualitative evidence and the ENTREQ checklist were used to ensure that the review was conducted and reported appropriately [74, 75]. The PICOS framework (participants, interventions, comparators, outcomes, study design) was used to determine the eligibility criteria for study inclusion [29]. This review protocol was registered with PROSPERO, number CRD42022318723 (22/03/2022).
Inclusion criteria
Studies were included if they had participants who were adolescents and/or adults with psychosis. Studies were included if participants were reported as having severe mental illness (SMI). Studies exploring digital interventions or digitalized forms of assessment that are delivered via smartphone applications and/or web-based interventions that promote mental health, physical health and wellbeing were included. Studies that had qualitative elements which explored the potential effectiveness, usability and acceptability of digital interventions for people with psychosis were included. Only peer-reviewed studies were included.
Exclusion criteria
Studies were excluded if participants did not have a diagnosis of psychosis, this includes participants that were solely reported to have a diagnosis of bipolar disorder. Studies were excluded if they reported on digital interventions that were evaluating or developed for staff and/or carers of people with psychosis. Studies that reviewed digital interventions that purely provide consultation (telehealth) were not included. Studies that only used quantitative methods to evaluate a digital intervention and papers that report on study protocols were not included.
Search strategy, data screening and selection
The following databases were searched for this systematic review: PubMed, Embase, PsycINFO, & OVID Medline. Only articles that were published in English and were published between 1992 and October 2023 were included in the search.
Search terms related first to the population comprising Mental health OR Severe mental health OR Severe mental illness OR Psychosis OR Schizophrenia OR Voices OR Hallucinations. The second group of terms related to the digital technologies including Digital health interventions OR Digital interventions OR Digital treatment OR Mobile interventions OR Mobile treatment OR Mobile health applications OR Mobile health apps OR Smartphone OR Smartphone treatment OR Smartphone interventions OR Online treatment OR Online interventions OR Mhealth OR Ehealth. The third term related to experience of technologies including Experience OR User experience OR User perspective OR Engagement OR Satisfaction. The final term related to the methodology including Qualitative OR Interview OR Focus group OR Mixed methods.
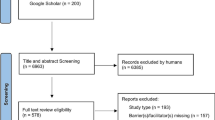
Titles and/or abstracts of studies retrieved using the search strategy were reviewed by the first author (SD) to identify studies that potentially met inclusion criteria. The second author (RP) reviewed the studies to check these decisions. Full texts of potentially eligible studies were retrieved and reviewed by the first author. At least 20% of these studies were independently screened by RP. Final decisions on papers to be included within the review were discussed between SD and RP following this independent review. Both reviewers (SD and RP) extracted data from the papers selected for inclusion in the review. Disagreements or discrepancies between the two reviewers at any stage of the screening and extraction process were resolved through discussion. An Excel spreadsheet was used to record the inclusion decisions and extracted data from the included studies for assessment of study quality. Data extracted from each of the included studies consisted of; aims of the study, ethical issues, study setting, theoretical background of study, sampling approach, participant characteristics, data collection, data analysis approach, key themes highlighted, and data related to the themes. Figure 1 presents the study selection process.

Study selection process
Assessment of study quality
The Critical Appraisal Skills Programme (CASP) qualitative studies checklist was used to assess the quality of the papers included in this review [30]. The first and second authors (SD and RP) independently assessed the quality of the studies before discussing the quality findings together and agreeing on the quality ratings of each paper. Each item was assigned a score, with ‘1’ indicating yes, and ‘0’ indicating either can’t tell or not addressed. Papers were then given a total score out of 10. Papers with a total score of 9 or above were categorised as being high quality, medium quality papers were those with a total score of 7 or 8, and papers with a total score of 6 or below were categorised as being low quality.
Data synthesis
The data from the selected studies were analysed using an inductive approach to thematic synthesis [31] in order to provide an understanding of the experiences of people with psychosis using digital interventions. The data synthesis for this current review followed the three stages of thematic synthesis; (1) Individual study findings were treated as raw data within the analysis. Each identified study was coded line by line in order to identify meaning in the data. (2) Codes from across the studies were reviewed together, and those with similar concepts were grouped together and given new, more descriptive names. (3) Final codes were grouped into broader, analytical themes.
Reflexivity statement
The first author is a White British, female Clinical Psychologist with experience of working clinically with people with psychosis including delivering psychological interventions such as Cognitive Behavioural Therapy for psychosis (CBTp) and Family Intervention for psychosis (FIp). The second author is a female research assistant with an Indian ethnic background who has worked in Early Intervention Psychosis services and Increasing Access to Psychological Therapies (IAPT) services. The remaining three authors are White British Female (PG and CE), and White British Male (AG), all experienced clinical psychology researchers, specializing in working clinically with people with psychosis, developing treatment approaches, including CBTp and digitally supported interventions, and new services. All authors have strong interests in understanding the perceptions and experiences of people who experience psychosis in order to enhance the quality of treatment. As such, the epistemological position of the authors in this review is most closely aligned to a “critical realist” perspective [32].
Results
Assessment of study quality
Fifteen out of the nineteen studies were rated as high quality, with a score of 9 or above [12, 33,34,35,36,37,38,39,40,41,42,43,44,45,46]. The rest of the studies were rated as moderate quality, scoring either 7 or 8 [14, 47,48,49]. None of the included studies were rated as low quality (scoring 6 or below). Scores on individual items for all included studies can be found in Table 1. In all of the studies, there was a clear statement of aims, and the methods were deemed appropriate to address these aims. For five of the studies, the method used to analyse the data was stated, however a more detailed reporting of the steps used to analyse the qualitative data was not clearly stated [14, 42, 43, 47, 49]. The item that was scored most poorly across the included studies was in relation to reflexivity and bias. Only seven out of the nineteen studies had a clear reflexivity statement or explanation of the researchers’ relationship with the participants [12, 33, 34, 39, 42, 44, 45].
Thematic synthesis
After screening 407 records that were identified in the search, 19 studies were found to meet the inclusion criteria for the thematic synthesis (see Fig. 1).The number of participants across the studies ranged from 6 to 95 (M = 22.5). The mean ages of the participants ranged from 20 to 55yrs across the studies. In total, 54.1% of the participants across all of the studies were male, 45.7% were female, and 0.2% were transgender. The ethnicity of participants was not reported in 6 out of the 15 studies. In studies that did report on ethnicity, between 42.1 and 100% of participants were White. 10 out of 15 studies used a mixed-method design, with the remaining four employing only qualitative methods. Further information on the included studies are detailed in Table 2. The synthesis resulted in six overarching themes and sixteen sub-themes (Table 2). The six themes were: (1) Content of digital intervention, (2) relationship with technology, (3) accessibility, (4) awareness and management of mental health, (5) enhancing communication and relationships, and (6) opportunity for reflection. A thematic map describing the themes and sub-themes can be found in Fig. 2 (Table 3).

Thematic map of themes and sub-themes
(1) Content of digital intervention
This theme relates to specific features of the digital interventions that participants found helpful and unhelpful, and also suggestions on how the content of the digital intervention could be improved. This theme is comprised of three subthemes: (I) tailoring to specific needs, (II) views on notifications/reminders, and (III) range of content. For participants, having interventions that felt meaningful to their experiences as well as feeling they can trust the information within interventions are important for motivation and longevity of use. Notifications received through interventions can be helpful, encouraging engagement when it fits within daily routines and other activities. When notifications are inaccurate, causing additional stress, they can reduce people’s willingness or motivation to use the intervention. This may lead to participants ignoring notifications which could impact on long term usage or effectiveness of interventions. When tasks feel mundane or participants no longer feel they are able to learn new skills, interest in or motivation to use interventions may decrease. There, however, needs to be a balance between feeling challenged with learning new skills, however not having content that is too challenging which could cause people to feel overwhelmed or deskilled. Providing solution focused interventions can help participants to feel good and think more positively about the intervention, ensuring that it feels like a positive addition to their lives.
-
(I)
Tailoring to specific needs
Being able to customise and tailor interventions to individual needs was reported as an important feature. This included being able to see visual representations of their own experiences, personalising reminders, and having the option to write qualitative feedback [33, 35, 40, 43, 46,47,48]. ‘’I would've changed my prompts to check in with my sleep’’ [p.6, 47]. Participants reported difficulty using interventions in instances where the content was hard for them to relate to, or when there were concerns related to the accuracy of data recorded in the intervention [36, 37, 43, 47]. ‘’Hard to relate to the content, mostly for teenagers (had to put examples to my own context)’’ [Participant 6, Suppl material, 48].
-
(II)
Views on notifications/reminders
Notifications and reminders were consistently reported as helping participants to complete tasks such as remembering to take medication, or feeling supported when receiving positive messages [12, 33,34,35,36, 45, 47]. ‘’most participants in both groups commented on the overall positive tone of the apps and how this was a necessary attribute to maintain their engagement over time’’ [p. 9, 36]. Negative views associated with notifications and reminders included receiving too many prompts, timing inaccuracies, and receiving false alarms on potential relapses [14, 33, 39, 47]. ‘’Overall, 5 participants commented on how they would have concerns over false alarms—for example, whether sleeping poorly in the absence of deterioration in symptoms would trigger a response’’ [p. 8, 39].
-
(III)
Range of content
The content range of interventions were reported to be too limited, with participants expressing a need for the content to be broader and to have more options. This was especially the case after a sustained period of continued use, which could be seen as repetitive over time [33, 39, 44,45,46,47,48]. ‘’..I found content on the actual app was too limited..” [Participant 128, p.1078, 14]. Participants also commented on positive aspects of the intervention content including finding it enjoyable answering questions, the overall supportive tone, and having more solution-focused content [34, 38, 44, 47]. ‘’Audrey identified the positive environment on Horyzons as an important element of her high usage level. She did not want to spend time at a place where “the people are all negative” [p. 7, 44].
(2) Relationship with technology
This second theme is comprised of three subthemes which include participants’ views on technology and their previous experiences of using technology. These were (I) experience of technology, (II) concerns about technology, and (III) technical issues. Existing experience or views about technology could impact on people’s initial willingness or ability to use interventions, however these views can be altered through support from others and with increased familiarity. Having a lack of experience using technology could increase feelings of disempowerment, disconnection and confidence. This could mean that participants do not experience the full benefits that such technology could offer. Technology could impact or interact with pre-existing concerns about monitoring and therefore impact on paranoia. The way in which tracking or monitoring is perceived could impact on how attitudes towards interventions which could be negative or create a sense of safety from knowing others may be supporting from afar.
-
(I)
Experience of technology
A lack of experience using technology was cited as a reason why participants found it difficult to engage with an intervention, however for some, this improved over time [33,34,35, 46]. ‘’..the rest of us never had a smartphone. I think a class on how to use it would be helpful’’ [Participant 6, p.10, 40]. For others, this lack of experience could restrict their interaction with the intervention and affect their motivation to use it, or in some cases, result in them discontinuing their use [12, 34, 35, 38, 43]. ‘’Lack of smartphone experience was a barrier in some cases, with 1 participant accidentally deleting the app from the phone and 2 others commenting that their lack of smartphone experience prevented them from accessing the app's extra features’’ [p. 17, 34].
Receiving training and/or support with using the intervention was, in some instances, helpful and enabled people to continue using it even after experiencing initial difficulties. However, limited access to the internet could cause some participants to continue experiencing difficulties in engaging [33, 40, 43, 45]. ‘’watching the videos at home supported the information to “sink in” for Viv. Participants who had no or limited Internet access at home due to reception, accommodation, or financial difficulties, did not have this opportunity’’ [p. 8, 45].
-
(II)
Concerns about technology
Concerns about technology, specifically with privacy and access to data were raised across a number of studies [33,34,35, 37,38,39, 44]. Some participants reported experiencing feelings of paranoia about being monitored or concerns that others would be able to see the content of the intervention whilst using it in public [12, 34, 39, 46]. ‘’It's difficult for me … yeah I always felt a bit of conscious somebody might be coming along and looking over your shoulder'' [Participant S8, p. 690, 12]. For others, being monitored or tracked by therapists was seen as a positive, leading them to feel safe and supported [33, 43]. ‘’participants were positive about the therapist being able to track how they were doing’’ [p. 947, 33]. Receiving further information regarding privacy settings and confidentiality was reported to help participants feel more comfortable engaging with the technology and disclosing their personal experiences [38, 48]. ‘’most participants liked the inclusion of terms and conditions that outlined the privacy settings and rules of use to alleviate potential concerns around engaging with the social network’’ [p. 10, 38].
-
(III)
Technical issues
Technical issues associated with the digital interventions were reported in a number of studies including reduced battery life, compatibility issues, difficulty navigating apps, or connecting to Bluetooth [33,34,35,36, 40, 43, 47, 48]. ‘’Just the amount of work you had to do to get a quick reminder of what you wanna do […] you'd have to go through quite a bit just to get to the section that you want’’ [Participant 3, p.729, 43]. Experiencing such difficulties caused some participants to feel discouraged and frustrated having to spend time to fix them [40]. ‘’It was kind of a pain in the neck so I got discouraged with that. It wasn’t the phone; it was because I didn’t know the phone.” [p. 9, 40].
(3) Accessibility
The third theme relates to how easy digital interventions are to use, as well as the opportunity for quicker access to support and being able to assist with potential physical and cognitive impairments. This theme is comprised of two subthemes; (I) easily accessible, and (II) supporting with cognitive/physical difficulties. Having a therapists support in their pocket could be a particularly useful aspect of digital interventions for people with psychosis who may have found it more difficult to access or trust services, and feel able to ask for help. Having symptoms readily recorded within interventions make it easier to recall information to not only share with others, but also in helping to remember experiences they had in the past. This provided participants with more opportunities to learn without having to rely on memory. Being sensitive to literacy and other individual needs is important to ensure that people feel supported and not made to feel that interventions are still inaccessible.
-
(I)
Easily accessible
Participants reported the digital nature of the intervention meant they were able to access this at any time in a range of situations and settings, easily fitting into their daily routine [12, 14, 33,34,35, 38, 40, 43,44,45, 47, 48]. ‘’Every day if I go out, I always do what I need to do on it, like take my deep breaths and get me encouraged to go out… that phone is always with me when I’m out. If I stop, I use it as well’’ [Participant L16, p. 689, 12]. Participants reported feeling safer and more supported due to having easy access to healthcare professionals, or through access to coping strategies [12, 35,36,37,38, 42, 46, 48]. ‘’Individuals noted that they felt safer or more secure both in regards to their physical safety and in terms of receiving support for mental health issues quickly and easily’’ [p. 8, 35]. Access to, and integration of digital interventions within the routine care that participants were receiving was reported as a key recommendation for future interventions [47].
-
(II)
Supporting with cognitive/physical difficulties
Having a device with them at all times was reported as beneficial for a number of participants who reported difficulties with their memory [40, 44, 45]. ‘’one doesn’t have to sit there and make an effort to remember what to say’’ [p. 946, 33]. Real-time documentation of experiences meant they could record how they were feeling at that time rather than having to rely on their memory, which was particularly useful when experiencing acute symptoms [33, 34, 47]. ‘’Like for me when I was talking about my illness, the more I got ill, the more I couldn’t remember’’ [p. 16, 34].
For participants with lower literacy levels, completing more challenging tasks was reported to be difficult and a barrier to fully engaging with the intervention [34, 38, 43, 48]. Suggestions such as having more visual components or gamifying certain aspects of the intervention was reported to help make it more accessible [48]. ‘’Most effective method is videos’’ [Participant 5, Suppl material, 48]. Recommendations were also made for adaptations for people with visual or hearing impairments, especially for interventions which were delivered on smaller screens [12, 35, 47]. ‘’A way for hearing and vision impaired veterans to be able to use the app’’ [p. 8, 47].
(4) Awareness and understanding of mental health
This fourth theme is comprised of three subthemes which include participants' increased insight and understanding of their mental health as well as the impact this had on their self-management behaviours and feelings towards the management of their mental health. These were; (I) increased insight, (II) self-management, and (III) feelings of empowerment. Having increased insight into their mental health helped participants to feel more in touch with their own experiences and feel that they, and others can be better equipped to manage their symptoms. This increases confidence in themselves and others in noticing or intervening at times when relapse may be more likely, therefore taking more control of their mental health rather than it feeling like it is controlling them. Increased symptoms however could interact and impact on participants’ sense of connection towards the intervention and their sense of ability in managing them. At these times, providing participants with additional support in using the intervention could help to increase engagement with it and build hope, confidence and increased skills.
-
(I)
Increased insight
Gaining an increased awareness of symptoms and mood was reported as a key benefit of the digital interventions [12, 14, 33,34,35,36,37,38, 40, 46, 47]. Understanding the links between symptoms, mood and behaviour, as well as being able to identify factors that could impact mood and symptoms was deemed helpful [33, 34, 36, 38]. ‘’It (the app) has made me more conscious of myself and of what has caused me to feel down and what causes me to feel better’’ [p. 947, 33]. Such information was also reported to be helpful for care providers who could gain an increased insight into the mental health experiences of those they support [33, 45, 46].
Participants reported being able to use the digital interventions to learn new coping strategies and ways to keep well [12, 40, 44, 45]. Information collected over time helped participants to identify factors that could increase the likelihood of relapse [34, 39]. ‘’11 felt that sleep monitoring could be a successful strategy for the early detection of relapse’’ [p. 8, 39]. Reduced levels of engagement with the digital intervention were reported to be useful in indicating relapses [34, 39].
-
(II)
Self-management
Mood and symptom monitoring was reported as useful for being able to better manage symptoms [14, 33, 34, 44, 46, 47]. Having access to resources and strategies enabled participants to support their mental health such as through adhering to medication, or being able to test negative thoughts, voices and paranoid beliefs [12. 34, 35, 37, 47]. ‘’you become your own therapist and that’s what CBT is about, being able to change your behaviour … reassess a situation, about going forward on your own, uhm solution.” [p. 1078, 14]. Participants reported that a variety of symptoms could impact their ability to self-manage, including both negative and positive symptoms increasing the length of time it took to respond to the intervention, or increasing their avoidance of it [12, 33, 34, 44]. ‘’Several participants described how low mood, negative symptoms, and poor motivation could at times lead them to avoid interacting with the mHealth solution’’ [p. 948, 33]. Factors such as social anxiety and internalised stigma impacted on engagement and therefore on participants ability to engage in self-management behaviours [44].
-
(III)
Feelings of empowerment
Participants reported feeling empowered, motivated, proud and more in control of their mental health as a result of the digital interventions [12, 14, 36, 39 40, 42, 44, 45]. ‘’I think with it being on the phone it’s in your hands a little, it’s under your control a bit more, as opposed to feeling a bit like you’re under house arrest” [p. 1078, 14]. This helped participants to feel uplifted, happier and more able to engage in day-to-day activities [35, 45, 46, 49]. Engaging in the digital interventions also enabled participants to build their confidence in using coping skills and their own recovery [12, 14, 43, 45,46,47]. This impacted on participants’ feelings of hope for the future, and for some, reduced feelings of shame, helplessness, and suicidality [42, 45]. ‘’Helped reduce suicidality primarily through instilling some level of hope’’ [p. 1016, 42].
(5) Enhancing communication and relationships
In this fifth theme participants’ experiences of feeling understood, connected and better able to communicate with others are discussed. This theme is comprised of three subthemes; (I) feeling understood, (II) increased connection, and (III) facilitating communication. Digital interventions were felt to strengthen existing relationships with professionals through feeling their experiences are understandable, and increased confidence that they can be effectively supported. Reducing feelings of loneliness in relation to their experiences helped to increase feelings of community, knowing that others experience similar things, which may not be as easily accessed in more traditional forms of support. Being supported by a community, as well as supporting others could increase feelings of being cared for, but also may provide people with skills and confidence in helping others and using their experiences to empower themselves and others. Having this community or a sensed need to support others could however result in some feeling pressured to help which could be particularly difficult for those who find interacting with others hard. Knowing what to bring to meetings with professionals may have been a difficult for people in traditional interventions, however with digital interventions participants could more easily instigate conversations and make be open about experiences. This also enabled conversations with families whereby previously it felt difficult to do so.
-
(I)
Feeling understood
Participants reported feeling understood using the digital intervention either due to interactions with a therapist or researcher, others who have experienced psychosis, or just due to the overall understanding and support tone [12, 14, 33, 38, 43, 44, 48]. ‘’many participants continued to perceive both apps as positive and supportive and noted that this was a strength of the apps’’ [p. 9, 36]. This helped participants feel cared and looked out for, which for some enhanced therapeutic relationships [12, 33, 36, 38]. The digital interventions themselves helped participants to recognise that other people also struggle with their mental health, either through being able to interact with peers in the intervention or just as a result of there being an intervention for psychosis [12, 34, 35, 38, 42, 44, 45]. ‘’to be able to see that there were other people out there struggling just as much as I was, or were struggling just as much as I was…was quite helpful’’ [p. 6, 45]. This helped participants to feel less alone and their experiences normalised [12, 34, 38, 42, 44, 45].
-
(II)
Increased connection
The digital interventions increased feelings of connection for participants, through feeling connected with peers, with the person who was accessing their data, and to something bigger [12, 34,35,36,37,38, 42, 44, 49]. ‘’Many expressed that they could relate to others and both understand and feel understood’’ [p. 5, 44]. Having the opportunity to connect with others with shared experiences meant that participants could relate to others and create an environment of reciprocal sharing and support [44,45,46].
Having easy access to the digital interventions meant that participants could connect with others anywhere they were, which reduced feelings of stigma and loneliness, as well as increased confidence in social situations and feelings of empowerment to support others [12, 35, 38, 44, 45, 48, 49]. ‘’I think I feel a lot more confident in myself… I think prior to it I was a bit, not shy, but a bit hesitant in social situations’’ [p. 883, 49]. However, for some, connecting with others also led participants to feel a sense of responsibility to support others and tiredness from the pressure of offering peer support [36, 44, 45]. ‘’…some people don’t like talking to people like, you know, sometimes you don’t want to talk to people about stuff you might just prefer to deal with an app’’ [Participant 10, p. 728, 43].
-
(III)
Facilitating communication
The digital interventions were reported by participants to facilitate communication with professionals either by using information or data stored in the intervention to help bring up certain topics or to help identify areas for discussion [12, 33,34,35, 37, 45]. ‘’It keeps me in contact with my mental health professionals out in the community, so it helps [us to] communicate when there is no physical presence’’ [p. 8, 35]. Participants also reported that digital interventions provided them with an easier way to communicate with other people who experience psychosis, and also with their loved ones [39, 44, 49]. The online platform was reported by participants to feel easier and a less threatening means of communicating and opening up about their experiences [34, 35, 43, 45]. ‘’it’s in the privacy of your own home…So there’s no judgement, there’s no judgement of who you are or what you've been’’ [p. 8, 45].
(6) Opportunity for reflection
The sixth and final theme is comprised of two subthemes which include digital interventions enabling participants to think and reflect on their mental health, including their ideas on recovery. These were (I) space to reflect, and (II) recovery. Interventions provided participants to stop to pause and notice their experiences. Having experiences or symptoms recorded enabled participants to see these and provide space to rationalise them, providing a broader picture of their experiences. Participants may have previously not had access to references of recovery and how the future may look for them, however the interventions helped to provide a sense of recovery being something that is tangible and realistic.
-
(I)
Space to reflect
The digital interventions included in the reviewed studies were reported by many participants to provide a space to think and reflect on their mental health experiences, either through reviewing daily symptom diaries, hearing others' experiences, or through discussion with clinicians [12, 33, 34, 39, 44,45,46,47, 49]. Reflecting on previous and current mental health experiences through accessing data and symptom diaries was reported by some to enable them to look at their experiences from a more objective perspective [33, 34]. ‘’It can be a good thing to just keep an eye on how things are going because it can be a bit like... inside one’s head it’s going splendidly, and then in reality one’s been... (...) or vice versa, if you’re feeling really low but then you realize that... okay, this past week has actually been good’’ [p. 947, 33].
-
(II)
Recovery
Access to information about their own experiences, as well as the experiences of others within the digital interventions was reported by participants to be helpful in getting them to learn and reflect on the meaning of recovery for themselves and others, including increasing beliefs that recovery is possible [12, 34, 36, 45]. ‘’Afterwards I’d just be like “I can get better. I can get better!” there was just, there was this hope that I had when I was using it’’ [p. 16, 34].
Discussion
This systematic review adds to the limited body of qualitative literature exploring the experiences of people with psychosis using digital interventions. We constructed six themes which showed that the use of digital interventions for psychosis can have a number of benefits, which could be enhanced in existing and future interventions. Some of the findings highlighted across these themes are consistent with reviews both within people with psychosis, but also amongst non-psychosis populations. Specifically, findings related to experiences of technical challenges, concerns regarding privacy and confidentially, a need for training and guidance, as well as interventions being able to enhance therapeutic relationships and provide people with opportunities to learn new skills and connect with others [25, 26, 77,78,79].
Increasing self-management of symptoms in psychosis is a key feature of digital interventions which can have a positive impact on medication adherence, and also on an individual’s sense of agency over their own symptoms [50]. Enhancing control of their own mental health was reported in the current review as increasing feelings of empowerment and confidence in coping on a day-to-day basis. Empowerment has been identified as one of the key components within recovery, and is particularly important for psychosis populations who are more likely to face disempowering situations [51, 52].
Digital interventions enhancing self-reflection emerged as another theme. Such self-reflection may be helpful in addressing cognitive biases e.g. jumping to conclusions which have been found to be a factor in the onset and maintenance of psychosis [53]. Digital interventions were also reported to help normalise experiences related to psychosis. This process of normalisation can help to reduce stigma in a population that experiences significant rates of stigmatisation compared to other mental health conditions [54]. Further, peer support has been found to have numerous benefits for people with psychosis, including increased feelings of hope, empowerment, optimism and reducing feelings of social isolation and fears of judgement situations [52, 55,56,57]. Having the option to access peer support and increase connections with others is an important feature of digital interventions and confers many benefits for those using them.
The ability to customise an intervention and receive notifications or reminders was valued. However, study participants also reported on the limited nature of content which could be repetitive over time. Therefore, to ensure longevity of engagement with digital interventions, it may be important to ensure that there is a varied and wide range of content and that individuals have the option to customise the intervention to make it specific to their individual needs. This could help to integrate such interventions into individuals’ everyday lives, which was also reported as beneficial in the current and previous reviews [17, 26].
Easy access to support in daily life could be particularly useful for people with psychosis where there is an increased prevalence of cognitive difficulties [58, 59]. It is also worth considering literacy levels as studies have revealed that these tend to be lower in people with psychosis compared to the general population [60, 61]. Having interventions which are too challenging could create barriers to access as well as increase feelings of shame and stigma, which would likely impact on levels of engagement. Previous research that developed digital interventions with this in mind found that engagement was high and cognitive ability did not impact on participants’ use of the intervention [62].
Consistent with other findings, some of the participants in the reviewed studies reported a lack of experience in using technology limiting engagement with the digital intervention [63, 64]. Compared to the general population, people with psychosis were twice less likely to have foundation or life skills in using digital technology [65]. The opportunity to access training in order to increase confidence and skills in using technology has been suggested as a way to increase accessibility and reduce the digital divide that continues to exist for people with psychosis [64,65,66]. Further, the use of blended approaches whereby therapists provide support to people whilst using digital interventions has also been found to increase engagement and confidence in using technology [12, 17, 67].
In line with other studies, participants in the reviewed studies raised concerns regarding privacy and worries about being monitored [26, 68]. Participants also reported experiencing technical issues which could cause feelings of frustration, and at times, increased paranoid ideation, which could impact on future engagement. It is worth noting however that raising concerns about, or trust in technology is not mutually exclusive with symptoms such as paranoia and is a consideration in the wider context of digital health care [69] These findings therefore highlight two important points when implementing digital interventions. Firstly, it is crucial to have easy access to ongoing support in order to overcome any technical issues when they arise to reduce disengagement. Secondly, ensuring that individuals using digital interventions are provided with a full explanation and information regarding who can access their data, and the reasons why it is being accessed is vital.
The findings of this review should be considered in the context of the methods in which it was conducted and its limitations. As with all qualitative syntheses, the review is reliant on an analysis of secondary data which was originally generated from different theoretical underpinnings and data analysis methods [70]. People from global majority backgrounds are disproportionately represented within psychosis populations [71,72,73]. Despite this, there was a lack of reporting of ethnicity in some of the reviewed studies, and in studies that did report on it, the majority of participants identified as White. Therefore, research that reports, and includes people from global majority backgrounds is important to ensure their needs and experiences are represented. The studies within this review explored a wide variety of digital interventions, however the thematic synthesis did not examine potential differences between specific types of digital interventions. This may be useful to investigate in future qualitative reviews as it may highlight specific experiences based on the type of digital intervention used.
The current review was conducted and reported in line with PRISMA guidelines [28]. It is worth nothing, however, that a confidence assessment was not completed as recommended in these guidelines e.g. the GRADE-CERQual approach [76]. Although such assessments have previously been confused with assessments of quality, they are separate and distinct assessments which should be considered in future qualitative systematic reviews [76]. Finally, four different databases were used in order to identify a range of peer-reviewed literature for the review. These databases have been found to be robust in identifying relevant studies for reviews [80]. Research has found that the CINAHL database could also be good source of primary studies in qualitative research and therefore it is recommended that future reviews use this as one of the databases within their search strategy [81]. The current review used a modified version of the PICO, the PICOS, which has been found to be more sensitive to study design and therefore useful in removing irrelevant studies when conducting qualitative systematic reviews [82]. The SPIDER tool has also been recommended for qualitative studies, however research has found the SPIDER may not be as robust as the PICO/PICOS frameworks [29]. Further, the PerSPEcTIF, is another tool developed for qualitative studies however this has not yet been robustly compared against other, more well-established frameworks [83].
The themes in this review can inform stakeholders involved in the development and implementation of digital interventions for people with psychosis. This includes healthcare policy makers, service commissioners, healthcare professionals, and those involved in research. Digital interventions for people with psychosis have a number of benefits for users such as gaining an increased understanding of their experiences, improving self-management of symptoms, and feeling more connected to others. All of these benefits have positive impacts on feelings of empowerment which is an important component of recovery in psychosis and have all been highlighted in this review. However, for those developing and implementing digital interventions for people with psychosis, there is a need to ensure that such interventions are accessible for the population. This includes providing sufficient training and ongoing support to ensure that people with psychosis do not continue to experience a digital divide and can access effective mental health care.
Data Availability
No datasets were generated or analysed during the current study.
References
Lattie EG, Stiles-Shields C, Graham AK (2022) An overview of and recommendations for more accessible digital mental health services. Nat Rev Psych 1:87–100. https://doi.org/10.1038/s44159-021-00003-1
Polillo A, Voineskos AN, Foussias G, Kidd SA, Sav A, Hawley S, Soklaridis S, Stergiopoulos V, Kozloff N (2021) Using digital tools to engage patients with psychosis and their families in research: survey recruitment and completion in an early psychosis intervention program. JMIR Ment Health 8(5):e24567. https://doi.org/10.2196/24567
Lyons EJ, Swartz MC, Lewis ZH, Martinez E, Jennings K (2017) Feasibility and acceptability of a wearable technology physical activity intervention with telephone counseling for mid-aged and older adults: a randomized controlled pilot trial. JMIR Mhealth Uhealth 5(3):e28. https://doi.org/10.2196/mhealth.6967
Smuck M, Odonkor CA, Wilt JK, Schmidt N, Swiernik MA (2021) The emerging clinical role of wearables: factors for successful implementation in healthcare. Npj Dig Med 4:1–8. https://doi.org/10.1038/s41746-021-00418-3
Geraets CNW, Snippe E, van Beilen M, Pot-Kolder RMCA, Wichers M, van der Gaag M, Veling W (2020) Virtual reality based cognitive behavioral therapy for paranoia: effects on mental states and the dynamics among them. Schizophr Res 222:227–234. https://doi.org/10.1016/j.schres.2020.05.047
Craig TK, Rus-Calafell M, Ward T, Leff JP, Huckvale M, Howarth E, Emsley R, Garety PA (2018) AVATAR therapy for auditory verbal hallucinations in people with psychosis: a single-blind, randomised controlled trial. Lancet Psychiatry 5(1):31–40. https://doi.org/10.1016/S2215-0366(17)30427-3
Firth J, Cotter J, Torous J, Bucci S, Firth JA, Yung AR (2016) Mobile phone ownership and endorsement of “mHealth” among people with psychosis: a meta-analysis of cross-sectional studies. Schiz bull 42(2):448–455. https://doi.org/10.1093/schbul/sbv132
Young AS, Cohen AN, Niv N, Nowlin-Finch N, Oberman RS, Olmos-Ochoa TT, Goldberg RW, Whelan F (2020) Mobile phone and smartphone use by people with serious mental illness. Psychiatr Serv 71(3):280–283. https://doi.org/10.1176/appi.ps.201900203
Rus-Calafell M, Schneider S (2020) Are we there yet?!-a literature review of recent digital technology advances for the treatment of early psychosis. Mhealth. https://doi.org/10.21037/mhealth.2019.09.14
Berry N, Machin M, Ainsworth J, Berry K, Edge D, Haddock G, Lewis S, Morris R, Bucci S (2020) Developing a theory-informed smartphone app for early psychosis: learning points from a multidisciplinary collaboration. Front Psych 11:602861. https://doi.org/10.3389/fpsyt.2020.602861
Fortuna KL, Brooks JM, Umucu E, Walker R, Chow PI (2019) Peer support: a human factor to enhance engagement in digital health behavior change interventions. J Techn Behav Sci 4(2):152–161. https://doi.org/10.1007/s41347-019-00105-x
Greenwood KE, Gurnani M, Ward T, Vogel E, Vella C, McGourty A, Robertson S, Sacadura C, Hardy A, Rus-Calafell M, Collett N, Emsley R, Freeman D, Fowler D, Kuipers E, Bebbington P, Dunn G, Michelson D, Garety P, Involvement SPP, (PPI) team, (2022) The service user experience of SlowMo therapy: a co-produced thematic analysis of service users’ subjective experience. Psych Psychother 95(3):680–700. https://doi.org/10.1111/papt.12393
Hardy A, Wojdecka A, West J, Matthews E, Golby C, Ward T, Lopez ND, Freeman D, Waller H, Kuipers E, Bebbington P, Fowler D, Emsley R, Dunn G, Garety P (2018) How inclusive, user-centered design research can improve psychological therapies for psychosis: development of SlowMo. JMIR Ment Health 5(4):e11222. https://doi.org/10.2196/11222
Bucci S, Barrowclough C, Ainsworth J, Machin M, Morris R, Berry K, Emsley R, Lewis S, Edge D, Buchan I, Haddock G (2018) Actissist: proof-of-concept trial of a theory-driven digital intervention for psychosis. Schizo Bull 44(5):1070–1080. https://doi.org/10.1093/schbul/sby032
O’Hanlon P, Aref-Adib G, Fonseca A, Lloyd-Evans B, Osborn D, Johnson S (2016) Tomorrow’s world: current developments in the therapeutic use of technology for psychosis. BJPsych Adv 22:301–310. https://doi.org/10.1192/apt.bp.115.014654
Proudfoot J (2013) The future is in our hands: The role of mobile phones in the prevention and management of mental disorders. Aust N Z J Psychiatry 47(2):111–113. https://doi.org/10.1177/0004867412471441
Aref-Adib G, McCloud T, Ross J, O’Hanlon P, Appleton V, Rowe S, Murray E, Johnson S, Lobban F (2019) Factors affecting implementation of digital health interventions for people with psychosis or bipolar disorder, and their family and friends: a systematic review. Lancet Psychiatry 6(3):257–266. https://doi.org/10.1016/S2215-0366(18)30302-X
Chan A, De Simoni A, Wileman V, Holliday L, Newby CJ, Chisari C, Ali S, Zhu N, Padakanti P, Pinprachanan V, Ting V, Griffiths CJ (2022) Digital interventions to improve adherence to maintenance medication in asthma. Cochrane Database Syst Rev 6(6):CD013030. https://doi.org/10.1002/14651858.CD013030.pub2
Morton K, Dennison L, May C, Murray E, Little P, McManus RJ, Yardley L (2017) Using digital interventions for self-management of chronic physical health conditions: a meta-ethnography review of published studies. Patient Educ Couns 100(4):616–635. https://doi.org/10.1016/j.pec.2016.10.019
Rose T, Barker M, Maria Jacob C, Morrison L, Lawrence W, Strömmer S, Vogel C, Woods-Townsend K, Farrell D, Inskip H, Baird J (2017) A systematic review of digital interventions for improving the diet and physical activity behaviors of adolescents. J Adolesc Health Off Publ Soc Adolesc Med 61(6):669–677. https://doi.org/10.1016/j.jadohealth.2017.05.024
Ben-Zeev D, Brenner CJ, Begale M, Duffecy J, Mohr DC, Mueser KT (2014) Feasibility, acceptability, and preliminary efficacy of a smartphone intervention for schizophrenia. Schizophr Bull 40(6):1244–1253. https://doi.org/10.1093/schbul/sbu033
Velligan D, Mintz J, Maples N, Xueying L, Gajewski S, Carr H, Sierra C (2013) A randomized trial comparing in person and electronic interventions for improving adherence to oral medications in schizophrenia. Schizophr Bull 39(5):999–1007. https://doi.org/10.1093/schbul/sbs116
Skivington K, Matthews L, Simpson SA, Craig P, Baird J, Blazeby JM, Boyd KA, Craig N, French DP, McIntosh E, Petticrew M, Rycroft-Malone J, White M, Moore L (2021) A new framework for developing and evaluating complex interventions: update of medical research Council guidance. BMJ 374:n2061. https://doi.org/10.1136/bmj.n2061
Tong A, Palmer S, Craig JC, Strippoli GF (2016) A guide to reading and using systematic reviews of qualitative research. Nephrol Dial Transplant Off Publ Eur Dial Transplant Assoc Eur Renal Assoc 31(6):897–903. https://doi.org/10.1093/ndt/gfu354
Batra S, Baker RA, Wang T, Forma F, DiBiasi F, Peters-Strickland T (2017) Digital health technology for use in patients with serious mental illness: a systematic review of the literature. Med Devices 10:237–251. https://doi.org/10.2147/MDER.S144158
Bell I, Pot-Kolder RMCA, Wood SJ, Nelson B, Acevedo N, Stainton A, Nicol K, Kean J, Bryce S, Bartholomeusz CF, Watson A, Schwartz O, Daglas-Georgiou R, Walton CC, Martin D, Simmons M, Zbukvic I, Thompson A, Nicholas J, Alvarez-Jimenez M et al (2022) Digital technology for addressing cognitive impairment in recent-onset psychosis: a perspective. Schizophr Res Cogn 28:100247. https://doi.org/10.1016/j.scog.2022.100247
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (2022) Cochrane Handbook for Systematic Reviews of Interventions, Version 6.3. Retrieved from: https://training.cochrane.org/handbook
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 6(7):e1000100. https://doi.org/10.1371/journal.pmed.1000100
Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S (2014) PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res 14:579. https://doi.org/10.1186/s12913-014-0579-0
Ma LL, Wang YY, Yang ZH, Huang D, Weng H, Zeng XT (2020) Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: what are they and which is better? Mil Med Res 7(7):1–11. https://doi.org/10.1186/s40779-020-00238-8
Thomas J, Harden A (2008) Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 8:45. https://doi.org/10.1186/1471-2288-8-45
Fletcher AJ (2017) Applying critical realism in qualitative research: methodology meets method. Int J Soc Res Methodol 20(2):181–194. https://doi.org/10.1080/13645579.2016.1144401
Austin SF, Frøsig A, Buus N, Lincoln T, von Malachowski A, Schlier B, Frost M, Simonsen E (2021) Service user experiences of integrating a mobile solution (IMPACHS) into clinical treatment for psychosis. Qual Health Res 31(5):942–954. https://doi.org/10.1177/1049732320986556
Eisner E, Bucci S, Berry N, Emsley R, Barrowclough C, Drake RJ (2019) Feasibility of using a smartphone app to assess early signs, basic symptoms and psychotic symptoms over six months: a preliminary report. Schizophr Res 208:105–113. https://doi.org/10.1016/j.schres.2019.04.003
Forchuk C, Reiss JP, O’Regan T, Ethridge P, Donelle L, Rudnick A (2015) Client perceptions of the mental health engagement network: a qualitative analysis of an electronic personal health record. BMC Psychiatry 15:250. https://doi.org/10.1186/s12888-015-0614-7
Gowarty MA, Longacre MR, Vilardaga R, Kung NJ, Gaughan-Maher AE, Brunette MF (2021) Usability and acceptability of two smartphone apps for smoking cessation among young adults with serious mental illness: mixed methods study. JMIR Ment Health 8(7):e26873. https://doi.org/10.2196/26873
Kidd SA, Feldcamp L, Adler A, Kaleis L, Wang W, Vichnevetski K, McKenzie K, Voineskos A (2019) Feasibility and outcomes of a multi-function mobile health approach for the schizophrenia spectrum: App4Independence (A4i). PLoS ONE 14(7):e0219491. https://doi.org/10.1371/journal.pone.0219491
Klein P, Lawn S, Tsourtos G, van Agteren J (2019) Tailoring of a smartphone smoking cessation App (Kick.it) for serious mental illness populations: qualitative study. JMIR Hum Factors 6(3):14023. https://doi.org/10.2196/14023
Meyer N, Kerz M, Folarin A, Joyce DW, Jackson R, Karr C, Dobson R, MacCabe J (2018) Capturing rest-activity profiles in schizophrenia using wearable and mobile technologies: development, implementation, feasibility, and acceptability of a remote monitoring platform. JMIR Mhealth Uhealth 6(10):e188. https://doi.org/10.2196/mhealth.8292
Naslund JA, Aschbrenner KA, Bartels SJ (2016) Wearable devices and smartphones for activity tracking among people with serious mental illness. Ment Health Phys Act 10:10–17. https://doi.org/10.1016/j.mhpa.2016.02.001
Palmier-Claus JE, Rogers A, Ainsworth J, Machin M, Barrowclough C, Laverty L, Barkus E, Kapur S, Wykes T, Lewis SW (2013) Integrating mobile-phone based assessment for psychosis into people’s everyday lives and clinical care: a qualitative study. BMC Psychiatry 13(34):1–12. https://doi.org/10.1186/1471-244X-13-34
Schlosser DA, Campellone TR, Truong B, Etter K, Vergani S, Komaiko K, Vinogradov S (2018) Efficacy of PRIME, a mobile app intervention designed to improve motivation in young people with schizophrenia. Schizophr Bull 44(5):1010–1020. https://doi.org/10.1093/schbul/sby078
Taylor KM, Bradley J, Cella M (2022) A novel smartphone-based intervention targeting sleep difficulties in individuals experiencing psychosis: a feasibility and acceptability evaluation. Psychol Psychother Theory Res Pract 95(3):717–737
Valentine L, McEnery C, O’Sullivan S, Gleeson J, Bendall S, Alvarez-Jimenez M (2020) Young people’s experience of a long-term social media-based intervention for first-episode psychosis: qualitative analysis. J Med Internet Res 22(6):e17570. https://doi.org/10.2196/17570
Williams A, Fossey E, Farhall J, Foley F, Thomas N (2018) Recovery after psychosis: qualitative study of service user experiences of lived experience videos on a recovery-oriented website. JMIR Ment Health 5(2):e37. https://doi.org/10.2196/mental.9934
Zarbo C, Agosta S, Casiraghi L, De Novellis A, Leuci E, Paulillo G, Rocchetti M, Starace F, Zamparini M, de Girolamo G (2022) Assessing adherence to and usability of experience sampling method (ESM) and actigraph in patients with schizophrenia spectrum disorder: a mixed-method study. Psychiatry Res 314:114675. https://doi.org/10.1016/j.psychres.2022.114675
Buck B, Nguyen J, Porter S, Ben-Zeev D, Reger GM (2022) FOCUS mHealth intervention for veterans with serious mental illness in an outpatient department of veterans affairs setting: feasibility, acceptability, and usability study. JMIR Ment Health 9(1):e26049. https://doi.org/10.2196/26049
Lal S, Gleeson JF, D’Alfonso S, Lee H, Etienne G, Joober R, Lepage M, Alvarez-Jimenez M (2023) Digital health innovation to prevent relapse and support recovery in young people with first-episode psychosis: a pilot study of Horyzons-Canada. Schizophrenia 9(1):21. https://doi.org/10.1038/s41537-023-00352-1
Lim MH, Gleeson JFM, Rodebaugh TL, Eres R, Long KM, Casey K, Abbott JM, Thomas N, Penn DL (2020) A pilot digital intervention targeting loneliness in young people with psychosis. Soc Psychiatry Psychiatr Epidemiol 55(7):877–889. https://doi.org/10.1007/s00127-019-01681-2
Lean M, Fornells-Ambrojo M, Milton A, Lloyd-Evans B, Harrison-Stewart B, Yesufu-Udechuku A, Kendall T, Johnson S (2019) Self-management interventions for people with severe mental illness: systematic review and meta-analysis. Br J Psychiatry J Ment Sci 214(5):260–268. https://doi.org/10.1192/bjp.2019.54
Leamy M, Bird V, Le Boutillier C, Williams J, Slade M (2011) Conceptual framework for personal recovery in mental health: systematic review and narrative synthesis. Br J Psychiatry J Ment Sci 199(6):445–452. https://doi.org/10.1192/bjp.bp.110.083733
Faith LA, Collins JO, Decker J, Grove A, Jarvis SP, Rempfer MV (2019) Experiences of empowerment in a community cognitive enhancement therapy program: an exploratory qualitative study. Psychosis 11(4):319–330. https://doi.org/10.1080/17522439.2019.1632920
Livet A, Navarri X, Potvin S, Conrod P (2020) Cognitive biases in individuals with psychotic-like experiences: a systematic review and a meta-analysis. Schizophr Res 222:10–22. https://doi.org/10.1016/j.schres.2020.06.016
Degnan A, Berry K, Humphrey C, Bucci S (2021) The relationship between stigma and subjective quality of life in psychosis: a systematic review and meta-analysis. Clin Psychol Rev 85:102003. https://doi.org/10.1016/j.cpr.2021.102003
Nguyen J, Goldsmith L, Rains LS, Gillard S (2022) Peer support in early intervention in psychosis: a qualitative research study. J Ment Health 31(2):196–202. https://doi.org/10.1080/09638237.2021.1922647
Burke E, Wood L, Zabel E, Clark A, Morrison AP (2016) Experiences of stigma in psychosis: a qualitative analysis of service users’ perspectives. Psychosis 8(2):130–142. https://doi.org/10.1080/17522439.2015.1115541
White S, Foster R, Marks J, Morshead R, Goldsmith L, Barlow S, Sin J, Gillard S (2020) The effectiveness of one-to-one peer support in mental health services: a systematic review and meta-analysis. BMC Psychiatr 20(1):1–20. https://doi.org/10.1186/s12888-020-02923-3
Fett AK, Viechtbauer W, Dominguez MD, Penn DL, van Os J, Krabbendam L (2011) The relationship between neurocognition and social cognition with functional outcomes in schizophrenia: a meta-analysis. Neurosci Biobehav Rev 35(3):573–588. https://doi.org/10.1016/j.neubiorev.2010.07.001
Fulford D, Schupbach E, Gard DE, Mueser KT, Mow J, Leung L (2022) Do cognitive impairments limit treatment gains in a standalone digital intervention for psychosis? a test of the digital divide. Schizophr Res Cogn 28:100244. https://doi.org/10.1016/j.scog.2022.100244
Lincoln AK, Adams W, Eyllon M, Garverich S, Prener CG, Griffith J, Paasche-Orlow MK, Hopper K (2017) The double stigma of limited literacy and mental health illness: examining barriers to recovery and participation among public mental health service users. Soc Ment Health 7(3):121–141. https://doi.org/10.1177/2156869317707001
Vanova M, Aldridge-Waddon L, Jennings B, Puzzo I, Kumari V (2020) Reading skills deficits in people with mental illness: a systematic review and meta-analysis. Eur Psychiatry J Assoc Eur Psychiatr 64(1):e19. https://doi.org/10.1192/j.eurpsy.2020.98
Garety P, Ward T, Emsley R, Greenwood K, Freeman D, Fowler D, Kuipers E, Bebbington P, Rus-Calafell M, McGourty A, Sacadura C, Collett N, James K, Hardy A (2021) Effects of SlowMo, a blended digital therapy targeting reasoning, on paranoia among people with psychosis: a randomized clinical trial. JAMA Psychiat 78(7):714–725. https://doi.org/10.1001/jamapsychiatry.2021.0326
Greer B, Robotham D, Simblett S, Curtis H, Griffiths H, Wykes T (2019) Digital exclusion among mental health service users: qualitative investigation. J Med Internet Res 21(1):e11696. https://doi.org/10.2196/11696
Spanakis P, Peckham E, Mathers A, Shiers D, Gilbody S (2021) The digital divide: amplifying health inequalities for people with severe mental illness in the time of COVID-19. Br J Psychiatry J Ment Sci 219(4):529–531. https://doi.org/10.1192/bjp.2021.56
Spanakis P, Wadman R, Walker L, Heron P, Mathers A, Baker J, Johnston G, Gilbody S, Peckham E (2022) Measuring the digital divide among people with severe mental ill health using the essential digital skills framework. Perspect Public Health. https://doi.org/10.1177/17579139221106399
Holmberg C, Gremyr A, Karlsson V, Asztély K (2022) Digitally excluded in a highly digitalized country: an investigation of Swedish outpatients with psychotic disorders and functional impairments. Eur J Psychiatry 36:217–221. https://doi.org/10.1016/j.ejpsy.2022.04.005#
Biagianti B, Hidalgo-Mazzei D, Meyer N (2017) Developing digital interventions for people living with serious mental illness: perspectives from three mHealth studies. Evid Based Ment Health 20(4):98–101. https://doi.org/10.1136/eb-2017-102765
Watson A, Mellotte H, Hardy A, Peters E, Keen N, Kane F (2022) The digital divide: factors impacting on uptake of remote therapy in a South London psychological therapy service for people with psychosis. J Ment Health 31(6):825–832. https://doi.org/10.1080/09638237.2021.1952955
Adjekum A, Blasimme A, Vayena E (2018) Elements of trust in digital health systems: scoping review. J Med Internet Res 20(12):e11254. https://doi.org/10.2196/11254
Barnett-Page E, Thomas J (2009) Methods for the synthesis of qualitative research: a critical review. BMC Med Res Methodol 9:59. https://doi.org/10.1186/1471-2288-9-59
Bodicoat DH, Routen AC, Willis A, Ekezie W, Gillies C, Lawson C, Yates T, Zaccardi F, Davies MJ, Khunti K (2021) Promoting inclusion in clinical trials-a rapid review of the literature and recommendations for action. Trials 22(1):880. https://doi.org/10.1186/s13063-021-05849-7
Farooqi A, Jutlla K, Raghavan R, Wilson A, Uddin MS, Akroyd C, Patel N, Campbell-Morris PP, Farooqi AT (2022) Developing a toolkit for increasing the participation of black, Asian and minority ethnic communities in health and social care research. BMC Med Res Methodol 22(1):17. https://doi.org/10.1186/s12874-021-01489-2
Lawrence V, McCombie C, Nikolakopoulos G, Morgan C (2021) Ethnicity and power in the mental health system: experiences of white British and black Caribbean people with psychosis. Epidemiol Psychiatr Sci 30:e12. https://doi.org/10.1017/S2045796020001043
Flemming K, Booth A, Hannes K, Cargo M, Noyes J (2018) Cochrane qualitative and Implementation methods group guidance series-paper 6: reporting guidelines for qualitative, implementation, and process evaluation evidence syntheses. J Clin Epidemiol 97:79–85. https://doi.org/10.1016/j.jclinepi.2017.10.022
Noyes J, Booth A, Cargo M, Flemming K, Harden A, Harris J, Garside R, Hannes K, Pantoja T, Thomas J (2023) Chapter 21: Qualitative evidence. In: Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (eds). Cochrane Handbook for Systematic Reviews of Interventions version 6.4 (updated August 2023). Available from www.training.cochrane.org/handbook.
Wainwright M, Zahroh RI, Booth TÖ, A, Bohren M. A, Noyes J, Cheng W, Munthe-Kaas H, & Lewin S. (2023) The use of GRADE-CERQual in qualitative evidence synthesis: an evaluation of fidelity and reporting. Health Res Policy Syst 21(1):77. https://doi.org/10.1186/s12961-023-00999-3
Borghouts J, Eikey E, Mark G, De Leon C, Schueller SM, Schneider M, Stadnick N, Zheng K, Mukamel D, Sorkin DH (2021) Barriers to and facilitators of user engagement with digital mental health interventions: systematic review. J Med Internet Res 23(3):e24387. https://doi.org/10.2196/24387
Peng R, Li X, Guo Y, Ning H, Huang J, Jiang D, Feng H, Liu Q (2024) Barriers and facilitators to acceptance and implementation of eMental-health intervention among older adults: a qualitative systematic review. Digital Health. https://doi.org/10.1177/20552076241234628
MacHale R, Ffrench C, McGuire B (2023) The experiences and views of adults with intellectual disabilities accessing digital mental health interventions: a qualitative systematic review and thematic synthesis. J Appl Res Intell Disabil JARID 36(3):448–457. https://doi.org/10.1111/jar.13082
Dhippayom T, Rattanachaisit N, Wateemongkollert A, Napim R, Chaiyakunapruk N (2023) Should CINAHL be used as one of the main databases for evidence synthesis of health services intervention? Cochrane Evid Synth Methods 1:e12019. https://doi.org/10.1002/cesm.12019
Wright K, Golder S, Lewis-Light K (2015) What value is the CINAHL database when searching for systematic reviews of qualitative studies? Syst Rev 4:104. https://doi.org/10.1186/s13643-015-0069-4
Eriksen MB, Frandsen TF (2018) The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Libr Assoc JMLA 106(4):420–431. https://doi.org/10.5195/jmla.2018.345
Booth A, Noyes J, Flemming K, Moore G, Tunçalp Ö, Shakibazadeh E (2019) Formulating questions to explore complex interventions within qualitative evidence synthesis. BMJ Glob Health 4(Suppl 1):e001107. https://doi.org/10.1136/bmjgh-2018-001107
Acknowledgements
C.E. acknowledges support from a Wellcome Early Career Award (227646/Z/23/Z). P.G. is part funded by the NIHR Maudsley Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, grant reference NIHR203318. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Funding
No financial funding was received for this review.
Author information
Authors and Affiliations
Contributions
All authors contributed to the review conception and design. Data collection and analysis were performed by S.D. and R.P. The first draft of the manuscript was written by S.D. all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors disclose that there are no potential conflicts of interest in this review.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dennard, S., Patel, R., Garety, P. et al. A systematic review of users experiences of using digital interventions within psychosis: a thematic synthesis of qualitative research. Soc Psychiatry Psychiatr Epidemiol (2024). https://doi.org/10.1007/s00127-024-02692-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00127-024-02692-4