
Abstract
Background
The application of the suprapatellar (SP) approach has challenged the traditional infrapatellar (IP) approach in the surgery treatment of tibial shaft fractures, yet the advantages and disadvantages still remain controversial. We included more high-quality studies for this meta-analysis and systematic review to evaluate the clinical outcomes and prognosis of both approaches and thus to provide new ideas for surgeons.
Method
We searched literatures from PubMed, Cochrane Library, Web of Science, and EMBASE databases from January 2000 to December 2022. We extracted general information including sample size, gender, proportion of open fracture, follow-up time, and outcome indicators including entrance accuracy, fluoroscopy time, operation time, intraoperative blood loss, Lysholm score, VAS pain score, range of motion (ROM) function score, reposition accuracy, and revision cases. Cochrane Collaboration's tool and the Newcastle–Ottawa Scale were used to evaluate literature qualities. Meta-analysis was performed using RevMan 5.4 software.
Results
A total of 23 studies were generated that qualified for inclusion, 17 of which were used for meta-analysis. This study found statistically significant differences in coronal plane entrance accuracy, fluoroscopy time, Lysholm score, and VAS pain score.
Conclusion
The results of our meta-analysis showed that the SP approach was significantly better than the IP approach in angle and distance entrance accuracy of coronal plane, angle entrance accuracy of sagittal plane, fluoroscopy time, Lysholm score, and VAS pain score. There were no significant differences in sagittal angle accuracy, operative time, intraoperative blood loss, and ROM score.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Among all long bone fractures, the tibial fracture is the most common and accounts for the largest proportion of adolescents, of which approximately 24% are open fractures, with the fracture form often presenting as transverse oblique and spiral fractures. Tibial shaft fractures account for approximately 1.9% of all fractures in the body, with an overall incidence of approximately 20/100,000/year [1, 2]. Due to the specificity of the site, non-surgical treatment often results in poor alignment, fracture displacement, prolonged immobilization, ankle stiffness, and lower limb function [41]. Currently, the main surgical treatment measures for tibial shaft fractures are intramedullary nailing (IMN) and open reduction internal fixation (ORIF) with locking plates. However, after ORIF, complications such as surgical site infection [45], effusion, and osteomyelitis often occur [3], with a consequent risk of readmission [28], while IMN is widely used because of convenient access, less trauma, less stripping of periosteal tissue, and easy recovery with half or even full weight bearing [3].
The traditional incision point for IMN was the IP approach, separating the patellar tendon and inserting IMN from the parapatellar position. Although the minimal incision facilitated postoperative recovery, it was still challenged by the high incidence of postoperative complications such as anterior knee pain [4].In 1996, P Tornetta 3rd was the first to report an alternative surgical approach [5], the SP approach, which has the advantage that the target leg is placed in a semi-extended position of the knee, eliminating quadriceps stretch forces on the proximal fragment and valgus deformity. Intraoperatively, the procedure was performed under the condition that the knee was flexed at approximately 20 degrees. A 3 cm long incision was made approximately 3–5 cm wide above the patella to longitudinally separate the quadriceps tendon, the patellofemoral joint was further bluntly dissected, and then a trocar system was inserted through the joint space to create a starting point at the junction of the proximal tibial anterior cortex and articular surface. Intraoperative fluoroscopy as well as fracture reposition was easier to obtain due to the specific flexion position, and another potential advantage may be improving in anterior knee pain, as the new approach was unlikely to stimulate the patellar tendon or injure intra-articular structures if surgeons performed properly [40, 44]. Studies [6,7,8] showed that the ideal inserting point of the safety zone was located at the anterior edge of the tibial plateau and medial to the lateral tibial spine. The aforementioned safety zone was small and the intra-articular structures of the knee may be damaged if the correct point of entrance was lost.
To further investigate whether there is a significant difference in the effect of the two approaches on the surgical procedure and postoperative recovery, we compiled more and newer literature, and then performed this meta-analysis to obtain the final results. We hypothesized that the SP approach would be superior to the IP approach in terms of entrance accuracy, fluoroscopy time, functional scores, and anterior knee pain.
Methods
Search method
This meta-analysis was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [16]. We searched the following databases: PubMed, EMBASE, Cocharen, and Web of Science, from January 2000 to December 2022. The following keywords were entered: “Suprapatellar and infrapatellar”, “intramedullary nail”, and “tibal” “fracture” in the process. The language was set as English, without geographical restrictions.
Criteria
Inclusion criteria: (1) adult patients with normal skeletal development and tibial intramedullary nailing for the first time; (2) RCTs or observational studies; (3) intervention controls: suprapatellar versus infrapatellar groups; (4) record of the results: entrance accuracy (include degree and distance), fluoroscopy time, operation time, intraoperative blood loss, Lysholm score (which was first published in 1982 in the form of a scale containing eight items on knee function and symptoms describing activities of daily living for patients, and is now widely used in all types of knee fractures, 6 months postoperatively), VAS pain score (6 months postoperative) and ROM scores (6 months postoperative). The exclusion criteria were as follows: biomechanical experiments, animal experiments, cadaveric studies, conference abstracts, case reports, review and meta-analyses or pathologic fractures.
Statistics
The extracted information included: (1) research background, first author, year of publication, country, study design, sample size, average sample age, gender, proportion of open fracture, and follow-up time; (2) study results, including entry point accuracy, fluoroscopy time, operation time, intraoperative blood loss, Lysholm score, VAS pain score, and ROM function score.
Research quality assessment
We assessed the risk of bias by using Revman for the included study type of RCT by Cochrane criteria, including: random sequence generation, allocation concealment, participant and personnel blinding, blind method of result assessment, incomplete outcome data, selective reporting, and other source bias, and evaluated them with low risk, high risk, or unclear risk. For observational studies, we used the Newcastle–Ottawa Scale for a systematic star rating, dividing the studies into a 0–9 level, with levels greater than 6 being considered as high-quality studies. Any of the above assessment differences were resolved by the co-authors through consultation.
Statistical analysis
For the included data, all were analyzed by the Revman 5.4 software. Mean difference and 95% confidence intervals were calculated. I2 was used for the heterogeneity testing. A random effect model was used regardless of I2. Sources of heterogeneity were explored by sensitivity analysis or subgroup analysis.
Results
Study search
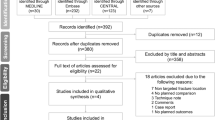
Following the search strategy described above, 525 studies were initially screened from the four databases, and 59 were retained after removing the duplicates. By reading the titles and abstracts, 20 studies were excluded for not meeting our requirements, leaving 39 articles for the full text reading. Finally, 23 articles were selected for the meta-analysis. The searching process is shown in Fig. 1. Demographic characteristics are summarized in Table 1.

Flow diagram of the article selection process
Data included
3 RCTs and 20 observational studies were included following the above search strategy, and all included studies were completed by December 2022. A total of 2140 patients with tibial fractures were considered, including 1008 SP intramedullary nailing and 1132 IP intramedullary nailing therapy. Follow-up time for each study varied from 6 to 63 months.
Risk bias and quality assessment
Two RCTs showed a higher risk of bias in participant blinding (Fig. 2). All observational studies had an NOS score of 7 or higher, indicating an acceptable methodological quality (Fig. 3).

Risk of bias assessment summary of three RCTs (Cochrane tool RoB 2). Green, low risk of bias; red, high risk of bias; yellow, moderate risk of bias

A funnel plot of Lysholm scores. An asymmetry was exhibited in the funnel plot, which reflected the publication bias

Forest plot for coronal and sagittal plane degrees alignment (°); SP suprapatellar; IP infrapatellar; MD mean difference; SD standard deviation; IV inverse variance analysis; CI confidence interval; SMD standard mean difference; CI confidence interval

Forest plot for coronal and sagittal plane distance alignment (mm); SP suprapatellar; IP infrapatellar; MD mean difference; SD standard deviation; IV inverse variance analysis; CI confidence interval; SMD standard mean difference

Forest plot for fluoroscopy time (s)、operative time (min) and intraoperative blood loss (ml); SP suprapatellar; IP infrapatellar; MD mean difference; SD standard deviation; IV inverse variance analysis; CI confidence interval; SMD standard mean difference

Forest plot for Lysholm knee score、VAS pain score and range of motion; SP suprapatellar; IP infrapatellar; MD mean difference; SD standard deviation; IV inverse variance analysis; CI confidence interval; SMD standard mean difference
Alignment
Five studies [20, 21, 41,42,43] reported the angular alignment and the difference of the angle was significant between the two groups in the coronal plane (SMD = – 1.74[ – 2.22, – 1.26]; p < 0.00001; I2 = 84%), while it was not significant in the sagittal plane (SMD = – 1.18[ – 2.59,0.24]; p < 0.10; I2 = 98%) (Fig. 4).
Five studies [23, 25, 29, 33, 43] reported the distance alignment, and one paper was excluded from this meta-analysis because it reported only the median of the quartile spacing, while Anderson et al.[23] found better distance alignment in the coronal plane in their study. Both the differences in the distance between the two groups in the coronal plane (SMD = – 1.47[ – 2.18, – 0.77]; p = 0.04; I2 = 65%) and sagittal plane (SMD = – 3.12[ – 5.54, – 0.69]; p < 0.01; I2 = 91%) were significant (Fig. 5) (Table 2).
Overall in terms of alignment, the superiority of the SP over the IP is reflected in the distance alignment in the coronal and sagittal planes, as well as the angular alignment in the coronal plane. It is noteworthy that the included sample almost had no proximal tibial fractures.
Fluoroscopy time (s)
Six studies [21, 26, 27, 34, 41, 43] reported fluoroscopy exposure during the procedure. Among them, Gao [41] only reported the fluoroscopy number and not time, and Llano [34] only reported the interquartile range of fluoroscopy time. Thus, their studies were excluded from this meta-analysis. Fluoroscopy was used for a significantly shorter amount of time in the SP group (SMD = – 39.23[ – 45.55, – 32.91]; p < 0.00001; I2 = 0%). Even so, in the two studies that were excluded, the number of fluoroscopies was significantly less in the SP (14.10 ± 2.51) than in the IP group (19.61 ± 3.12) with statistical difference (p < 0.001) [41]. The mean time of use of fluoroscopy was 94,5 s in the SP group compared with 204,5 s in the IP group. There was a significant difference (p < 0.001) [34] (Fig. 6).
Operation time (s)
Eight studies [21, 22, 26, 29, 32, 38, 40, 41] reported the operation time. A random-effects model was used. The difference between the two groups in terms of operation time was not significant (SMD = – 3.90[ – 10.23,2.42]; p = 0.23; I2 = 94%).
Intraoperative blood loss (mL)
Five studies [22, 26, 32, 40, 43] reported the intraoperative blood loss. A fixed-effects model was used. The difference between the two groups in terms of intraoperative blood loss was not significant (SMD = -0.12[-0.95,1.71]; p = 0.09; I2 = 0%).
Lysholm knee score
Eleven studies [22, 24, 26, 28, 29, 31, 33, 38, 40, 41, 43] reported the Lysholm knee score. A random-effects model was used. In the result of a 6-month follow-up including 851 patients (SP 423, IP 438), there was significant difference between the two groups in terms of Lysholm knee score (SMD = 5.88[3.39, 8.36]; p < 0.00001; I2 = 76%). In the subgroup analysis, the RCT studies showed that a higher Lysholm knee score in the IP group with homogeneity detected (SMD = 7.88[5.52, 10.24]; p < 0.00001; I2 = 0%) (Fig. 7).
VAS pain score
Six studies [26, 28, 31, 39, 41, 43] reported the anterior knee VAS pain score, and it was not connected with the site of the approach used. A random-effects model was used. There was significant difference between the two groups in terms of VAS pain score. (SMD = – 0.64[ – 1.10, – 0.17]; p = 0.007; I2 = 96%). We discovered that Gao et al.[41] had a significant impact on heterogeneity by analyzing six studies of sensitivity, After removing the study, the results showed low heterogeneity in the remaining five studies. After exclusion, there was still significant difference between the two groups in terms of VAS pain score. (SMD = – 0.84[ – 0.93, – 0.76]; p < 0.00001; I2 = 35%). After careful analysis of the literature and the selection criteria, we still did not find the exact source of heterogeneity and decided to keep it in this meta-analysis considering the relevant quality of the study.
Range of motion
Six studies [26, 31, 32, 38, 40, 43] reported the range of motion. A random-effects model was used. There was no significant difference between the two groups in terms of range of motion (SMD = 3.21[ – 1.37,7.78]; p = 0.17; I2 = 96%).
Discussion
We included more and newer studies [22, 29,30,31, 34, 40,41,42,43] for this meta-analysis and systematic review, 20 observational studies and 3 RCTs. According to our latest findings, the SP group performed better in entrance alignment and intraoperative fluoroscopy time, and had significantly superior Lymsholm scores and anterior knee VAS scores to the IP group, while we did not find similar results in terms of operative time and intraoperative blood loss.
The SP approach has attracted a lot of attention from scholars in the intraoperative and postoperative conditions. In two meta-analyses published in 2018, the results showed the superiority of the SP group over the IP group in terms of intraoperative blood loss, ROM, VAS, Lysholm, and fluoroscopy time. The authors acknowledged the need for more other high-quality RCTs to confirm these findings [9,10,11,12]. In 2021, Packer [13] found differences between the two approaches in Lysholm scores, fluoroscopy time, and entrance alignment in a meta-analysis including 12 studies, while the differences in complications and intraoperative blood loss were not significant. However, Ponugoti [14] found in his meta-analysis that the two approaches differed only in VAS and Lysholm, while there were no significant differences in operative time, fluoroscopy time, deep infection rate, bone nonunion, or secondary procedures. In addition to pain, Lysholm's ratings include instability, thigh muscle atrophy, swelling, and lameness. Despite the correlation between Lysholm and VAS, due to the higher level of heterogeneity resulting from variability in follow-up time, the author stated that their long-term results still need to be confirmed and evaluated in further studies. Sepehri [15] found in a recent meta-analysis that the SP group performed better in Lysholm and intraoperative fluoroscopy time, but showed no such differences in operative time.
The alignment of the entry point is a parameter that is often overlooked by researchers, yet it is equally influenced by the approach. First, mechanically, since the SP approach avoids patellar obstruction, the inserted guide pin easily finds a satisfactory angle while providing a narrow safe entry point for the intramedullary nail to ensure a satisfactory distance deviation [25]; in fluoroscopic slice position, the entry point of the sagittal plane can be clearly confirmed to be located at the junction between the anterior cortex and the articular surface in the tibial plane [43] and therefore did not show any correlation with the two entry points. This may explain the better performance of the entrance point in the coronal plane in terms of accuracy.
In addition, Anderson [23] found that in terms of distance, the accuracy of the entry point in the coronal plane was significantly better than in the sagittal plane, which was similar to our analysis. In cadaveric studies, Franke [17] found that when using the SP approach in the procedure, a more parallel insertion angle to the longitudinal axis was obtained. Thus, both the risk of iatrogenic fracture of the posterior cortex and implant protrusion can be reduced. Therefore, it is reasonable to believe that the suprapatellar approach can help the surgeon to obtain better accuracy in angles and distances in the coronal plane.
According to the accuracy of the achieved reposition, Avilucea [20] reported primary angular disorders in 35 (26.1%) patients in the SP group and 5(3.8%) patients in the SP group (p < 0.0001). For valgus and recurvatum, SP performed better than IP. Moreover, Matthew [42] reported that 11 (15%) patients in the SP group had alignment of > 5 degrees from ideal, compared to 17 (33%) patients in the IP group. Gao [41] reported that 3 (4.3%) patients in the SP group and 15 (23.8%) patients in the IP group had poor fracture reduction. Although this seems to indicate that SP has better reduction results, the data are almost exclusively from distal tibial fractures, and the difference between fracture reduction in the middle and proximal tibia remains to be studied more.
Both Chan [28] and Courtney [21] reported one case requiring return to the operating room for exchange intramedullary nailing due to nonunion in the SP group. MacDonald [24] reported 11 further procedure cases in the SP group, in which 6 involved removal of distal locking screws and 5 involved removal of proximal locking screws. These number are three and one in the IP group. Sun [26] reported seven cases of implant loosening, 4(4%) in the SP and three (5%) in IP; they all led to bone nonunion and IMN revision. However, there were no significant differences in the major complication rate that induced revision or implant removal between the two groups. None of our current study included skin incision infections and deep infections, as these are influenced by multiple factors. Also, open fractures were not included in our study because of the high incidence of sepsis [46]. Therefore, the available findings suggest that although the SP group outperformed the IP group in terms of reposition accuracy and remaining malposition, the superiority in the subsequent need for revision may be challenged.
In the analysis of the fluoroscopy time, the SP group took less time than the IP group and the statistical results were discrepant. In the infrapatellar approach, the knee is placed in a hyper-flexed position on the fluoroscopic triangle device, whereas in the suprapatellar approach the semi-extended position of the knee (15–20°) not only facilitates the repositioning, but also allows for a shorter and easier fluoroscopy condition [6]. Moreover, the fluoroscopy time required by itself is substantially reduced due to the easier positioning of the intramedullary nail entry point under the SP approach. Correspondingly, the reduction in fluoroscopy time also shortens the operative time. It was worth mentioning that Wilianmson [7] innovatively focused on the data of radiation exposure (cGY/cm2), which was significantly lower in the SP group than in the IP group. Azzawi [29] stated the same conclusion in his study. These suggest that the change in approach will benefit both the surgeons and the patients. In the study of Gao [41], the mean number of fluoroscopy procedures (n) in the SP group was 14.10, significantly lower than that of the IP group at 19.61. Almost all of the studies that included fluoroscopy condition favored the SP group. Therefore, we have reason to believe that fluoroscopy time(s), fluoroscopy number (n), and radiation exposure (cGY/cm2) were significantly lower in the SP group than in the IP group.
There are more clinical evaluations of knee function, and due to limitations in literature screening, we only included in our analysis the Lysholm score [8]. This meta-analysis showed that between the two groups, the SP group had a better Lysholm score. Because pain conditions were also included in the Lysholm score, it had some association with the VAS pain score. The outcome of both groups may depend on intraoperative damage to the patellofemoral joint, saphenous nerve, intramedullary nail protrusion, and local inflammation, although the specific device maximally protects the patellofemoral cartilage and talus [10]. Gelbke [9] showed that SP nail insertion contact pressure was high on the patellofemoral joint, but still lower than the threshold of chondrocyte damage. In addition, Leliveld [35] found that the infrapatellar approach may damage the infrapatellar nerve, thereby causing postoperative knee pain and numbness in patients. Katsoulis [4] reported a 47% rate of knee pain after intramedullary nail fixation; however, there is a lack of data to support whether the SP approach will reduce this.
Most of the Lysholm scores in this meta-analysis were from patients 6 months postoperatively. Meanwhile, at the 12-month follow-up, several studies [22, 28, 41] reported the total knee Lysholm scores were comparable between the two groups. Nevertheless, MacDonald [24] reported significant improvements in SP compared to IP at only 1 year. In addition, Sun [26] found tha Lysholm scores were higher in the SP group at both 6 and 24 months after surgery. At about 30 months of follow-up, Çiçekli [33] did not find a significant difference in Lysholm scores between the two groups. These may suggest that the two approaches are fraught with uncertainty in the long-term prognosis of Lysholm scores, even so, we are still confident in the results of this meta-analysis that they differed significantly at least within 6 months after surgery.
Postoperative anterior knee pain was always unavoidable [18], and the sources of pain include implant protrusion, changed biomechanics. and the injury of intra-articular structures, patellar tendon, fat pad, and infrapatellar branch of the saphenous nerve [19]. Theoretically, the change in approach could effectively circumvent some of these factors. For example, in the suprapatellar approach, precise insertion points can avoid damage to the knee structure. A more parallel insertion angle to the longitudinal axis can avoid implant protrusion and infrapatellar nerve injury. These may explain the association between higher insertion point accuracy and lower VAS scores.
Likewise, most of the VAS scores in this meta-analysis were also from patients 6 months postoperatively. In the long-term prognosis, Sun [26] showed significant difference between the two groups at 12 and 24 months postoperatively; he also reported the conditions at 1and 3 months, but the outcomes were not significant. Lu [43] reported better performance in the SP group at 12 months, though it contradicted the findings of some studies [28, 30, 41].
Although some former studies [25, 28, 36, 37] did not find any difference in VAS scores between SP and IP, more data from the combined meta-analysis still gives us confidence in the results. Considering the high heterogeneity for some results of this meta-analysis, it should be treated with caution, which also means that we need more high-quality studies.
Although our meta-analysis incorporated more recent studies, explored most of the relevant questions, and reached the latest conclusions in the two groups, several potential limitations should be noted: (1) we were unable to include more RCTs in the literature due to the specificity of the study; (2) in the face of high heterogeneity, we were not able to explore their sources; (3) the prognosis of short-term follow-up within 6 months as well as infection, deformity,and bone nonunion was not comprehensive due to literature limitations.
Conclusion
The results of our meta-analysis showed that the SP approach was significantly better than the IP approach in angle and distance entrance accuracy of coronal plane, angle entrance accuracy of sthe agittal plane, fluoroscopy time, Lysholm score, and VAS pain score. There were no significant differences in the sagittal angle accuracy, operative time, intraoperative blood loss, and ROM score. Moreover, the specificity of the SP approach may be more suitable for young surgeons to learn, and in terms of safety, no significant patellar injury was observed in patients undergoing the SP approach.
Availability of data and materials
The authors declare that all the data supporting the findings of this study are available within the article and its supplementary information files.
References
Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37(8):691–7.
Mundi R, Chaudhry H, Niroopan G, et al. Open tibial fractures:updated guidelines for management. JBJS Rev. 2015. https://doi.org/10.2106/JBJS.RVW.N.00051.
Costa ML, Achten J, Griffin J, Petrou S, Pallister I, Lamb SE, Parsons NR, FixDT Trial Investigators. Effect of locking plate fixation vs intramedullary nail fixation on 6-month disability among adults with displaced fracture of the distal tibia: the UK FixDT randomized clinical trial. JAMA. 2017;318(18):1767–76.
Katsoulis E, Court-Brown C, Giannoudis PV. Incidence and aetiology of anterior knee pain after intramedullary nailing of the femur and tibia. J Bone Joint Surg Br. 2006;88(5):576–80. https://doi.org/10.1302/0301-620X.88B5.16875.
Tornetta P 3rd, Collins E. Semiextended position of intramedullary nailing of the proximal tibia. Clin Orthop Relat Res. 1996;328:185–9.
Franke J, Hohendorff B, Alt V, et al. Suprapatellar nailing of tibial fractures: indications and technique. Injury. 2016;47(2):495–501.
Eastman J, Tseng S, Lo E, et al. Retropatellar technique for intramedullary nailing of proximal tibia fractures: a cadaveric assessment. J Orthop Trauma. 2010;24(11):672–6.
Kubiak EN, Widmer BJ, Horwitz DS. Extra-articular technique for semiextended tibial nailing. J Orthop Trauma. 2010;24(11):704–8.
Wang C, Chen E, Ye C, Pan Z. Suprapatellar versus infrapatellar approach for tibia intramedullary nailing: a meta-analysis. Int J Surg. 2018;51:133–9. https://doi.org/10.1016/j.ijsu.2018.01.026. (Epub 2018 Jan 31).
Chen X, Xu HT, Zhang HJ, Chen J. Suprapatellar versus infrapatellar intramedullary nailing for treatment of tibial shaft fractures in adults. Medicine (Baltimore). 2018;97(32): e11799. https://doi.org/10.1097/MD.0000000000011799.
Gao Z, Han W, Jia H. Suprapatellar versus infrapatellar intramedullary nailing for tibal shaft fractures: a meta-analysis of randomized controlled trials. Medicine (Baltimore). 2018;97(24): e10917. https://doi.org/10.1097/MD.0000000000010917.
Yang L, Sun Y, Li G. Comparison of suprapatellar and infrapatellar intramedullary nailing for tibial shaft fractures: a systematic review and meta-analysis. J Orthop Surg Res. 2018;13(1):146. https://doi.org/10.1186/s13018-018-0846-6.
Packer TW, Naqvi AZ, Edwards TC. Intramedullary tibial nailing using infrapatellar and suprapatellar approaches: a systematic review and meta-analysis. Injury. 2021;52(3):307–15. https://doi.org/10.1016/j.injury.2020.09.047. (Epub 2020 Sep 23).
Ponugoti N, Rudran B, Selim A, Nahas S, Magill H. Infrapatellar versus suprapatellar approach for intramedullary nailing of the tibia: a systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):94. https://doi.org/10.1186/s13018-021-02249-0.
Sepehri A, You D, Lobo AA, Schneider P, Lefaivre KA, Guy P. Comparison of patient-reported outcomes after suprapatellar versus infrapatellar nailing techniques for tibial shaft fractures: a systematic review and meta-analysis. J Orthop Trauma. 2022;36(6):e208–14. https://doi.org/10.1097/BOT.0000000000002303.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372: n71.
Franke J, Homeier A, Metz L, Wedel T, Alt V, Spät S, Hohendorff B, Schnettler R. Infrapatellar vs. suprapatellar approach to obtain an optimal insertion angle for intramedullary nailing of tibial fractures. Eur J Trauma Emerg Surg. 2018;44(6):927–38. https://doi.org/10.1007/s00068-017-0881-8. (Epub 2017 Nov 20).
Ringenberg JD, Tobey JL, Horinek JL, Teague DC. Suprapatellar versus infrapatellar approach for intramedullary nail fixation of tibial shaft fractures: a review of the literature. OTA Int. 2022;5(1): e196. https://doi.org/10.1097/OI9.0000000000000196.
Bishop JA, Campbell ST, Eno JT, et al. Knee pain after intramedullary nailing of tibia fractures: prevalence, etiology, and treatment. J Am Acad Orthop Surg. 2018;26:e381–7.
Avilucea FR, Triantafillou K, Whiting PS, Perez EA, Mir HR. Suprapatellar intramedullary nail technique lowers rate of malalignment of distal tibia fractures. J Orthop Trauma. 2016;30(10):557–60.
Courtney PM, Boniello A, Donegan D, Ahn J, Mehta S. Functional knee outcomes in infrapatellar and suprapatellar tibial nailing: does approach matter? Am J Orthop (Belle Mead NJ). 2015;44(12):E513–6 (PMID: 26665254).
Lu Y, Wang G, Hu B, Ren C, Sun L, Wang Z, He C, Xue H, Li Z, Zhang K, Ma T, Wang Q. Comparison of suprapatellar versus infrapatellar approaches of intramedullary nailing for distal tibia fractures. J Orthop Surg Res. 2020;15(1):422.
Anderson TRE, Beak PA, Trompeter AJ. Intra-medullary nail insertion accuracy: a comparison of the infra-patellar and supra-patellar approach. Injury. 2019;50(2):484–8.
MacDonald DRW, Caba-Doussoux P, Carnegie CA, Escriba I, Forward DP, Graf M, Johnstone AJ. Tibial nailing using a suprapatellar rather than an infrapatellar approach significantly reduces anterior knee pain postoperatively: a multicentre clinical trial. Bone Joint J. 2019;101-B(9):1138–43.
Jones M, Parry M, Whitehouse M, Mitchell S. Radiologic outcome and patient-reported function after intramedullary nailing: a comparison of the retropatellar and infrapatellar approach. J Orthop Trauma. 2014;28(5):256–62.
Sun Q, Nie X, Gong J, Wu J, Li R, Ge W, Cai M. The outcome comparison of the suprapatellar approach and infrapatellar approach for tibia intramedullary nailing. Int Orthop. 2016;40(12):2611–7.
Williamson M, Iliopoulos E, Williams R, Trompeter A. Intra-operative fluoroscopy time and radiation dose during suprapatellar tibial nailing versus infrapatellar tibial nailing. Injury. 2018;49(10):1891–4.
Chan DS, Serrano-Riera R, Griffing R, Steverson B, Infante A, Watson D, Sagi HC, Sanders RW. Suprapatellar versus infrapatellar tibial nail insertion: a prospective randomized control pilot study. J Orthop Trauma. 2016;30(3):130–4.
Al-Azzawi M, Davenport D, Shah Z, Khakha R, Afsharpad A. Suprapatellar versus infrapatellar nailing for tibial shaft fractures: a comparison of surgical and clinical outcomes between two approaches. J Clin Orthop Trauma. 2021;29(17):1–4.
Rodríguez-Zamorano P, García-Coiradas J, Galán-Olleros M, Marcelo Aznar H, Alcobia-Díaz B, Llanos S, Valle-Cruz JA, Marco F. Suprapatellar tibial nailing, why have we changed? Rev Esp Cir Ortop Traumatol. 2022;66(3):159–69.
Zhu Z, Wang Z, Zhou P, Wang X, Guan J. Comparison of clinical efficacy of suprapatellar and infrapatellar intramedullary nailing in treating tibial shaft fractures. Pak J Med Sci. 2021;37(7):1753–7.
Cui Y, Hua X, Schmidutz F, Zhou J, Yin Z, Yan SG. Suprapatellar versus infrapatellar approaches in the treatment of tibia intramedullary nailing: a retrospective cohort study. BMC Musculoskelet Disord. 2019;20(1):573.
Cicekli O, Topcu HN, Kochai A, Sukur E, Turker M. Comparison of suprapatellar and infrapatellar tibial nailing: moreanatomic entry point and fracture reduction via the suprapatellarapproach. Int J Clin Exp Med. 2019;12(1):804–11.
Llano L, Soruco ML, Taype Zamboni D, Sancineto C, Barla J, Carabelli G. Comparison between functionality and quality of reduction between suprapatellar vs infrapatellar approaches in the treatment of diaphyseal and distal tibial fractures. Eur J Orthop Surg Traumatol. 2022;33:889–92.
Leliveld MS, Verhofstad MH. Injury to the infrapatellar branch of the saphenous nerve, a possible cause for anterior knee pain after tibial nailing? Injury. 2012;43(6):779–83.
Bakhsh WR, Cherney SM, McAndrew CM, Ricci WM, Gardner MJ. Surgical approaches to intramedullary nailing of the tibia: comparative analysis of knee pain and functional outcomes. Injury. 2016;47(4):958–61. https://doi.org/10.1016/j.injury.2015.12.025. (Epub 2016 Jan 18).
Ryan SP, Steen B, Tornetta P 3rd. Semi-extended nailing of metaphyseal tibia fractures: alignment and incidence of postoperative knee pain. J Orthop Trauma. 2014;28(5):263–9. https://doi.org/10.1097/BOT.0000000000000083.
Ozcan C, Turkmen I, Sokucu S. Comparison of three different approaches for anterior knee pain after tibia intramedullary nailing. Eur J Trauma Emerg Surg. 2020;46(1):99–105.
Isaac M, O’Toole RV, Udogwu U, Connelly D, Baker M, Lebrun CT, Manson TT, Zomar M, O’Hara NN, Slobogean GP. Incidence of knee pain beyond 1 year suprapatellar versus infrapatellar approach for intramedullary nailing of the tibia. J Orthop Trauma. 2019;33(9):438–42.
Lu K, Gao YJ, Wang HZ, Li C, Qian RX, Dong QR. Comparison between infrapatellar and suprapatellar approaches for intramedullary nailing for the fractures of the tibial shaft. Eur J Trauma Emerg Surg. 2020;48:3651–7.
Gao F, Wang XH, Xia SL, Zhou XX, Wang MH, Fu BG, Yi CG, Guo SY. Intramedullary nail fixation by suprapatellar and infrapatellar approaches for treatment of distal tibial fractures. Orthop Surg. 2022;14(9):2350–60.
Hague M, Texeira D, Anderson T, Williamson M, Trompeter A. Nailing distal tibial fractures: does entry technique affect distal alignment? Eur J Orthop Surg Traumatol. 2021;33(61):66.
Lu K, Wang HZ, Qian RX, Wu ZQ, Li C, Gao YJ. Removing a suprapatellar intramedullary nail via a suprapatellar approach: a retrospective cohort study. Int Orthop. 2022;46(5):1145–54.
Gaines RJ, Rockwood J, Garland J, Ellingson C, Demaio M. Comparison of insertional trauma between suprapatellar and infrapatellar portals for tibial nailing. Orthopaedics. 2012;39:1155–8.
Stephens KR, Shahab F, Galat D, Anderson D, Shahabuddin S, Whiting PS, et al. Management of distal tibial metaphyseal fractures with the SIGN intramedullary nail in 3 developing countries. J Orthop Trauma. 2015;29:469–75.
Marecek GS, Nicholson LT, Broghammer FH, Talerico M, Tougas C, Donegan DJ, Scolaro JA. Risk of knee sepsis after treatment of open tibia fractures: a multicenter comparison of suprapatellar and infrapatellar approaches. J Orthop Trauma. 2018;32(2):88–92. https://doi.org/10.1097/BOT.0000000000001024.
Funding
This study was supported by the Natural Science Foundation of Guangdong Province (2018A030313369), 2022 Huang Feng National Famous Traditional Chinese Medicine Expert Inheritance Studio, Special Funds for the Discipline Reserve Talent Cultivation Project of Guangzhou University of Chinese Medicine “Double First-Class”, and High-level University Construction, National Natural Science Foundation of China (81974575).
Author information
Authors and Affiliations
Contributions
ZW: writing—original draft, writing—review and editing. XX: literature search, visualization, validation. ZL: literature search. YG: supervision, project administration, funding acquisition.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wang, Z., Xiong, X., Lu, Z. et al. A systematic review and meta-analysis comparing suprapatellar versus infrapatellar approach intramedullary nailing for tibal shaft fractures. Eur J Trauma Emerg Surg 50, 383–394 (2024). https://doi.org/10.1007/s00068-023-02384-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00068-023-02384-9