
Abstract
Background
To evaluate the role of craniofacial shape in malocclusion by application of geometric morphometrics to a set of two-dimensional landmarks and semilandmarks obtained from lateral skull radiographs.
Methods
Cephalometric radiograph tracings of 88 untreated Caucasians (age range 7–39 years) were assigned to four groups according to their occlusion: neutrocclusion, distocclusion, mesiocclusion, and anterior open bite. The geometric morphometric shape analysis incorporated 66 landmarks and semilandmarks, which underwent generalized Procrustes analysis, between-groups principal component analysis, thin-plate spline deformation grid visualization, permutation tests, and receiver operating characteristic curves.
Results
The position and shape of the mandible contributed to differences between the distocclusion and mesiocclusion groups, whereas the maxillary shape showed less variation. The growth-related shape alteration during adolescence was most pronounced in the mesiocclusion group and least pronounced in the neutrocclusion group. The open bite group was associated with an altered orientation of the mandibular body and the maxilla, showed the most hyperdivergent maxillomandibular pattern but was not an own skeletal entity. Despite clear differences in mean shape across the four groups, the individual distribution of craniofacial shape overlapped between the groups without discrete clusters.
Conclusions
Craniofacial shape was clearly associated with dental malocclusion and showed considerable variation. Geometric morphometrics was a powerful research tool but for diagnosing individual malocclusion standard cephalometric measurements including overjet and overbite were equally or more efficient than geometric morphometric descriptors.
Zusammenfassung
Hintergrund
Untersuchung der kraniofazialen Formvariation und ihrer Assoziation mit 4 Okklusionstypen mittels geometrisch-morphometrischer Analysen zweidimensionaler Messpunkte auf seitlichen Schädelröntgenbildern.
Methodik
Untersucht wurden Durchzeichnungen der Fernröntgenseitenbilder von 88 unbehandelten Europäern im Alter zwischen 7 und 39 Jahren, die anhand ihrer Verzahnung 4 Gruppen zugeteilt worden waren: Neutralokklusion, Distalokklusion, Mesialokklusion und anterior offener Biss. Die geometrische Morphometrie bezog 66 (Semi-)Landmarken ein, diese wurden einer Prokrustesanalyse und einer “between-groups principal component analysis” unterzogen, in einem Thin-Plate-Spline-Deformationsgitter visualisiert und mit Permutationstests und ROC (“receiver operating characteristic”)-Kurven evaluiert.
Ergebnisse
Position und Gestalt des Unterkiefers trugen zu den primären Unterschieden zwischen der Distal- und Mesialokklusionsgruppe bei. Die Form der Maxilla dagegen zeigte deutlich weniger Variation. Wachstumsbedingte Formveränderungen während der Adoleszenz waren in der Mesialokklusionsgruppe am stärksten, in der Neutralokklusionsgruppe am wenigsten ausgeprägt. In der Gruppe mit anterior offenem Biss fiel eine Umorientierung des Corpus mandibulae und der Maxilla bei maximal hyperdivergentem Muster auf, doch stellte diese Gruppe keine eigene skelettale Entität dar. Trotz klarer Unterschiede zwischen den morphometrischen Durchschnittsformen der 4 Okklusionsgruppen überlappten die individuellen Formkonfigurationen zwischen den Gruppen, ohne dass Cluster beobachtet wurden.
Schlussfolgerung
In der vorliegenden Studie bestanden eindeutige Verknüpfungen zwischen kraniofazialer Form und Okklusionstyp, sie unterlagen aber erheblicher Variation. Die geometrische Morphometrie hat sich als effektive Forschungsmethode bewährt. Für die individuelle Diagnose einer Malokklusion waren jedoch kephalometrische Standardmessungen einschließlich Overjet und Overbite gleich effizient oder sogar effizienter als geometrisch-morphometrische Deskriptoren.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Thorough diagnosis and treatment planning of malocclusions require a distinct understanding of both dentoalveolar and skeletal components in anterior–posterior and vertical directions [17, 33, 34]. While Angle’s classification is based on dental criteria, lateral cephalometric headfilms display the skeletal framework in association with the dentition [30, 36].
Conventional radiograph cephalometry combines linear and angular measurements or indices derived from these measurements [18, 35]. For research, however, cephalometric measurements may not suffice a detailed description of the craniofacial morphology [5, 13, 15, 25, 29]. These shortcomings can be overcome by geometric morphometrics (GM), a method based upon the Cartesian coordinates of landmarks. After standardizing landmark configurations for overall position, scale, and orientation, the resulting shape coordinates represent the shape of the configurations only, whereas the overall size of the configurations is explicitly represented by a single variable: centroid size, a standard measure of the overall size of a landmark configuration. Centroid size equals the square root of the summed squared distances of the landmarks from their centroid (average landmark position).
Because of the powerful visualization techniques and the typically large number of variables, GM allows for effective exploratory studies and statistical tests [5, 25]. GM has been applied in orthodontic research to study growth, treatment effects, and shape variation [6–8, 12, 15, 16, 20, 21].
In the present study we applied GM including between-groups principal component analysis (bgPCA) in order to (1) compare craniofacial shape across the Angle classes and open bite malocclusion in a sample of juvenile and adult untreated patients. (2) We investigated if different types of occlusion were associated with a particular skeletal pattern. (3) We assessed individual variation within the malocclusion groups and quantified (4) to which degree the diagnosis of malocclusion can be inferred from skeletal morphology itself. For this purpose we contrasted the performance of GM descriptors with classic measurements.
Materials and methods
The sample comprised 88 Caucasians aged from 7 to 39 years (median 12 years; details shown in Table 1). In all, 28 males and 60 females were pooled together for all analyses. Inclusion criteria embraced complete mixed and permanent dentitions without consideration of third molars. Exclusion criteria were dental agenesis except third molars, cleft palate, craniofacial syndrome, former orthodontic treatment, and prosthetic therapy. Following the assignment protocol of Ellis and McNamara [9] and Singh et al. [35], pretreatment study casts of the patients were used to diagnose either an Angle class I (neutrocclusion), class II (distocclusion), class III (mesiocclusion), or open bite malocclusion (zero or negative overbite). The institutional ethics committee approved this investigation (no. 1033/2012).
The lateral cephalometric radiographs originated from two private practices, a public health care institution, and the dental university, all situated in Vienna, Austria. The radiographs had been taken for orthodontic treatment planning. Two authors traced the X-rays on matte acetate sheets. Intra- and interoperator reliabilities of the tracings were tested with Dahlberg’s equation yielding errors ranging from 0.3 to 1.3 mm (mean 0.7 mm) and 0.5°–1.8° (mean 1°). A third investigator, who was blind to the diagnosis, made scans of the manual tracings and digitized the following 16 anatomical landmarks using the TPSdig 2.0 software (James Rohlf, State University of New York, Stony Brook, NY, USA): nasion, orbitale, sella, the most superior point on the clivus, basion, the highest point on the coronoid process, condylion, anterior nasal spine, posterior nasal spine, supradentale, infradentale, the intercuspal indentions of the averaged maxillary and mandibular first molars, superior incision, inferior incision, and the apices of the maxillary and mandibular incisors.
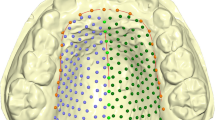
In addition, the outlines of the mandible, the clivus, and the maxilla between posterior nasal spine and prosthion were measured by a total of 50 semilandmarks, i.e., points on smooth curves, for which the exact location on the curve cannot be identified and hence is statistically estimated. We used the sliding landmark algorithm for this purpose, which minimized the bending energy, a measure of local shape difference, between each individual and the sample average [5, 23]. This approach allowed for the joint analysis of homologous points (anatomical landmarks) and curves represented by semilandmarks (Fig. 1; Table 2).

a Scatterplot of the superimposed landmark configurations (Procrustes shape coordinates). b Visualization of the sample mean shape
Abb. 1 a Scatter-Plot der überlagerten Landmarken-Konfigurationen (Prokrustes-Koordinaten). b Visualierung der Durchschnittsform in der Patientengruppe
After sliding the semilandmarks, all 88 landmark configurations were superimposed by Generalized Procrustes Analysis, a least-squares oriented registration technique, standardizing position, scale, and orientation of all configurations [31]. Procrustes registration does not require specification of a reference plane because it is based on all landmarks and semilandmarks [15]. The resulting Procrustes shape coordinates contain only information on the shape of the landmark configurations and are the basis for further statistical analysis.
We computed and visualized the average shape of all four diagnostic groups, regardless of the age. In addition, we linearly regressed the shape coordinates on age to model age-dependent shape variation within each of the four groups. Gender was used as a covariate in these regressions to account for the heterogeneity of the age distribution between the sexes. The multivariate pattern of individual and group mean differences was assessed by bgPCA [24], an ordination technique in-between the more familiar approaches of principal component analysis and discriminant function analysis. It leads to a low-dimensional representation of the high-dimensional shape space that maximizes the variation between the group means. Thin-plate spline deformation grids were used to visualize average shape differences between diagnostic groups and age effects.
The statistical significance of group mean differences was assessed by permutation tests, using 5000 random permutations and the Procrustes distance between the group mean shapes as the test statistic. Permutation tests do not require normally distributed variables and can be applied to multivariate datasets that are not of full rank, such as Procrustes shape coordinates.
To investigate whether the patients can be successfully classified to their diagnostic groups when using only bony structures, without reference to the teeth, we computed leave-one-out classifications based on multiple-group linear discriminant functions for two different datasets, one containing only skeletal landmarks and another one containing only dental landmarks (molars and incisors). We used the first five ordinary principal components (PCs) of each dataset for the classification. A higher number of PCs did not increase classification success. In addition, we computed receiver operating characteristic (ROC) curves [39] based on the bgPCs for (1) the full dataset, (2) the skeletal landmarks, and (3) the linear measurements overjet and overbite. The ROC curve plots the true positive rate (sensitivity) against the false-positive rate (1—specificity).
Results
The four mean craniofacial shapes of the malocclusion groups differed mainly in mandibular shape and size (relative to other facial structures) as well as in the orientation and position of the teeth (Figs. 2, 3; Table 2). The average mandible was more prognathic in the class III group and retrognathic in the class II group. Compared to class III individuals, the class II group had a more flexed gonial angle and a shorter chin. In the anterior open bite group the mandible was short, the gonial angle obtuse, and the maxilla and mandible showed the greatest divergence.

Mean shapes of the four diagnostic groups
Abb. 2 Durchschnittsformen der 4 diagnostischen Gruppen

Deformation grids illustrating the mean shape differences between Angle Class I group and the three types of malocclusion. Shape differences are linearly extrapolated by factor 2
Abb. 3 Deformationsgitter zur Darstellung der Formunterschiede zwischen der Klasse-I-Gruppe und den 3 Arten der Malokklusion. Formunterschiede sind linear mit dem Faktor 2 extrapoliert
The first two between-groups PCs in Fig. 4 accounted for 42% of total shape variation between the patients and for 97% of shape variation between the four group means. The shape differences among the three Angle classes were closely aligned with bgPC 1 (anterior–posterior direction), where the class I group was between class II and class III individuals. The class II and open bite groups were considerably more variable along bgPC 2 (vertical direction) than the other groups (Fig. 4).

Scatter plot of the first two between-group principal components (bgPCs) of shape. Class I patients are shown by black filled circles, class II patients by red squares, class III patients by green triangles, and open bite patients by blue open circles. Large black circles represent group averages. Black arrows depict linear estimates of average growth in the four groups (linear regressions of shape on age). Arrows are scaled to correspond to the average shape change from 8- to 20-year-old individuals in each group; the length of the arrow is an estimate of the magnitude of overall shape change in this age period, whereas differences in direction indicate differences in the pattern of shape change. Shape differences associated with PC axes are visualized by shapes corresponding to scores of −0.8 and 0.8 for PC1 (anteroposterior direction) and −0.6 and 0.6 for PC2 (vertical direction). (Units in Procrustes distance)
Abb. 4 Scatter-Plot der ersten 2 “between-group principal components” (bgPCs) der Form. Schwarze geschlossene Kreise Klasse-I-Patienten, rote Vierecke Klasse-II-Patienten, grüne Dreiecke Klasse-III-Patienten, blaue offene Kreise Patienten mit offenem Biss. Große schwarze Kreise stehen für Durchschnittswerte in den Gruppen, schwarze Pfeile für lineare Schätzungen des durchschnittlichen Wachstums in den 4 Gruppen (lineare Regressionen: Form—Alter). Skalierungen auf den Pfeilen entsprechen den durchschnittlichen Formveränderungen zwischen 8 und 20 Lebensjahren in jeder Gruppe, die Länge des Pfeils ist eine Abschätzung der Formveränderungen insgesamt in diesem Altersintervall, unterschiedliche Richtungen dagegen zeigen Unterschiede im Muster der Formveränderung an. Mit den PC-Achsen assoziierte Formunterschiede sind visualisiert durch Formen entsprechend Scores von −0,8 und 0,8 für PC1 (anteroposteriore Richtung) sowie −0.6 und 0,6 für PC2 (vertikale Richtung). (Einheiten in Prokrustes-Distanzen)
In Fig. 4, the bgPCA shows substantial individual overlap between the groups. Despite this overlap, the groups without open bite differed significantly in mean shape (p < 0.001 for all pairwise tests after Bonferroni correction). Individuals with open bite differed significantly from the class II group only (p < 0.001 after Bonferroni correction).
The black arrows in the bgPCA plot (Fig. 4) represent the average shape difference between 8-year-old patients and 20-year-old patients, derived from the linear regressions of shape on age. The arrows head in similar directions, indicating that growth patterns were similar across all four groups and that the shape differences between the four groups were already present in childhood. Hence, the variation of age within each group did not obscure the presented group mean differences.
In Fig. 5, the average shape change within the observed growth period, pooled over all diagnostic groups and genders, is shown. With increasing age, the mandibular ramus increased in height and the gonial angle flexed, the chin projected forward, and the lower incisors were displaced anteriorly relative to the upper incisors.

Visualization of the average age-related shape changes, pooled over all four groups. The first three illustrations show the average shapes of 7-, 18-, and 40-year-old patients, estimated from a linear regression of shape on age. The 40-year shape is an extrapolation of the actual growth pattern. The deformation grid illustrates shape differences between the 7- and 40-year shapes by threefold extrapolation of the actually observed growth
Abb. 5 Visualisierung der durchschnittlichen altersbezogenen Formveränderungen, gepoolt für alle 4 Gruppen. Die ersten 3 Bilder zeigen die durchschnittlichen Formen bei 7, 18 und 40 Jahre alten Patienten, geschätzt entsprechend einer linearen Form-Alter-Regression. Die Form bei 40 Jahren ist eine Extrapolation des tatsächlichen Wachstumsmusters. Das Deformationsgitter stellt die Unterschiede zwischen den 7- und 40-Jahre-Formen durch dreifache Extrapolation des beobachteten Wachstums dar
In Figs. 2, 3 and 4, it can be seen that bony structures differed across the groups even though the diagnostic criteria referred to the first molar interdigitation exclusively. When using landmarks located only on bony structures, 64.5% of the patients were classified correctly with regard to their occlusion in the discriminant function analysis. Using molar and incisor landmarks, 80.3% of the patients were classified in agreement with the original assignment of occlusion.
Figure 6 shows the ROC curves computed separately for three different datasets: a dataset including all landmarks, another containing skeletal landmarks only, and a third one for standard linear measurements of incisor overjet and overbite. The ROC curves for Angle class I versus class II groups (Fig. 6a) and group I versus group III (Fig. 6b) yielded three similar curves, indicating that the three datasets have a similar power to discriminate between the malocclusion groups. Table 3 lists the values for the areas under the ROC curves, which ranged from 0.74 to 0.98.

Receiver operating characteristic (ROC) curves for a Angle class I versus Angle class II, b Angle class I versus Angle class III, and c Angle class I versus open bite. Classifications in a and b are based on bgPC 1 using all landmarks (solid blue lines) and skeletal landmarks only (dashed red lines). Dotted green lines denote classifications based on overjet. In c, blue and red lines are computed from bgPC 2 using all landmarks and skeletal landmarks, respectively (green line refers to overbite)
Abb. 6 ROC (“receiver operating characteristic”)-Kurven für a Angle-Klasse I vs. Klasse II, b Angle-Klasse I vs. Klasse III und c Angle-Klasse I vs. offener Biss. Die Klassifikationen zu a und b basieren auf bgPC 1 unter Verwendung aller Landmarken (durchgezogene blaue Linie) bzw. der skelettalen Landmarken (gestrichelte rote Linie). Gepunktete grüne Linien zeigen auf dem Overjet basierende Klassifikationen. c Blaue und rote Linien wurden auf der Basis von bgPC 2 unter Verwendung aller bzw. nur der skelettalen Landmarken berechnet (die grüne Linie basiert auf dem Overbite)
The Angle class III group was generally more distinguishable from the class I group than the class II sample from the class I sample. In Fig. 4, the larger overlap between groups I and II than between groups I and III corroborates this statement. The comparisons between the class I and open bite group is illustrated in Fig. 6c. Here the incisor overbite discriminated the groups to a higher degree than other landmark datasets.
Discussion
Deviant size, shape, and inclination of the maxillae contribute to craniofacial phenotype variation and malocclusion [11, 30]. Using GM and bgPCAs, we found a significant association between craniofacial shape and malocclusion. The average shape of the mandible differed across the four groups and presented a more acute gonial angle as well as a sagittally and vertically shorter lower face in the distocclusion group, while the mesiocclusion group showed the opposite pattern.
In the open bite group, both the maxilla and the mandibular body differed in their average inclination from the neutrocclusion group. The maxilla was inclined upward and the mandible downward. The downward rotation of the mandibular body was not primarily located at the gonion but along the entire posterior half of the mandibular corpus. This finding displays a similarity with Björk’s mandibular backward rotation around the last occluding molars in growing individuals [4].
In contrast to maxillary and mandibular shapes, the cranial base and upper face were similar across the groups as illustrated by Figs. 2 and 3. These structures suggested less association with malocclusion. The class I and class II groups showed almost identical dimensions for the average distance between sella and nasion while the mesiocclusion and open bite groups were also alike in their average sella-nasion measurements, but shorter (Table 2). This resemblance of the mesiocclusion and open bite groups is in agreement with Ellis and McNamara [9], who reported similar cranial base morphology for class III individuals with and without open bite.
Angulation and size of the cranial base have been considered causative factors in developing class II or class III relationships [10, 14, 22]. In our study the mesiocclusion group showed, on average, the greatest cranial base angle (nasion-sella-basion), the neutrocclusion group the smallest angle, and the means of the class II and open bite groups were between these. However, in accordance with recent investigations [2, 32], the differences in cranial base angle were small (ranging from 128.5° to 132.3°; Table 2) and they were not statistically significant, questioning the relevance of cranial base flexion for malocclusion.
In addition to skeletal differences, the malocclusion groups differed in incisor position. Proclined maxillary incisors and retroclined mandibular incisors in the class III group as well as protruded mandibular incisors in the class II group indicate dentoalveolar compensation for functional interarch relations under varying jaw relationships [26, 37, 38].
Because our sample was of mixed age, we observed growth effects on craniofacial shape from age 8 years onward. At this age the median cranial base, the presphenoid, and the cribriform plate as well as the cranial base angle are stable [1, 3, 22]. In the observed growth period, the mandibular ramus increased in height while the gonial angle decreased and the chin projected forward (Fig. 5). In the bgPCA plot in Fig. 4, the growth effects are represented as arrows from the average 8-year-old shape to the average 20-year-old shape within each group. The Angle class I group had the shortest arrow, i.e., the least alteration in shape between 8 and 20 years, while the other three groups showed more growth changes. The class III patients experienced the greatest extent of shape change. This unique divergence from the growth of the class I group may represent unbalanced growth rates or remodelling of craniofacial structures in class III individuals. The similarities of class I and class II craniofacial growth patterns, leading to a flattening of the face, agree with Yoon and Chung [40].
Despite the clear differences in average shape across the four groups, the individual distribution of craniofacial shape overlapped between these groups (Fig. 4). The deformation grids of Fig. 3 explicitly visualise the sites, where between-group differences of the phenotypes exist. Thus, craniofacial shape is not the sole cause of malocclusion but it clearly contributes to dental misalignment. The mesiocclusion group overlapped least with the neutrocclusion group, as compared to class II and open bite individuals. Craniofacial morphology seems to play a more important role for class III malocclusion than for other malocclusions.
The mesiocclusion group was also less variable along the vertical dimension (bgPC 2) than the other groups. Unique proportions and minimum skeletal variability explain this characteristic of the mesiocclusion group. The predominantly hyperdivergent but horizontally short maxilla of the class III group showed increased maxillary and mandibular molar dentoalveolar heights (Fig. 3) and yielded high mean values but small standard deviations for the angles SN–PP and PP–MP (Table 2).
The overlap of craniofacial shape among different types of occlusion is also reflected by the imperfect classification of patients based on the skeletal measurement points (Fig. 6; Table 3). The discriminant function analysis is powerful in determining whether a set of landmarks is effective in predicting inclusion to a category. Using skeletal landmarks and semilandmarks exclusively, classification was most successful for the class III group, again indicating its distinct craniofacial shape. However, malocclusion could also not be predicted perfectly when using molar and incisor landmarks only, presumably because of averaging bilateral structures on the tracing. About 20% of patients were classified incorrectly (Table 3).
Two-dimensional cephalograms apparently do not allow for a correct diagnosis in every instance. The actual occlusion was diagnosed according to the molar relationship on plaster casts. If diagnosis of malocclusion has to be made on the basis of cephalograms alone, the ROC statistics show that the geometric morphometric quantification of craniofacial shape does not outperform simple linear measurements of horizontal or vertical projections of the distance between the incisal edges (overbite, overjet). For the diagnosis of open bite, a measure of overbite is diagnostically even more effective than the multivariate approach.
As mentioned above, the malocclusion groups overlapped in shape space. Moreover there were no discrete clusters within the malocclusion groups. Moreno Uribe et al. [27, 28] studied craniofacial variation in distocclusion and mesiocclusion patients using numerous conventional cephalometric measurements, which were ranked by PCA, and reported the presence of multiple clusters of patients with respect to their craniofacial phenotypes. However, these “clusters” strongly overlapped even in a canonical variate analysis and, hence, are not clusters in the sense of separated groups of individuals. Neither their results nor our data support a distinctive and unique typology of craniofacial shape and occlusal pattern. Corroborating our findings, a morphometric study of adult skeletal open bite [19] also reported substantial variation in sagittal and vertical directions.
Limitations of our study include sample size, distribution of gender within groups, restriction to 2D data, and a cross-sectional retrospective study type. Within these limitations, the geometric morphometric analysis allowed for novel insights into craniofacial shape variation within and between the neutrocclusion and malocclusion groups.
Conclusions
Shape and relative position of the mandible contributed to malocclusion but varied considerably within the malocclusion groups. The maxillary shape and the cranial base showed less variation.
Skeletal morphology plays a larger role in individuals with class III malocclusion than in other malocclusions. Class III patients were considerably less variable in vertical direction than the other groups. The Angle class I group showed the least alteration in shape between 8 and 20 years.
The anterior open bite group had the most hyperdivergent skeletal pattern but was highly variable. The open bite group overlapped in its distribution with all three other groups and did not represent its own entity.
Geometric morphometrics proved to be a powerful research tool. Nonetheless, for the pure purpose of diagnosing malocclusion in an individual, standard cephalometric measurements as well as overjet and overbite appear to be equally or more efficient than geometric morphometric descriptors of dentofacial shape.
References
Afrand M, Ling CP, Khosrotehrani S, Flores-Mir C, Lagravère-Vich MO (2014) Anterior cranial-base time-related changes: a systematic review. Am J Orthod Dentofac Orthop 146(21–32):e6
Agarwal A, Pandey H, Bajaj K, Pandey L (2013) Changes in cranial base morphology in Class I and Class II Division 1 malocclusions. J Int Oral Health 5:39–42
Bastir M, Rosas A, O’Higgins P (2006) Craniofacial levels and the morphological maturation of the human skull. J Anat 209:637–654
Björk A (1969) Prediction of mandibular growth rotation. Am J Orthod 55:585–599
Bookstein FL (1997) Landmark methods for forms without landmarks: morphometrics of group differences in outline shape. Med Image Anal 1:225–243
Čelar AG, Onodera K, Bertl MH, Astl E, Bantleon H-P, Sato S, Mitteroecker P (2014) Geometric morphometric evaluations of a randomized prospective split-mouth study on modes of ligation and reverse-curve mechanics. Orthod Craniofac Res 17:158–169
Cevidanes LH, Franco AA, Gerig G, Proffit WR, Slice DE, Enlow DH, Yamashita HK, Kim YJ, Scanavini MA, Vigorito JW (2005) Assessment of mandibular growth and response to orthopedic treatment with 3-dimensional magnetic resonance images. Am J Orthod Dentofac Orthop 128:16–26
Cleall JF, BeGole EA, Chebib FS (1979) Craniofacial morphology: A principal component analysis. Am J Orthod 75:650–666
Ellis E, McNamara JA Jr (1984) Components of adult class III open-bite malocclusion. Am J Orthod 86:277–290
Enlow DH, Hans MG (1996) Essentials of facial growth. Saunders, Philadelphia, p 180
Enlow DH, Kuroda T, Lewis AB (1971) The morphological and morphogenetic basis for craniofacial form and pattern. Am J Orthod 41:161–188
Gkantidis N, Halazonetis DJ (2011) Morphological integration between the cranial base and the face in children and adults. J Anat 218:426–448
Grayson BH, Weintraub N, Bookstein FL, McCarthy JG (1985) A comparative cephalometric study of the cranial base and craniofacial anomalies: part I: tensor analysis. Cleft Pal J 22:75–87
Guyer EC, Ellis EE, McNamara JA Jr, Behrents RG (1986) Components of class III malocclusion in juveniles and adolescents. Angle Orthod 56:7–30
Halazonetis DJ (2004) Morphometrics for cephalometric diagnosis. Am J Orthod Dentofac Orthop 125:571–581
Hayashi K, Saitoh S, Mizoguchi I (2012) Morphological analysis of the skeletal remains of Japanese females from the Ikenohata-Shichikencho site. Eur J Orthod 34:575–581
Isaacson JR, Isaacson JI, Speidel TM, Worms FW (1971) Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod 41:219–229
KimYH Vietas JJ (1978) Anteroposterior dysplasia indicator: an adjunct to cephalometric differential diagnosis. Am J Orthod 73:619–633
Krey KF, Dannhauer KH, Hierl T (2015) Morphology of open bite. J Orofac Orthop 76:213–224
Krey KF, Dannhauer KH (2008) Morphometric analysis of facial profile in adults. J Orofac Orthop 68:424–436
McIntyre GT, Mossey PA (2003) Size and shape measurement in contemporary cephalometrics. Eur J Orthod 25:231–242
Melsen B (1974) The cranial base. The postnatal development of the cranial base studied histologically on human autopsy material. Acta Odontol Scand 32(Suppl):1–126
Mitteroecker P, Gunz P, Neubauer S, Müller GB (2012) How to explore morphological integration in human evolution and development. Evol Biol 39:536–553
Mitteroecker PM, Bookstein FL (2011) Linear discrimination, ordination, and the visualization of selection gradients in modern morphometrics. Evol Biol 38:100–114
Mitteroecker PM, Gunz P (2009) Advances in geometric morphometrics. Evol Biol 36:235–247
Molina-Berlanga N, Llopis-Perez J, Flores-Mir C, Puigdollers A (2013) Lower incisor dentoalveolar compensation and symphysis dimensions among class I and III malocclusion patients with different skeletal patterns. Angle Orthod 83:948–955
Moreno Uribe LM, Howe SC, Kummet C, Vela KC, Dawson DV, Southard TE (2014) Phenotypic diversity in white adults with moderate to severe class II malocclusion. Am J Orthod Dentofac Orthop 145:305–316
Moreno Uribe LM, Vela KC, Kummet C, Dawson DV, Southard TE (2013) Phenotypic diversity in white adults with moderate to severe class III malocclusion. Am J Orthod Dentofac Orthop 144:32–42
Moyers RE, Bookstein FL (1979) The inappropriateness of conventional cephalometrics. Am J Orthod 75:599–617
Proffit WR, Fields HW (1999) Contemporary Orthodontics, 3rd edn. Mosby, St. Louis, pp 146–196
Rohlf FJ, Slice DE (1990) Extensions of the Procrustes method for the optimal superimposition of landmarks. Syst Zool 39:40–59
Sanggarnjanavanich S, Sekiya T, Nomura Y, Nakayama T, Hanada M, Nakamura Y (2014) Cranial-base morphology in adults with skeletal Class III malocclusion. Am J Orthod Dentofac Orthop 146:82–91
Sassouni V, Nanda S (1964) Analysis of dentofacial vertical proportions. Am J Orthod 50:801–823
Schudy FF (1968) The control of vertical overbite in clinical orthodontics. Angle Orthod 38:19–39
Singh GD, McNamara JA Jr, Lozanoff S (1998) Procrustes, Euclidean and cephalometric analyses of the morphology of the mandible in human class III malocclusions. Arch Oral Biol 43:535–543
Singh P, Davies TI (2011) A comparison of cephalometric measurements: a picture archiving and communication versus the hand-tracing method—a preliminary study. Eur J Orthod 33:350–353
Solow B (1980) The dentoalveolar compensatory mechanism: background and clinical implications. Brit J Orthod 7:145–161
Sung-Jin K, Kyung-Ho K, Hyung-Seog Y, Hyoung-Seon B (2014) Dentoalveolar compensation according to skeletal discrepancy and overjet in skeletal Class III patients. Am J Orthod Dentofac Orthop 145:317–324
Wardlaw DW, Smith RJ, Hertweck DW, Hildebolt CF (1992) Cephalometrics of anterior open bite: a receiver operating characteristic (ROC) analysis. Am J Orthod Dentofac Orthop 101:234–243
Yoon SS, Chung CH (2015) Comparison of craniofacial growth of untreated Class I and Class II girls from ages 9 to 18 years: a longitudinal study. Am J Orthod Dentofac Orthop 147:190–196
Acknowledgement
Open access funding provided by [Medical University of Vienna].
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. Freudenthaler, A. Čelar, C. Ritt, and P. Mitteröcker declare that they have no competing interests.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Additional information
Professor Dr. Aleš Čelar.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Freudenthaler, J., Čelar, A., Ritt, C. et al. Geometric morphometrics of different malocclusions in lateral skull radiographs. J Orofac Orthop 78, 11–20 (2017). https://doi.org/10.1007/s00056-016-0057-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-016-0057-x