
Abstract
Background
The correlation between cardiovascular risk scoring systems and the severity of coronary artery diseases (CAD) is not clear. The present research aimed to evaluate the Multi-Ethnic Study of Atherosclerosis (MESA) risk score and Framingham risk score (FRS), using the Gensini score (GS) system as reference, so as to determine which model is better for the prediction of CAD severity.
Methods
This research was a single-center and cross-sectional observational study. In total, 1423 patients were included in our study. Three different groups were formed according to GS: 0 < GS ≤ 22 (low GS group, n = 484); 22 < GS ≤ 42 (intermediate GS group, n = 468); GS > 42 (high GS group, n = 471). Logistic and linear regression analyses were carried out to explore the relationship between the risk score models and the GS. The performance of the risk models was determined by receiver operating characteristic curve (ROC) analysis.
Results
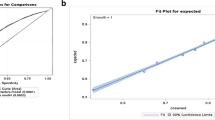
The MESA risk score and the FRS both had a statistically significant power for the prediction of CAD severity (MESA area under curve: 0.630; FRS area under curve: 0.613). Furthermore, the MESA had a better performance in predicting the severity (p < 0.05) of CAD compared with the FRS. In the subgroup analysis, the MESA showed a better performance in the male (p < 0.05), diabetes mellitus (p < 0.05), and smoking subgroups (p < 0.05) compared with the FRS.
Conclusion
The MESA and FRS predicted the severity of CAD in the Chinese population of this study. Moreover, the MESA had a better performance than the FRS model in predicting the severity of CAD in the overall population as well as in the male, smoking, diabetes, and non-diabetes subgroups.
Zusammenfassung
Hintergrund
Die Korrelation zwischen kardiovaskulären Risikobewertungssystemen und dem Schweregrad einer koronaren Herzkrankheit (KHK) ist unklar. Ziel dieser Studie war es, den Risikoscore der Multi-Ethnic Study of Atherosclerosis (MESA) und den Framingham-Risikoscore (FRS) unter Einsatz des Gensini-Scores (GS) als Referenz zu untersuchen, um zu ermitteln, welches Modell sich besser zur Prädiktion des KHK-Schweregrads eignet.
Methoden
Es handelte sich um eine Einzelzentrum-Beobachtungsstudie im Querschnittdesign. In die Studie wurden 1423 Patienten einbezogen. Gemäß GS wurden 3 verschiedene Gruppen gebildet: 0 < GS ≤ 22 (Gruppe mit niedrigem GS, n = 484); 22 < GS ≤ 42 (Gruppe mit mittlerem GS, n = 468); GS > 42 (Gruppe mit hohem GS, n = 471). Logistische und lineare Regressionsanalysen erfolgten, um den Zusammenhang zwischen den Risikoscore-Modellen und dem GS zu untersuchen. Die Leistungsstärke der Risikomodelle wurde anhand der Receiver-Operating-Characteristic-Curve(ROC)-Analyse beurteilt.
Ergebnisse
Der MESA-Risikoscore und der FRS wiesen beide eine statistisch signifikante Power für die Prädiktion des KHK-Schweregrads auf (Fläche unter der Kurve, AUC, für MESA: 0,630; AUC für FRS: 0,613). Außerdem zeigte sich beim MESA eine bessere Leistungsstärke zur Vorhersage des Schweregrads einer KHK (p < 0,05) als bei dem FRS. In der Subgruppenanalyse war die Leistungsstärke des MESA in Bezug auf die Subgruppen Männer (p < 0,05), Diabetes-mellitus-Patienten (p < 0,05) und Raucher (p < 0,05) besser als der FRS.
Schlussfolgerung
Sowohl mit dem MESA als auch mit dem FRS ließ sich der Schweregrad einer KHK in der chinesischen Population dieser Studie vorhersagen. Darüber hinaus ergab sich für den MESA eine bessere Leistungsstärke als für das FRS-Modell hinsichtlich der Vorhersage des Schweregrads einer KHK in der Gesamtpopulation sowie bei den Subgruppen Männer, Raucher, Diabetespatienten und Personen ohne Diabetes.


Similar content being viewed by others

References
GBD 2013 Mortality and Causes of Death Collaborators (2015) Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 385(9963):117–171. https://doi.org/10.1016/S0140-6736(14)61682-2
Patel V, Chatterji S, Chisholm D, Ebrahim S, Gopalakrishna G, Mathers C, Mohan V, Prabhakaran D, Ravindran RD, Reddy KS (2011) Chronic diseases and injuries in India. Lancet 377(9763):413–428. https://doi.org/10.1016/s0140-6736(10)61188-9
D’Agostino RB Sr, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, Kannel WB (2008) General cardiovascular risk profile for use in primary care. Circulation 117(6):743–753. https://doi.org/10.1161/circulationaha.107.699579
McClelland RL, Jorgensen NW, Budoff M et al (2015) 10-year coronary heart disease risk prediction using coronary artery calcium and traditional risk factors. J Am Coll Cardiol 66(15):1643–1653. https://doi.org/10.1016/j.jacc.2015.08.035
Sayin MR, Cetiner MA, Karabag T, Akpinar I, Sayin E, Kurcer MA, Dogan SM, Aydin M (2014) Framingham risk score and severity of coronary artery disease. Herz 39(5):638–643. https://doi.org/10.1007/s00059-013-3881-4
Versteylen MO, Joosen IA, Shaw LJ, Narula J, Hofstra L (2011) Comparison of Framingham, PROCAM, SCORE, and Diamond Forrester to predict coronary atherosclerosis and cardiovascular events. J Nucl Cardiol 18(5):904–911. https://doi.org/10.1007/s12350-011-9425-5
Chen S, Liu Y, Islam SMS, Yao H, Zhou Y, Chen J‑Y, Li Q (2018) A simple prediction model to estimate obstructive coronary artery disease. BMC Cardiovasc Disord 18(1):1–9. https://doi.org/10.1186/s12872-018-0745-0
Günaydın ZY, Karagöz A, Bektaş O, Kaya A, Kırış T, Erdoğan G, Işık T, Ayhan E (2016) Comparison of the Framingham risk and SCORE models in predicting the presence and severity of coronary artery disease considering SYNTAX score. Anatol J Cardiol 16(6):412–418. https://doi.org/10.5152/AnatolJCardiol.2015.6317
Gensini GG (1983) A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol 51(3):606
Xu RX, Li S, Li XL, Zhang Y, Guo YL, Zhu CG, Wu NQ, Qing P, Sun J, Dong Q, Li JJ (2015) High-density lipoprotein subfractions in relation with the severity of coronary artery disease: A Gensini score assessment. J Clin Lipidol 9(1):26–34. https://doi.org/10.1016/j.jacl.2014.11.003
Ipek E (2017) The relationship of micronucleus frequency and nuclear division index with coronary artery disease SYNTAX and Gensini scores. Anatol J Cardiol. https://doi.org/10.14744/anatoljcardiol.2017.7582
Gong P, Luo SH, Li XL, Guo YL, Zhu CG, Xu RX, Li S, Dong Q, Liu G, Chen J, Zeng RX, Li JJ (2014) Relation of ABO blood groups to the severity of coronary atherosclerosis: An Gensini score assessment. Atherosclerosis 237(2):748–753. https://doi.org/10.1016/j.atherosclerosis.2014.10.107
Rashiti P, Behluli I, Bytyqi AR (2017) Assessment of the correlation between severity of coronary artery disease and waist–hip ratio. Open Access Maced J Med Sci 5(7):929–933. https://doi.org/10.3889/oamjms.2017.211
Wilson PWF, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB (1998) Prediction of coronary heart disease using risk factor categories. Circulation 97(18):1837–1847. https://doi.org/10.1161/01.CIR.97.18.1837
Acet H, Ertaş F, Bilik MZ, Aydın M, Yüksel M, Polat N, Yıldız A, Özyurtlu F, Akıl MA, Çiftçi L, Özbek M, Alan S, Toprak N (2015) The relationship of TIMI risk index with SYNTAX and Gensini risk scores in predicting the extent and severity of coronary artery disease in patients with STEMI undergoing primary percutaneous coronary intervention. Ther Adv Cardiovasc Dis 9(5):257–266. https://doi.org/10.1177/1753944715574814
Avci A, Fidan S, Tabakçı MM, Toprak C, Alizade E, Acar E, Bayam E, Tellice M, Naser A, Kargın R (2016) Association between the Gensini score and carotid artery stenosis. Korean Circ J 46(5):639–645. https://doi.org/10.4070/kcj.2016.46.5.639
Bekler A, Barutçu A, Tenekecioglu E, Altun B, Gazi E, Temiz A, Kırılmaz B, Ozkan MT, Yener AU (2015) The relationship between fragmented QRS complexes and SYNTAX and Gensini scores in patients with acute coronary syndrome. Kardiol Pol 73(4):246–254. https://doi.org/10.5603/KP.a2014.0208
Kalkan K, Hamur H, Yildirim E, Ipek E, Ermis E, Ozturk M, Karal H, Korkmaz AF, Bayantemur M, Demirelli S (2018) The comparison of angiographic scoring systems with the predictors of atherosclerosis. Angiology 69(2):158–163. https://doi.org/10.1177/0003319717712118
Acknowledgements
First and foremost, I would like to show my deepest gratitude to my supervisors, Dr. Fu and Dr. Zhang, respectable, responsible, and resourceful scholars, who have provided me with valuable guidance in every stage of writing this article. My sincere appreciation also goes to my colleagues, Heng Wu MD, Xulin Hong MD, Chunxia Gu MD, and Qingbo Lv MD; without their help and encouragement, this article would not be completed. Finally, thanks to those l love and those who love me.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
Y. Wang, Q. Lv, H. Wu, K. Chen, X. Hong, C. Gu, G. Fu, and W. Zhang declare that they have no competing interests.
All studies performed were in accordance with the ethical standards indicated in each case. All the study protocols were in accordance with the Declaration of Helsinki. All patients provided written informed consent.
Additional information
Y. Wang and Q. Lv contributed equally to this article.
Rights and permissions
About this article

Cite this article
Wang, Y., Lv, Q., Wu, H. et al. Comparison of MESA of and Framingham risk scores in the prediction of coronary artery disease severity. Herz 45 (Suppl 1), 139–144 (2020). https://doi.org/10.1007/s00059-019-4838-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00059-019-4838-z