
Background
Inflammation in the lung is the body’s natural response to injury. It acts to remove harmful stimuli such as pathogens, irritants, and damaged cells and initiate the healing process. Acute and chronic pulmonary inflammation are seen in different respiratory diseases such as; acute respiratory distress syndrome, chronic obstructive pulmonary disease (COPD), asthma, and cystic fibrosis (CF).
Findings
In this review, we found that inflammatory response in COPD is determined by the activation of epithelial cells and macrophages in the respiratory tract. Epithelial cells and macrophages discharge transforming growth factor-β (TGF-β), which trigger fibroblast proliferation and tissue remodeling. Asthma leads to airway hyper-responsiveness, obstruction, mucus hyper-production, and airway-wall remodeling. Cytokines, allergens, chemokines, and infectious agents are the main stimuli that activate signaling pathways in epithelial cells in asthma. Mutation of the CF transmembrane conductance regulator (CFTR) gene results in CF. Mutations in CFTR influence the lung epithelial innate immune function that leads to exaggerated and ineffective airway inflammation that fails to abolish pulmonary pathogens. We present mechanistic computational models (based on ordinary differential equations, partial differential equations and agent-based models) that have been applied in studying the complex physiological and pathological mechanisms of chronic inflammation in different airway diseases.
Conclusion
The scope of the present review is to explore the inflammatory mechanism in airway diseases and highlight the influence of aging on airways’ inflammation mechanism. The main goal of this review is to encourage research collaborations between experimentalist and modelers to promote our understanding of the physiological and pathological mechanisms that control inflammation in different airway diseases.
Similar content being viewed by others

Introduction
Inflammation is the body’s natural defense mechanism to remove harmful stimuli such as pathogens, irritants and damaged cells and initiate the healing process. In general, inflammation is classified as acute or chronic inflammation [1]. Acute inflammation is a beneficial process that helps to immobilize the injured region and lets the rest of the immune system mobilize to heal injuries [2]. Chronic inflammation, on the other hand, turns into a problem rather than a solution to the injuries. Chronically inflamed tissues typically proceed to evoke immune cells from the bloodstream to amplify the inflammatory response. They can destroy healthy tissues in a misdirected attempt at initiating the healing process [3]. In general, inflammatory mechanisms employ a group of pattern recognition receptors (PRRs) to recognize molecular patterns expressed by the invading pathogens. These receptors may either be on the membrane surface e.g., Toll-Like receptors (TLRs) and C-type Lectin Receptors (CLRs) or inside the cytoplasm, e.g., Nod-Like Receptors (NLRs) and RIG-I-Like Receptors (RLRs) [4]. Next, the resolution process, which involves apoptosis and subsequent clearance of activated inflammatory cells, will initiate [5, 6]. Then, the process of tissue repair starts to retrieve damaged tissue [7].
Airway inflammation is usually caused by pathogens or by exposure to toxins, pollutants, irritants, and allergens [8]. TLRs recognize molecular patterns shared by pathogens and activate inflammatory cells like nuclear factor kappa-light-chain-enhancer of activated B-cells (NF-κB) and produce growth factors, chemokines, pro-inflammatory cytokines interleukin 8 (IL-8) and tumor necrosis factor alpha (TNF-α) to start resolution process [9]. IL-8 evokes neutrophils and TNF-α rises expression of endothelial cell adhesion molecules from lung capillaries [10]. Moreover, many of the known inflammatory target proteins, such as matrix metalloproteinase-9 (MMP-9), intercellular adhesion molecule-1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1), cyclooxygenase-2 (COX-2), and cytosolic phospholipase A2 (cPLA2), are specifically associated with airways inflammation in response to various stimuli [11]. Figure 1 presents an overview of general inflammatory signaling pathways and highlight the contribution of inflammatory mediators in airways diseases. The lung is a vital organ for providing mandatory oxygen for all organs in the body, and excessive inflammation can be life threatening. A delicate balance between inflammation and anti-inflammation is essential for lung homeostasis. Therefore, a comprehensive understanding of the inflammatory mechanisms is crucial in the treatment of patients with lung inflammation [12].

General inflammatory response in airways disease: Pathogens, toxins, pollutants, irritants and allergens activate airways epithelial cells as inflammatory stimuli. TLRs recognize patters shared by pathogens (Pattern recognition) and activate inflammatory cells like NF-κB, growth factors, chemokines, IL-8 and TNF-α. Activated cells phagocytose pathogens in the injured region (Resolution) and start wound healing to repair damaged epithelial cells (Tissue remodeling). TLRs: Toll-like-receptors, NF-κB: nuclear factor kappa-light-chain-enhancer of activated B-cells, IL-8: proinflammatory cytokines interleukin 8, TNF-α: tumor necrosis factor alpha
Different factors have been identified that affect the inflammatory response including tissue microenvironment, disease, energy, stress, neighborhood, and seasonal changes [13, 14]. In general, an interaction between neutrophils and epithelial cells provides the possibility for communication during inflammatory responses where the tissue microenvironment has explicit influence on signaling pathways and triggers immune cells to rush to the injured tissue [15]. Different inflammatory responses have been observed for various diseases [16,17,18,19] and the upregulation of the inflammatory response that occurs with advancing age is recognized as a major factor that leads to inflammaging [20]. Despite several studies being conducted on inflammation mechanisms, the influence of the discussed parameters on the inflammation mechanism remains unclear. Since inflammation is a complex and beneficial process in the human body, a better understanding of this process would help to develop novel strategies to diagnose disease susceptibility, target and control therapies, and conclusively develop new approaches to prevent and treat chronic diseases associated with aging [21].
Mathematical modeling is the art of representing a system with mathematical formulations whose analysis give useful information about the real system. Computational modeling is the application of mathematics to develop computer models for simulating the behavior of complex systems. Mathematical models of biological systems are usually complex and are often difficult to solve analytically and require the application of computational models to obtain numerical approximation of the model solution. Mathematical and computational models are useful in testing hypotheses, interpreting experiments, identifying chains of causation, performing sensitivity analyses and guiding new experiments [22]. Mathematical and computational models of biological systems may be categorized roughly into statistical or mechanistic models. Statistical model are data-driven models that utilize correlative methods to gain an understanding of a system and often lack mechanistic insights [23]. Example of statistics-based models are regression techniques, hierarchical clustering and principal component analysis. Mechanistic models are based on causative interactions of the components of a system and can unravel system dynamics that cannot be understood by investigating the dynamics of individual components of the system [23]. This review focuses on mechanistic models.
Mathematical and computational models are excellent tools that have been utilized successfully in studying the mechanisms that control the development and functioning of biological tissues including epithelial morphogenesis [24, 25] and lung morphogenesis [26,27,28,29,30].
Mathematical and computational models have been developed to study inflammation and these models have contributed to our understanding of the inflammatory process [23, 46,47,48,49,50,51,52,53,54]. Models have been developed to study lung respiration including gas exchange [55,56,57], ventilation [58,59,60,61,62,63,64], perfusion [65, 66] and tissue mechanics [67,68,69,70,70,71]. Most of these models have investigated the physiological functioning of normal healthy lungs and relatively few have focused on obstructive lung diseases [69]. Few models of obstructive lung diseases incorporate the effect of inflammation [73,74,75].
Reynolds et al. [76] developed a cellular automata model to simulate acute lung inflammation. Their model described the interaction of pulmonary epithelial cells and immune cells during an inflammatory response resulting from pathogen exposure. Their model results predicted three possible outcomes of an inflammatory response: a return to homeostasis, persistent infection with damaged tissue and resolved infection but with continued inflammation and damaged tissue, similar to clinical situations. Ibrahim et al. [77] simulated inflammation in an alveolus. They investigated the effects of low, medium, and high stretch/strain on inflammation dynamics. Their model incorporated the interactions of pro- and anti-inflammatory cytokines, immune cells, and epithelial cells occurring during a stretch-induced inflammation. Their results showed that the threshold of innate healing of a tissue might depend on the strain experienced by the tissue. When strain is under the threshold, the tissue is still capable of adapting its structure to heal the damaged part. However, there exists a strain threshold where healing capability breaks down. An et al. [78] implemented an agent-based model of acute pulmonary inflammation and simulated pulmonary contusion, pneumonia, and acute lung injury/acute respiratory distress syndrome. Simulation results of the model were qualitatively similar to clinical and radiographic observations [78]. Their results demonstrated the progression of alveolar edema resulting from a localized injury corresponding to blunt pulmonary trauma, the progression of pneumonia resulting from a localized inoculation of bacteria, and the progression of alveolar edema formation arising from the development of acute respiratory distress syndrome.
Currently, very few mathematical and computational models have been implemented to study chronic lung inflammation. Existing models of lung inflammation are not yet at a level where they can capture the rich dynamics of the complex interaction between inflammation and airway diseases. We therefore highlight the needs for developing mathematical and computational models dedicated to understanding acute and chronic inflammation both in healthy and diseased states of lung functioning. The findings of the review are organized into three sections. First, lung inflammatory responses in different airway diseases such as chronic obstructive pulmonary disease (COPD), asthma and cystic fibrosis are presented. Second, low-grade chronic inflammation in the airways of aged lungs is discussed. Third, reviews of existing mathematical and computational models for airway diseases are presented and the advantages of employing mathematical and computational models in the study of lung inflammation in airway diseases are discussed. We would like to note that this review is not meant to be a comprehensive coverage of the experimental and computational aspects of inflammation processes in airway diseases but rather a broad overview for researchers seeking to understand the inflammation process in lung airway diseases. The goal of this review is to foster research collaborations between experimentalist and modelers in the study of lung inflammation. This has the prospect of furthering our understanding of the physiological and pathological mechanisms that control inflammation in different airway diseases.
Inflammation mechanism in COPD
COPD is commonly viewed as a chronic disease in pulmonary tissue. The disease is mainly initiated by inhaling cigarette smoke into the pulmonary system and associated with a switch from a self-limiting inflammatory response to a chronic persistent inflammatory response [79]. Cigarette pollutants can directly trigger PRRs such as TLRs and purinergic receptors and dying-autophagic, apoptotic or necrotic-cells can indirectly release damage-associated molecular patterns (DAMPs) to initiate pattern recognition. Chemotactic factors attract inflammatory cells to the injured region. CC-chemokine ligand 2 (CCL2) acts on CC-chemokine receptor 2 (CCR2) to attract monocytes, chemokine C-X-C motif ligand 1 (CXCL1). CXCL8 act on CCR2 to attract neutrophils and monocytes which differentiate into macrophages in the lung for resolution process [80, 81]. CXCL9, CXCL10 and CXCL11 act on CXCR3 to attract T helper 1 (TH1) cells and type 1 cytotoxic T (TC1) cells [82]. Macrophages, epithelial cells and attracted inflammatory cells to the injured site release proteases, such as MMP9, which results in elastin degradation and emphysema [83] where the immune system switches to a TH17 response to promote inflammation [79]. Epithelial cells and macrophages also discharge transforming growth factor-β (TGF-β), which triggers fibroblast proliferation for tissue remodeling [84]. Airway smooth muscle produces inflammatory cytokines, proteases, and growth factors, which may contribute to the remodeling process and induce phenotypic changes of the smooth muscle in COPD (Fig. 2). Also, small airway-wall remodeling is proposed as reason for airflow limitation in COPD, decline in lung function, and poor responses to available therapies [85]. Cigarette smoke, oxidative stress and the airway inflammatory microenvironment are acknowledged as main parameters that have a direct effect on alveolar macrophages phenotype in COPD [86]. Several other mechanisms such as airway-wall remodeling, impaired macrophage clearance, chronic colonization and infection of the lower airways, oxidative stress, tissue hypoxia, genetic susceptibility, and epigenetic changes have been implicated in the persistence of the inflammatory response despite smoking cessation [87].

Inflammatory response in COPD: Cigarette pollutants trigger TLRs and apoptotic, necrotic and dead cells release DAMPs (Pattern recognition). Activated inflammatory cells recruit neutrophils and monocyte to injured region (Resolution). Recruited inflammatory cells to the injured site release elastase and MMP9, which results in mucus hypersecretion and elastin degradation and emphysema, respectively. Macrophages discharge TGF-β which triggers fibroblast proliferation (Tissue remodeling). Airway smooth muscle produces inflammatory cytokines, proteases, and growth factors, which may contribute to the remodeling process. TLRs: Toll-like-receptors, DAMPs: damage-associated molecular patterns, MMP9: matrix metalloproteinase-9 , TGF-β: transforming growth factor-β
Inflammation mechanism in asthma
Asthma is one of the most serious pulmonary-system diseases and it affects more than 300 million individuals around the world. The presence of airway inflammation in asthma was detected in the nineteenth century. Asthma leads to airway hyper-responsiveness, obstruction, mucus hyper-production and airway-wall remodeling [88]. Cytokines, allergens, chemokines, and infectious agents are the main stimuli that activate signaling pathways in epithelial cells in asthma [89]. Airway epithelial cells activate epithelial TLRs to recognize patterns of inflammatory stimuli in allergic disease [90, 91]. Then resolution process starts where antigen presenting cells (APCs) endocytose inhaled allergens, present them to naïve T cells, and activate mast cells by crosslinking surface-bound IgE molecules to release several bronchoconstrictor mediators, including cysteinyl leukotrienes and prostaglandin D2 [92]. Myeloid dendritic cells process allergens and release CCL17 and CCL22, which act on CCR4 to attract TH2 cells. TH2 cells release IL-4 and IL-13, IL-5 and IL-9 and have a central role in the pathogenesis of allergic asthma [93]. Epithelial cells release CCL11, which recruits eosinophils via CCR3. Eosinophils secrete a wide array of cytotoxic and pro-inflammatory mediators [94]. Natural killer (NK) cells and type 2 innate lymphoid cells (ILC2s) express the pro-resolving receptors ALX/FPR2 for lipoxin A4 (LXA4) and Chemokine-like receptor 1 (CMKLR1) that increases airway eosinophilia and antigen (Ag)-specific CD4+ T-cell clearance [95]. LXA4 inhibits NK-cell cytotoxicity and increases eosinophil-induced apoptosis by NK cells, and inhibits interleukin (IL)-13 release by ILC2s. In addition, eosinophils may contribute to resolution of inflammation in asthma and produce pro-resolving lipid mediators (PD1) and RvE3. Where PD1 and IL-10 secrete interleukin IL-10 and promote macrophage activation [96]. Patients with asthma may have a defect in regulatory T (TReg) cells, which may lead to further TH2-cell proliferation [97]. TGF-β is introduced as a main regulator of remodeling in the airways of asthmatics [93]. Platelet-derived growth factor (PDGF) promotes fibroblasts and ASM proliferation in the asthmatic lung [98, 99]. Injured epithelial cells releases stem-cell factor (SCF) which promote myofibroblasts differentiation and induce structural changes throughout airway-wall remodeling [100] (Fig. 3). Increase in angiogenesis, pro-angiogenic cytokine vascular endothelial growth factor (VEGF) and its receptors [101, 102] and dysregulation in production of extracellular matrix metalloproteinase (MMPs) [103] have been reported as proteinases responsible for the degradation of the extracellular matrix during tissue remodeling in asthmatic airways [104].

Inflammatory response in asthma: TLRs recognize patterns of allergens (Pattern recognition). Myeloid DC process allergens and release CCL17 and CCL22 to attract TH2 to injured region. IgE molecules sensitize mast cells to release cysteinyl leukotrienes and PGD2. Damaged epithelial cells release CCL11 to recruit eosinophils which attract more proinflammatory mediators to the damaged region. Eosinophils produce PD1 and PD1 secrets IL10 which promotes macrophage activation (Resolution). Damaged epithelial cells releases SCF to activate myofibroblast to repair damaged epithelial cells. TLRs: Toll-like-receptors, CCL: CC-chemokine ligand, TH2: T helper cells type 2, IgE: immunoglobulin E, PGD2: prostaglandin D2, SCF: stem-cell factor, PD1: pro-resolving lipid mediators
Inflammation mechanism in cystic fibrosis
Apart from COPD and asthma, cystic fibrosis (CF) is an inherited chronic disease that affects the lungs of about 70,000 children and adults worldwide (30,000 in the US). Mutation of the CF transmembrane conductance regulator (CFTR) gene results in CF [105]. Mutations in CFTR influence the lung epithelial innate immune function that leads to exaggerated and ineffective airway inflammation that fails to abolish pulmonary pathogens [106]. CFTR deficiency is associated with altered fluid and electrolyte homeostasis of epithelial cells and leads to unusually thick and viscose mucus that clogs small airways, and contributes to the development of persistent lung inflammation and an increased risk of lung infections [107]. Pathogen-associated molecular patterns (PAMPs) activate TLR-MyD88 signaling to increase NF-κB signaling [108]. TLRs and bacterial colonization activate neutrophils, macrophages and NF-κB-mediated inflammatory response to initiate the pathological process. Activated NF-κB result in production of inflammatory cytokines, such as IL-8 and High mobility group box 1 (HMGB1) protein, and recruitment of polymorphonuclear leukocyte (PMNs). HMGB1 increases pro-inflammatory cytokine expression via its cellular receptors. Increase in pro-inflammatory cytokine expression promotes toll-like receptor TLR-2 and TLR-4 production [109]. Intracellular TLR4 activation prevents interferon regulatory factor 3 (IRF3) translocation to the nucleus to activate type I IFN gene products, which are required for the activation of dendritic cells (DCs) and the clearance of some cystic fibrosis-related pathogens [110]. TH2 skews the inflammatory environment in cystic fibrosis. Abundant IL-8 stimulates airway epithelial and smooth muscle remodeling and induces greater contraction in CF airway smooth muscle than non-cystic fibrosis airway smooth muscle, which results in airway hyper-responsiveness [111]. Decreased function of peroxisome proliferator-activated receptor-g (PPARg) associates with low levels of carbonic anhydrases that contribute to increased mucus viscosity and results in enhanced pro-inflammatory signaling and cytokine secretion in CF cells (Fig. 4). High numbers of neutrophils at the site of chronic infection and decreased neutrophil apoptosis, phagocytic capacity of macrophage and levels of pro-resolving mediators suggest an impaired inflammatory resolution that promotes sustained infection [112, 113]. In addition, defective cilia function, increased mucus viscosity, hypoxia, free nutrients, damage to lung architecture, defective or decreased antimicrobials, TH2 and TH17 responses and ineffective cellular mediators, changes in virulence and direct downregulation of antimicrobial pathways contribute to infection and pulmonary decline in cystic fibrosis [114]. Airway remodeling in CF is presented as secondary to infection and inflammation [115]. MMPs are involved in tissue breakdown and repair and MMP-8 and MMP-9, which are mainly derived from neutrophils in the lower respiratory tract, are the most important group of endopeptidases in CF remodeling [116,117,118]. In addition, TGFα is thought to play a role in the regulation of airways remodeling with CF [119] and TH2 cytokines (especially IL-13) has been found during cycles of epithelial injury and repair of CF airways [120].

Inflammatory response in CF: TLRs recognize PAMPs (pattern recognition). TLRs and bacterial colonization activate inflammatory mediators like; neutrophils, macrophages and NF-κB. NF-κB produce IL8 and HMGB1 and recruit monocyte. Type I IFN activates DCs to clear cystic fibrosis-related pathogens and TH2 skew CF (Resolution). IL8 stimulate damaged epithelial cells (Tissue remodeling). PAMPs: Pathogen-associated molecular patterns, TLRs: Toll-like-receptors, NF-κB: nuclear factor kappa-light-chain-enhancer of activated B-cells, IL-8: proinflammatory cytokines interleukin 8, HMGB1: High mobility group box 1, IFN: Interferon, DCs: dendritic cells
The contribution of harmful stimuli and inflammatory mediators in pattern recognition, resolution and remodeling process are classified for discussed disease condition in Table 1.
Inflammaging mechanism in airways
All vital organs lose their function with age. Human lung matures up to age 20–25 years and will start to lose functionality after about 35 years. Breathing existent pollutants in the environment or exogenous oxidants in young or healthy individuals causes cellular damage in lung tissue [121]. If the damage is too extreme, cells would sustain senescence to prevent oncogenic changes. Senescence signaling activates stem cells to replace damaged cells [122]. An increase in senescent cells and corresponding senescence-associated secretory phenotype can induce further inflammation, alveolar destruction, endothelial dysfunction [123]. In addition, excessive ROS will increase damage to cells by a defective repair mechanism in the elderly. Aging and ROS induce loss of quiescence and stem-cell senescence, which result in loss of stem cells’ renewal [122]. In classic aging pathways, growth factor signaling activates PI3K, phospho-AKT and mTOR, which accelerate aging [124,125,126]. Inhibition of mTOR signaling extends life span [127]. Antiaging molecules such as phosphatase and tensin homolog (PTEN) inhibits PI3K and AMPK prevent hyperactivation of the mTOR signaling pathway. Sirtuins (SIRT1 and SIRT6) upregulate FOXO3A and promotes autophagy [124, 128, 129]. Defective mechanism of positive regulators (SIRT1, SIRT6, PTEN, and AMPK) will induce cytokine, chemokine, and ribosomal synthesis and secrete growth factors favoring cell proliferation and growth (Fig. 5). COPD is identified with an elevated ROS level and ROS are able to change biological molecules, signaling pathways and antioxidant molecule function. A decrease in the level of PTEN and SIRT1 in COPD would lead to activation of the mTOR-aging pathway via PI3K activation by ROS. This results in reduced antioxidant defense by FOXO3A inhibition and a loss of autophagy. Loss of autophagy can prevent the clearance of defective mitochondria and further increase ROS production [130]. Defective autophagy decreases immune response to bacteria and cellular homoeostasis in COPD. In addition, an excessive level of ROS promotes NF-κB/AP-1 activation and chronic inflammation [131, 132].

Inflammaging mechanism in airways: ROS increase damage in airways epithelial cells. Growth factor signaling activate PI3K, phospho-AKT and mTOR signaling which accelerate aging in airways. PTEN and AMPK inhibit discussed factors that can lead to increase in life span. SIRT1 upregulate FOXO3A that functions as a trigger for apoptosis of damaged cells. SIRT1 also promotes autophagy. Effecting mechanism of SIRT1 will induce cytokine, chemokine and ribosomal synthesis and secrete growth factors favoring cell proliferation and growth. ROS: Reactive oxygen species, PI3K: Phosphoinositide 3-kinase, mTOR: mechanistic target of rapamycin, PTEN: phosphatase and tensin homolog , FOXO3: Forkhead box O3, SIRT1: Sirtuin 1
Experimental observation of inflammation in airway diseases
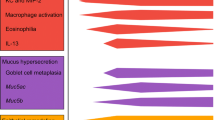
Asthma and COPD occur due to chronic inflammation of the airways. However, the mechanism of action is different. In asthma, mast cells, eosinophils and CD4 T lymphocytes represent the predominant cell types in the inflammatory process. In COPD, neutrophils, macrophages and CD8 T lymphocytes are the predominant cell types in the inflammatory process [133,134,135]. In CF, neutrophils are the predominant cell types in the inflammatory process and they release oxidants, proteases, and elastase that causes respiratory exacerbations [136].
Patients with COPD exhibit reduced airway caliber because of cell damage induced by external toxic agents such as cigarette smoke [134, 137, 138]. There is a positive correlation between inflammation intensity and COPD severity. At the final stages of the disease, the inflammatory process becomes very intense. The intensity of inflammation may be combated through the application of anti-inflammatory therapies [134, 139]. Anti-inflammatory therapies have the potential of combating CF and asthma, but care must be taken to avoid suppressing critical elements of the inflammatory response, which in turn may worsen the disease [136, 139]. Inflammatory responses are numerous and include transport of plasma from the blood into the injured tissues, biochemical signaling cascades, and the mobilization of cytokines, such as interleukins [140]. The complexity of the inflammation process suggests that strategies for developing effective and efficient therapeutic interventions for combating airway diseases would greatly benefit from predictions obtained from mathematical and computational modeling. For example, correlation of imaging measurements with disease severity would be useful in understanding the pathophysiology behind different airway diseases and guide the development of therapeutic interventions. In addition, computational models of lung tissue may aid in the study of lung tissue mechanics during an inflammatory process.
Aging is a complex process that occurs in different cell types and tissues and is controlled by environmental, genetic, stochastic, epigenetic events and their long-term interactions [141]. Inflammaging is associated with most of the age-related diseases but its precise etiology and potential causal role remain largely unknown [141]. An understanding of the mechanism of lung inflammaging is therefore important in determining whether treatments that modulate inflammaging may be beneficial in combating age-related airway diseases.
Mathematical modeling of lung inflammation
Mathematical models represent the essential characteristics of a system as a set of mathematical equations. They are useful in testing different hypotheses about the working of a system and their utility is established by matching their outputs with experimental observations. The study of inflammation is somewhat difficult because of the myriad inflammatory mediators involved and their effects on target tissues. The coordinated functions of these mediators and their multiple modes of regulation remain largely unknown [142]. Mathematical models are vital tools that would help in deciphering the dynamic behavior of these networks. Analysis of a model often provides insights into the underlying mechanisms for the regulation of the system, and this may drive formulation of new hypotheses that would in turn lead to new rounds of experiments [143].
Mechanistic models of inflammation may be classified as discrete-time or continuous-time models. Discrete-time models describe the changes in the system at certain time points with no information of its behavior at intervals between these time points. Discrete-time models such as agent-based models (ABMs) represent an inflammatory mediator as an agent (i.e., discrete entity with its own goal and behavior) that has the ability to adapt to its microenvironment and modify its behavior [49, 144]. Agent simulations are governed by local interactions among agents and can incorporate the stochasticity of the inflammatory process. Continuous-time models represent the system as continuous over time and usually manifest as differential equations [145]. Most continuum models of inflammation use ordinary differential equations (ODEs) to describe the dynamics of an inflammation response. Some models use partial differential equations (PDEs) in place of ODEs or a combination of both [54, 146]. Given the time frame (> 1 day) at which inflammation occurs, the spatial variations in distribution of inflammatory mediators may be assumed to be negligible compared to the time variations. Thus, ODEs may be better suited for modeling the inflammation process over several days. However, to study the spatial distribution of inflammatory mediators and their effect on the progress of an inflammation process, PDE models would be a better option. ODEs and PDEs that model the complex dynamics of an inflammatory response are mostly nonlinear, and their exact or analytical solutions are difficult and sometimes impossible to obtain. The application of techniques for solving differential equations based on numerical approximations is required for finding approximate solutions for nonlinear differential equations. Numerical algorithms for the numerical approximation of nonlinear differential equations produce computational models that are easily simulated on computers to obtain approximate solutions.
Mathematical and computational models have been developed to study the physiological functioning of the lungs and relatively few have focused on obstructive lung diseases [69, 147]. Most of the models of obstructive lung diseases do not incorporate the effect of inflammation [72,73,74,75].
Computational models of inflammation in asthma
Chernyavsky et al. [148] used a theoretical model to identify the role of inflammation resolution speed in airway smooth muscle mass accumulation in asthma. They present a mathematical model that describes qualitatively the growth dynamics of airway smooth muscle cells over short and long terms in the normal and inflammatory environments often observed in asthma. Their model predicts that long-term airway smooth muscle growth is influenced by the inflammation resolution speed, the inflammation magnitude, and the frequency of inflammatory episodes. Their model highlights the importance of the resolution speed of inflammation in the long-term management of asthma. A limitation of their model is that it does not account for the mechanical interaction of the cells between each other and with the extracellular matrix that could affect the growth and apoptosis rates as well as the total capacity of an airway wall. In addition, the model neglects the spatially heterogeneous and anisotropic growth observed in micrographs and cell hypertrophy [148, 149].
A study by Lee et al. [147] used a system of ODEs to investigate macrophage response to respiratory viral infection in normal and asthmatic conditions. Their model describes two types of macrophages that play complementary roles in fighting viral infections: classical-activated macrophages and alternative-activated macrophages. Classical-activated macrophages destroy infected cells and tissues to remove viruses, while alternative-activated macrophages repair damaged tissues. They describe populations of viruses and airway epithelial cells, concentrations of cytokines (such as IFN- β and IL-4) and enzymes (such as iNOS and arginase-1) secreted by the cells. After an infection, the airway epithelial cells are directly infected by the virus and the type I interferon they produce. Airway epithelial cells are defined to be in two states, dormant and activated. Dormant epithelial cells transition to the activated state upon exposure to virus. After epithelial cells have been infected and begun to respond, alveolar macrophages take control of the defense system. The balance between classically activated macrophages and alternatively activated macrophages is controlled by the cytokines IFNb and IL4. They investigate how viral infections alter the balance of the alveolar macrophage system and potentially trigger asthma exacerbations. In particular, they investigate how respiratory viral infection changes the balance between classical-activated macrophages and alternative-activated macrophages and how this response differs in hosts with asthma-like conditions, and how those differences can lead to accentuated symptoms.
Their simulation results show that a higher viral load or longer duration of infection provokes a stronger immune response from the macrophage system. Their result also showed that the differences in response to respiratory viral infection in normal and asthmatic subjects skews the system toward a response that generates more severe symptoms in asthmatic patients. Thus, respiratory viral infection can aggravate symptoms in asthmatic patients [147].
Kim et al. [75] presented a mathematical model consisting of a system of PDEs to study the regulation of type I (Th1) versus type II (Th2) helper T cells in asthma development. Airway exposure levels of lipopolysaccharide (LPS) determined type I versus type II helper T cell-induced experimental asthma. While high LPS levels induce Th1-dominant responses, low LPS levels derive Th2 cell-induced asthma. Their model describes the behaviors of T cells (Th0, Th1, Th2 and macrophages) and regulatory molecules (IFN-γ, IL-4, IL-12, TNF-α) in response to high, intermediate, and low levels of LPS. The simulation results showed how variations in the levels of injected LPS affect the development of Th1 or Th2 cell responses through differential cytokine induction.
Computational models of inflammation in COPD
A few mathematical models have also been developed to study COPD. An example is the model presented by Cheng et al. [72] investigating the effect of post coinfection with influenza A virus and Streptococcus pneumoniae. The model investigated coinfection interactions between influenza and Streptococcus pneumoniae through identifying variations in cytokine level, reflecting severity in inflammatory response. Their modeling framework is based on the mathematical within-host dynamics of coinfection with influenza A virus and Streptococcus pneumoniae developed in Smith et al. [153, 154]. Results from their study showed that Streptococcus pneumoniae may be a risk factor for COPD exacerbations. It further showed that the day of secondary Streptococcus pneumoniae infection had much more impact on the severity of inflammatory responses in pneumonia compared to the effects caused by initial virus titers and bacteria loads.
Cox [73] developed a system of ODEs to investigates how COPD can be caused by sustained exposure to cigarette smoke (CS) (or other pro-inflammatory agents). The ODEs represent possible quantitative causal relations among key variables, such as alveolar macrophages and neutrophil levels in the lung, levels of tissue-deteriorating enzymes, and rates of apoptosis, repair, and net destruction of the alveolar wall [73]. Their model explains irreversible degeneration of lung tissue as resulting from a cascade of positive feedback loops: a macrophage inflammation loop, a neutrophil inflammation loop, and an alveolar epithelial-cell apoptosis loop; and illustrates how to simplify and make more understandable, the main aspects of the very complex dynamics of COPD initiation and progression, as well as how to predict the effects on risk of interventions that affect specific biological responses.
An advantage of their model is the possibility of quantifying how interventions that change the times to activate different major feedback loops will affect the time course of the disease [73].
Computational models of inflammation in cystic fibrosis
Liquid hyperabsorption, airway surface dehydration, and impaired mucociliary clearance is prevalent in CF lung disease [155]. Markovetz et al. [155] implemented a system of ordinary differential equations based on functional imaging data to investigate the mucociliary clearance and absorption of aerosolized radiolabeled particle and small molecules probes from human subjects with and without CF. Their model captures the mucociliary clearance and liquid dynamics of the hyperabsorptive state in CF airways and the mitigation of that state by hypertonic saline treatment. Results from their study suggest that patients with CF have regions of airway with diminished mucociliary clearance function that can be recruited with hypertonic saline treatment.
Airway remodeling is a common factor in CF lung disease. Brown et al. [156] used an ABM to examine the response of an abstracted population of inflammatory cells and cells involved in remodeling to particulate exposure in the lung. The model focuses on relevant interactions among macrophages, fibroblasts, a pro-inflammatory cytokine (TNF-α), an anti-inflammatory cytokine (TGF-β1), collagen deposition, and tissue damage. Numerical simulations of the model gives three distinct states that equate with (1) self-resolving inflammation and a return to baseline, (2) a pro-inflammatory process of localized tissue damage and fibrosis, and (3) elevated pro- and anti-inflammatory cytokines, persistent tissue damage, and fibrosis outcomes. These states depend on the degree and duration of exposure and are consistent with experimental results from histology sections of lung tissue from mice exposed to particulate matter [156]. An advantage of their model is the ability to capture some of the important features of inflammation following exposure of the lung to particulate matter.
In summary, mathematical models of inflammation have contributed to our knowledge of the mechanism of action in lung diseases. There is need to develop a unified approach for modeling lung diseases that accounts for the different phenomena occurring at different spatial levels. Models that link the interactions at the molecular, cellular and tissue-level would provide a systems perspective to the pathology of lung diseases.
Multiscale modeling of lung inflammation and the aging process
Lung inflammation is a complex process and its onset and progress depends on the coordinated interactions involving different proteins, networks, tissues and other organs (e.g., in sepsis). Due to the large number of mediators involved in the inflammation process, it is often difficult to decipher the individual and collective control of mediators across the different spatial scales. The role of proteins, networks, tissues and other organs on local and systemic inflammation can be elicited using mathematical and computational models.
Multiscale mechanistic models link cellular and molecular processes to tissue-level behavior during injury. Such models have the capability to provide invaluable insight into the system-level regulation of inflammation. Computational mechanistic models are well-suited for such problems and are useful in understanding system-level operations. They can be used to test different hypotheses formulated to investigate the changes at the molecular and cellular-level that lead to the onset and progress of inflammation. Excellent multiscale models of asthmatic airway hyper-responsiveness and airway constriction have been developed by Donovan [157], Politi et al. [158], Venegas et al. [159] and Amin et al. [160]. There is need to extend these complex models to incorporate the dynamics of the inflammation process.
A typical multiscale mechanistic model may involve a combination of some or all of the following: a biomechanical model describing tissue-biomechanical response from trauma or infection; ordinary differential equations, partial differential equations and/or a reaction–diffusion system that describe the diffusion and kinetics of molecular mediators and migration of immune cells during the inflammation process [161,162,163,164]. Applications of digital image analysis in computational simulations may be utilized in studying how changes in tissue properties affect the expression and transport of inflammatory mediators across different spatial scales. Hybrid multiscale models couple continuum models and discrete models within different spatial scales [59, 77, 161,162,163,164,165,166,167,168]. Continuum models describing tissue-level behavior, may be coupled to agent-based models to describe the migration of immune cells (such as macrophages, T-cells and B-cells) to the site of injury [59, 77, 163, 164]. Agent-based models can incorporate stochasticity that exists in cellular-level processes and is inherent in biological systems [76, 162].
Experimental biologists usually adopt a reductionist approach, which may fail to describe system-level behavior. Mathematical and computational models though vital, may not give useful information when applied in isolation to biological/experimental findings. However, mathematical and computational models are invaluable when used with experimental approaches and have the potential of helping further knowledge on the complex inflammation process.
Aging represents a gradual deterioration of organization at the molecular, cellular, tissue, organ and system level of the body. Changes at the molecular and cellular-level would affect the working of the body at the tissue, organ and system-level and may impair the inflammation process leading to chronic inflammation or sepsis. The myriad inflammatory mediators involved in the inflammation process make it difficult to experimentally study age-related anomalies. Numerous studies have shown that low-grade inflammation is a common decimal in aging. Inflammaging is marked by a general increase in the production of pro-inflammatory cytokines and inflammatory markers [169]. The mechanism by which the low-grade inflammation is activated remains unknown. Computational modeling is a powerful tool that could help unravel the complexity of chronic inflammation including age-related inflammation. Using mathematical models that accurately represent the lung, we can study the interactions across various biological scales and make predictions for future outcomes of existing interactions based on currently available experimental data, which might otherwise not be possible.
Multiscale mechanistic models that couple cellular and molecular processes to tissue-level behavior could be implemented to test different hypotheses that explain how changes at the molecular and cellular-level may influence the onset and progress of chronic inflammation in aging subjects. Correlation between tissue properties, magnitude and duration of stress a tissue is exposed to and the molecular response during aging is necessary to understand inflammaging. Development and analysis of such models would provide insights into the process of aging and help physicians implement therapeutic strategies to address the aging process and treat diseases. Computational models have been developed to study the aging process [170,171,172,173]. Mc Auley and Mooney [171] used a computational model to study lipid metabolism and aging. Weinberg et al. [170] developed a computational model to study aging and calcification in an aortic heart valve. More information on models that have been developed within the last 50–60 years to study cellular aging can be found in the review by Witten [174]. More research is needed to understand the aging process at the cellular, organ and system-level and computational modeling is a valuable tool that could be used to further our understanding of aging and age-related diseases.
Summary and future directions
This paper reviews key mechanisms of inflammation in airway diseases. It discusses the role of mathematical and computational modeling in furthering our understanding of the complex inflammation mechanism in airway diseases. Results from experimental studies have greatly improved our knowledge of the cellular and molecular events that are involved in the acute inflammatory response to infection and tissue injury in many organs [175,176,177,178,179]. Experimental studies usually use reductionist approach, so they may fail to describe system-level behavior accurately. Mathematical and computational models can be employed to study the interactions across various biological scales and make predictions for future outcomes of existing interactions based on currently available experimental data.
We recommend that multiscale models should be implemented to test hypotheses that explain how changes at the molecular and cellular-levels may influence the onset and progress of chronic inflammation. Multiscale models should also be used to investigate how chronic inflammation could be caused by prolonged exposure to different kinds/levels of trauma, increased activation and diffusion of chemotactic attractants or high levels of inflammatory cytokines at a site of injury. Multiscale models could be employed to understand the tissue microenvironment effects on inflammation mechanism in young and aged lungs.
Computational models have been used to investigate the influence of inflammatory mediators [73, 147] and variables such as resolution speed, degree and location of stimuli, post coinfections on remodeling [72, 148, 150, 151, 156], severity [152] and development [73, 75] of airways’ disease and aging process [170,171,172,173,174]. Despite all conducted computational and experimental studies on lung inflammation mechanism, there is lack of details on molecular mechanisms and pathways that contribute to activation of low-grade inflammation and onset of chronic inflammation in lung. There is need for models that link the interactions at the molecular, cellular and tissue-levels to provide a systems perspective to the pathology of inflammatory mechanism in lung diseases. More research is needed to understand the mechanisms that produce acute or systemic chronic inflammation which occurs in many diseases such as autoimmune diseases, obesity, cardiovascular diseases, type 2 diabetes, among many others [142, 180,181,182].
References
Ahmed AU. An overview of inflammation: mechanism and consequences. Frontiers in Biology. 2011;6(4):274–81.
Ward P. Acute lung injury: how the lung inflammatory response works. Eur Respir Soc; 2003;44:22s–23s
Lee G, Walser TC, Dubinett SM. Chronic inflammation, chronic obstructive pulmonary disease, and lung cancer. Curr Opin Pulm Med. 2009;15(4):303–7.
Takeuchi O, Akira S. Pattern recognition receptors and inflammation. Cell. 2010;140(6):805–20.
Ortega-Gómez A, Perretti M, Soehnlein O. Resolution of inflammation: an integrated view. EMBO Mol Med. 2013;5(5):661–74.
Maskrey BH, Megson IL, Whitfield PD, Rossi AG. Mechanisms of resolution of inflammation. Arterioscler Thromb Vasc Biol. 2011;31(5):1001–6.
Najar M, Krayem M, Merimi M, Burny A, Meuleman N, Bron D, et al. Insights into inflammatory priming of mesenchymal stromal cells: functional biological impacts. Inflamm Res. 2018. https://doi.org/10.1007/s00011-018-1131-1.
Lumb AB. Nunn’s applied respiratory physiology eBook. Amsterdam: Elsevier Health Sciences; 2016.
Tripathi P, Aggarwal A. NF-kB transcription factor: a key player in the generation of immune response. Curr Sci Bangalore. 2006;90(4):519.
Grommes J, Soehnlein O. Contribution of neutrophils to acute lung injury. Mol Med. 2011;17(3–4):293.
Lee I-T, Yang C-M. Inflammatory signalings involved in airway and pulmonary diseases. Mediat Inflamm. 2013;2013:791231.
Moldoveanu B, Otmishi P, Jani P, Walker J, Sarmiento X, Guardiola J, et al. Inflammatory mechanisms in the lung. J Inflamm Res. 2009;2:1–11.
Nelson RJ. Seasonal immune function and sickness responses. Trends Immunol. 2004;25(4):187–92.
Nelson RJ, Demas GE. Seasonal changes in immune function. Q Rev Biol. 1996:511–48.
Colgan SP, Curtis VF, Campbell EL. The inflammatory tissue microenvironment in IBD. Inflamm Bowel Dis. 2013;19(10):2238.
Dantzer R. Cytokine-induced sickness behavior: where do we stand? Brain Behav Immun. 2001;15(1):7–24.
Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860–7.
Chung K, Adcock I. Multifaceted mechanisms in COPD: inflammation, immunity, and tissue repair and destruction. Eur Respir J. 2008;31(6):1334–56.
Hartupee J, Mann DL. Role of inflammatory cells in fibroblast activation. J Mol Cell Cardiol. 2016;93:143–8.
Baylis D, Bartlett DB, Patel HP, Roberts HC. Understanding how we age: insights into inflammaging. Longev Healthspan. 2013;2(1):8.
Libby P. Inflammatory mechanisms: the molecular basis of inflammation and disease. Nutr Rev. 2007;65(suppl_3):140-S6.
Brodland GW. How computational models can help unlock biological systems. Semin Cell Dev Biol. 2015;47–48:62–73. https://doi.org/10.1016/j.semcdb.2015.07.001.
Vodovotz Y. Computational modelling of the inflammatory response in trauma, sepsis and wound healing: implications for modelling resilience. Interface Focus. 2014;4(5):20140004. https://doi.org/10.1098/rsfs.2014.0004.
Fletcher AG, Osterfield M, Baker RE, Shvartsman SY. Vertex models of epithelial morphogenesis. Biophys J. 2014;106(11):2291–304. https://doi.org/10.1016/j.bpj.2013.11.4498.
Fletcher AG, Cooper F, Baker RE. Mechanocellular models of epithelial morphogenesis. Philos Trans R Soc Lond B Biol Sci. 2017;372(1720). https://doi.org/10.1098/rstb.2015.0519.
George UZ, Bokka KK, Warburton D, Lubkin SR. Quantifying stretch and secretion in the embryonic lung: Implications for morphogenesis. Mech Dev. 2015;138(Pt 3):356–63. https://doi.org/10.1016/j.mod.2015.07.003.
Lubkin SR, Murray JD. A mechanism for early branching in lung morphogenesis. J Math Biol. 1995;34(1):77–94.
Clément R, Douady S, Mauroy B. Branching geometry induced by lung self-regulated growth. Phys Biol. 2012;9(6):066006. https://doi.org/10.1088/1478-3975/9/6/066006.
Iber D, Menshykau D. The control of branching morphogenesis. Open Biol. 2013;3(9):130088. https://doi.org/10.1098/rsob.130088.
Varner VD, Nelson CM. Computational models of airway branching morphogenesis. Semin Cell Dev Biol. 2017;67:170–6. https://doi.org/10.1016/j.semcdb.2016.06.003.
Tran K, Smith NP, Loiselle DS, Crampin EJ. A metabolite-sensitive, thermodynamically constrained model of cardiac cross-bridge cycling: implications for force development during ischemia. Biophys J. 2010;98(2):267–76. https://doi.org/10.1016/j.bpj.2009.10.011.
Washio T, Okada JI, Sugiura S, Hisada T. Approximation for cooperative interactions of a spatially-detailed cardiac sarcomere model. Cell Mol Bioeng. 2012;5(1):113–26. https://doi.org/10.1007/s12195-011-0219-2.
Dewan S, McCabe KJ, Regnier M, McCulloch AD. Insights and challenges of multi-scale modeling of sarcomere mechanics in cTn and Tm DCM mutants-genotype to cellular phenotype. Front Physiol. 2017;8:151. https://doi.org/10.3389/fphys.2017.00151.
Constantino J, Hu Y, Trayanova NA. A computational approach to understanding the cardiac electromechanical activation sequence in the normal and failing heart, with translation to the clinical practice of CRT. Prog Biophys Mol Biol. 2012;110(2–3):372–9. https://doi.org/10.1016/j.pbiomolbio.2012.07.009.
Lopez-Perez A, Sebastian R, Ferrero JM. Three-dimensional cardiac computational modelling: methods, features and applications. Biomed Eng Online. 2015;14:35. https://doi.org/10.1186/s12938-015-0033-5.
Trayanova NA. Whole-heart modeling: applications to cardiac electrophysiology and electromechanics. Circ Res. 2011;108(1):113–28. https://doi.org/10.1161/CIRCRESAHA.110.223610.
Friedrich J, Lengyel M. Goal-directed decision making with spiking neurons. J Neurosci. 2016;36(5):1529–46. https://doi.org/10.1523/JNEUROSCI.2854-15.2016.
Rustichini A, Conen KE, Cai X, Padoa-Schioppa C. Optimal coding and neuronal adaptation in economic decisions. Nat Commun. 2017;8(1):1208. https://doi.org/10.1038/s41467-017-01373-y.
Cumming BD, McElwain DL, Upton Z. A mathematical model of wound healing and subsequent scarring. J R Soc Interface. 2010;7(42):19–34. https://doi.org/10.1098/rsif.2008.0536.
Flegg JA, Byrne HM, Flegg MB, McElwain DL. Wound healing angiogenesis: the clinical implications of a simple mathematical model. J Theor Biol. 2012;300:309–16. https://doi.org/10.1016/j.jtbi.2012.01.043.
Sherratt JA, Dallon JC. Theoretical models of wound healing: past successes and future challenges. C R Biol. 2002;325(5):557–64.
Patel AA, Gawlinski ET, Lemieux SK, Gatenby RA. A cellular automaton model of early tumor growth and invasion. J Theor Biol. 2001;213(3):315–31. https://doi.org/10.1006/jtbi.2001.2385.
Powathil G, Kohandel M, Sivaloganathan S, Oza A, Milosevic M. Mathematical modeling of brain tumors: effects of radiotherapy and chemotherapy. Phys Med Biol. 2007;52(11):3291–306. https://doi.org/10.1088/0031-9155/52/11/023.
Anderson AR, Chaplain MA. Continuous and discrete mathematical models of tumor-induced angiogenesis. Bull Math Biol. 1998;60(5):857–99. https://doi.org/10.1006/bulm.1998.0042.
McDougall SR, Anderson AR, Chaplain MA. Mathematical modelling of dynamic adaptive tumour-induced angiogenesis: clinical implications and therapeutic targeting strategies. J Theor Biol. 2006;241(3):564–89. https://doi.org/10.1016/j.jtbi.2005.12.022.
Vodovotz Y, Chow CC, Bartels J, Lagoa C, Prince JM, Levy RM, et al. In silico models of acute inflammation in animals. Shock. 2006;26(3):235–44. https://doi.org/10.1097/01.shk.0000225413.13866.fo.
Day J, Rubin J, Vodovotz Y, Chow CC, Reynolds A, Clermont G. A reduced mathematical model of the acute inflammatory response II. Capturing scenarios of repeated endotoxin administration. J Theor Biol. 2006;242(1):237–56. https://doi.org/10.1016/j.jtbi.2006.02.015.
Reynolds A, Rubin J, Clermont G, Day J, Vodovotz Y, Bard Ermentrout G. A reduced mathematical model of the acute inflammatory response: I. Derivation of model and analysis of anti-inflammation. J Theor Biol. 2006;242(1):220–36. https://doi.org/10.1016/j.jtbi.2006.02.016.
Dong X, Foteinou PT, Calvano SE, Lowry SF, Androulakis IP. Agent-based modeling of endotoxin-induced acute inflammatory response in human blood leukocytes. PLoS One. 2010;5(2):e9249. https://doi.org/10.1371/journal.pone.0009249.
Kumar R, Clermont G, Vodovotz Y, Chow CC. The dynamics of acute inflammation. J Theor Biol. 2004;230(2):145–55. https://doi.org/10.1016/j.jtbi.2004.04.044.
Álvarez E, Toledano V, Morilla F, Hernández-Jiménez E, Cubillos-Zapata C, Varela-Serrano A, et al. A system dynamics model to predict the human monocyte response to endotoxins. Front Immunol. 2017;8:915. https://doi.org/10.3389/fimmu.2017.00915.
Brown D, Namas RA, Almahmoud K, Zaaqoq A, Sarkar J, Barclay DA, et al. Trauma in silico: Individual-specific mathematical models and virtual clinical populations. Sci Transl Med. 2015;7(285):285ra61. https://doi.org/10.1126/scitranslmed.aaa3636.
Abboud A, Mi Q, Puccio A, Okonkwo D, Buliga M, Constantine G, et al. Inflammation following traumatic brain injury in humans: insights from data-driven and mechanistic models into survival and death. Front Pharmacol. 2016;7:342. https://doi.org/10.3389/fphar.2016.00342.
Barber J, Tronzo M, Harold Horvat C, Clermont G, Upperman J, Vodovotz Y, et al. A three-dimensional mathematical and computational model of necrotizing enterocolitis. J Theor Biol. 2013;322:17–32. https://doi.org/10.1016/j.jtbi.2012.11.018.
Swan AJ, Tawhai MH. Evidence for minimal oxygen heterogeneity in the healthy human pulmonary acinus. J Appl Physiol (1985). 2011;110(2):528–37. https://doi.org/10.1152/japplphysiol.00888.2010.
Hewitt TJ, Hattler BG, Federspiel WJ. A mathematical model of gas exchange in an intravenous membrane oxygenator. Ann Biomed Eng. 1998;26(1):166–78.
Brighenti C, Gnudi G, Avanzolini G. A simulation model of the oxygen alveolo-capillary exchange in normal and pathological conditions. Physiol Meas. 2003;24(2):261–75.
De Backer JW, Vos WG, Gorlé CD, Germonpré P, Partoens B, Wuyts FL, et al. Flow analyses in the lower airways: patient-specific model and boundary conditions. Med Eng Phys. 2008;30(7):872–9. https://doi.org/10.1016/j.medengphy.2007.11.002.
Aghasafari P, Bin M, Ibrahim I, Pidaparti R. Strain-induced inflammation in pulmonary alveolar tissue due to mechanical ventilation. Biomech Model Mechanobiol. 2017. https://doi.org/10.1007/s10237-017-0879-5.
Pidaparti RM, Koombua K. Tissue strains induced in airways due to mechanical ventilation. Mol Cell Biomech. 2011;8(2):149–68.
Pidaparti RM, Swanson J. Effect of mechanical ventilation waveforms on airway wall shear. J Med Eng Technol. 2015;39(1):1–8. https://doi.org/10.3109/03091902.2014.968675.
Yin Y, Choi J, Hoffman EA, Tawhai MH, Lin CL. A multiscale MDCT image-based breathing lung model with time-varying regional ventilation. J Comput Phys. 2013;244:168–92. https://doi.org/10.1016/j.jcp.2012.12.007.
Swan AJ, Clark AR, Tawhai MH. A computational model of the topographic distribution of ventilation in healthy human lungs. J Theor Biol. 2012;300:222–31. https://doi.org/10.1016/j.jtbi.2012.01.042.
Roth CJ, Yoshihara L, Ismail M, Wall WA. Computational modelling of the respiratory system: discussion of coupled modeling approaches and two recent extensions. Comput Methods Appl Mech Eng. 2017;314:473–93.
Burrowes KS, Clark AR, Tawhai MH. Blood flow redistribution and ventilation-perfusion mismatch during embolic pulmonary arterial occlusion. Pulm Circ. 2011;1(3):365–76. https://doi.org/10.4103/2045-8932.87302.
Tang BT, Fonte TA, Chan FP, Tsao PS, Feinstein JA, Taylor CA. Three-dimensional hemodynamics in the human pulmonary arteries under resting and exercise conditions. Ann Biomed Eng. 2011;39(1):347–58. https://doi.org/10.1007/s10439-010-0124-1.
Rausch SM, Martin C, Bornemann PB, Uhlig S, Wall WA. Material model of lung parenchyma based on living precision-cut lung slice testing. J Mech Behav Biomed Mater. 2011;4(4):583–92. https://doi.org/10.1016/j.jmbbm.2011.01.006.
Berger L, Bordas R, Burrowes K, Grau V, Tavener S, Kay D. A poroelastic model coupled to a fluid network with applications in lung modelling. Int J Numer Method Biomed Eng. 2016;32(1):e02731. https://doi.org/10.1002/cnm.2731.
Burrowes KS, Doel T, Brightling C. Computational modeling of the obstructive lung diseases asthma and COPD. J Transl Med. 2014;12(Suppl 2):5. https://doi.org/10.1186/1479-5876-12-S2-S5.
Kim J, Heise RL, Reynolds AM, Pidaparti RM. Quantification of age-related lung tissue mechanics under mechanical ventilation. Med Sci (Basel). 2017. https://doi.org/10.3390/medsci5040021.
Kim J, Heise RL, Reynolds AM, Pidaparti RM. Aging effects on airflow dynamics and lung function in human bronchioles. PLoS One. 2017;12(8):e0183654. https://doi.org/10.1371/journal.pone.0183654.
Cheng YH, You SH, Lin YJ, Chen SC, Chen WY, Chou WC, et al. Mathematical modeling of postcoinfection with influenza A virus and Streptococcus pneumoniae, with implications for pneumonia and COPD-risk assessment. Int J Chron Obstruct Pulmon Dis. 2017;12:1973–88. https://doi.org/10.2147/COPD.S138295.
Cox LA. A causal model of chronic obstructive pulmonary disease (COPD) risk. Risk Anal. 2011;31(1):38–62. https://doi.org/10.1111/j.1539-6924.2010.01487.x.
Brown BN, Price IM, Toapanta FR, DeAlmeida DR, Wiley CA, Ross TM, et al. An agent-based model of inflammation and fibrosis following particulate exposure in the lung. Math Biosci. 2011;231(2):186–96. https://doi.org/10.1016/j.mbs.2011.03.005.
Kim Y, Lee S, Kim YS, Lawler S, Gho YS, Kim YK, et al. Regulation of Th1/Th2 cells in asthma development: a mathematical model. Math Biosci Eng. 2013;10(4):1095–133.
Reynolds A, Koombua K, Pidaparti RM, Ward KR. Cellular automata modeling of pulmonary inflammation. Mol Cell Biomech. 2012;9(2):141–56.
Ibrahim I, Oruganti SV, Pidaparti R. Simulation of Healing Threshold in Strain-Induced Inflammation through a discrete informatics model. IEEE J Biomed Health Inform. 2017. https://doi.org/10.1109/JBHI.2017.2669729.
W GA,M. S. C. Agent-based modeling approaches to multi-scale systems biology: an example agent-based model of acute pulmonary inflammation. In: Prokop A, Csukás B, editors. Systems biology. Dordrecht: Springer; 2013. pp. 429–61.
Lane N, Robins RA, Corne J, Fairclough L. Regulation in chronic obstructive pulmonary disease: the role of regulatory T-cells and Th17 cells. Clin Sci. 2010;119(2):75–86.
Donnelly LE, Barnes PJ. Chemokine receptors as therapeutic targets in chronic obstructive pulmonary disease. Trends Pharmacol Sci. 2006;27(10):546–53.
Traynor TR, Herring AC, Dorf ME, Kuziel WA, Toews GB, Huffnagle GB. Differential roles of CC chemokine ligand 2/monocyte chemotactic protein-1 and CCR2 in the development of T1 immunity. J Immunol. 2002;168(9):4659–66.
Barnes PJ. Cellular and molecular mechanisms of asthma and COPD. Clin Sci. 2017;131(13):1541–58.
Suki B, Lutchen KR, Ingenito EP. On the progressive nature of emphysema: roles of proteases, inflammation, and mechanical forces. Am J Respir Crit Care Med. 2003;168(5):516–21.
Barnes PJ. Immunology of asthma and chronic obstructive pulmonary disease. Nat Rev Immunol. 2008;8(3):183–92.
Chung KF. The role of airway smooth muscle in the pathogenesis of airway wall remodeling in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005;2(4):347–54.
Hutchinson AT, Vlahos R, Bozinovski S. Role of alveolar macrophages in chronic obstructive pulmonary disease. Front Immunol. 2014;5:435.
Brusselle GG, Joos GF, Bracke KR. New insights into the immunology of chronic obstructive pulmonary disease. Lancet. 2011;378(9795):1015–26.
Kudo M, Ishigatsubo Y, Aoki I. Pathology of asthma. Front Microbiol. 2013;4:263.
Chung KF. Targeting the interleukin pathway in the treatment of asthma. Lancet. 2015;386(9998):1086–96.
Wang Y, Bai C, Li K, Adler KB, Wang X. Role of airway epithelial cells in development of asthma and allergic rhinitis. Respir Med. 2008;102(7):949–55.
Holgate ST. Innate and adaptive immune responses in asthma. Nat Med. 2012;18(5):673–83.
Kubo T, Morita H, Sugita K, Akdis CA. Introduction to mechanisms of allergic diseases. Middleton’s allergy essentials. Amsterdam: Elsevier; 2017. pp. 1–27.
Murdoch JR, Lloyd CM. Chronic inflammation and asthma. Mutat Res Fundam Mol Mech Mutagen. 2010;690(1):24–39.
Carr TF, Berdnikovs S, Simon H-U, Bochner BS, Rosenwasser LJ. Eosinophilic bioactivities in severe asthma. World Allergy Organ J. 2016;9(1):21.
Barnig C, Frossard N, Levy BD. Towards targeting resolution pathways of airway inflammation in asthma. Pharmacol Ther. 2018;186:98–113
Barnig C, Levy BD. Innate immunity is a key factor for the resolution of inflammation in asthma. Eur Respir Rev. 2015;24(135):141–53.
Martín-Orozco E, Norte-Muñoz M, Martínez-García J. Regulatory T cells in allergy and asthma. Front Pediatr. 2017;5.
Ross R. Platelet-derived growth factor. Lancet. 1989;333(8648):1179–82.
Heldin C-H. Structural and functional studies on platelet-derived growth factor. EMBO J. 1992;11(12):4251.
Dolgachev VA, Ullenbruch MR, Lukacs NW, Phan SH. Role of stem cell factor and bone marrow-derived fibroblasts in airway remodeling. Am J Pathol. 2009;174(2):390–400.
Lee CG, Link H, Baluk P, Homer RJ, Chapoval S, Bhandari V, et al. Vascular endothelial growth factor (VEGF) induces remodeling and enhances TH2-mediated sensitization and inflammation in the lung. Nat Med. 2004;10(10):1095–103.
Bhandari V, Choo-Wing R, Chapoval SP, Lee CG, Tang C, Kim Y, et al. Essential role of nitric oxide in VEGF-induced, asthma-like angiogenic, inflammatory, mucus, and physiologic responses in the lung. Proc Natl Acad Sci. 2006;103(29):11021–6.
McMillan SJ, Kearley J, Campbell JD, Zhu X-W, Larbi KY, Shipley JM, et al. Matrix metalloproteinase-9 deficiency results in enhanced allergen-induced airway inflammation. J Immunol. 2004;172(4):2586–94.
Lee CG, Homer RJ, Zhu Z, Lanone S, Wang X, Koteliansky V, et al. Interleukin-13 induces tissue fibrosis by selectively stimulating and activating transforming growth factor β1. J Exp Med. 2001;194(6):809–22.
Cutting GR. Cystic fibrosis genetics: from molecular understanding to clinical application. Nat Rev Genet. 2015;16(1):45.
Cutting GR, Engelhardt J, Zeitlin PL. Genetics and pathophysiology of cystic fibrosis. Kendig’s disorders of the respiratory tract in children (9th Edition). Amsterdam: Elsevier; 2019. pp. 757–68.e6.
Collawn JF, Matalon S. CFTR and lung homeostasis. Am J Physiol Lung Cell Mol Physiol. 2014;307(12):L917-L23.
Muir A, Soong G, Sokol S, Reddy B, Gomez MI, van Heeckeren A, et al. Toll-like receptors in normal and cystic fibrosis airway epithelial cells. Am J Respir Cell Mol Biol. 2004;30(6):777–83.
Chirico V, Lacquaniti A, Leonardi S, Grasso L, Rotolo N, Romano C, et al. Acute pulmonary exacerbation and lung function decline in patients with cystic fibrosis: high-mobility group box 1 (HMGB1) between inflammation and infection. Clin Microbiol Infect. 2015;21(4):368.e1–e9.
Cohen TS, Prince A. Cystic fibrosis: a mucosal immunodeficiency syndrome. Nat Med. 2012;18(4):509–19.
McCuaig S, Martin JG. How the airway smooth muscle in cystic fibrosis reacts in proinflammatory conditions: implications for airway hyper-responsiveness and asthma in cystic fibrosis. Lancet Respir Med. 2013;1(2):137–47.
Dekkers JF, van der Ent CK, Kalkhoven E, Beekman JM. PPARγ as a therapeutic target in cystic fibrosis. Trends Mol Med. 2012;18(5):283–91.
Bals R, Weiner DJ, Wilson JM. The innate immune system in cystic fibrosis lung disease. J Clin Investig. 1999;103(3):303–7.
Tang AC, Turvey SE, Alves MP, Regamey N, Tümmler B, Hartl D. Current concepts: host–pathogen interactions in cystic fibrosis airways disease. Eur Respir Rev. 2014;23(133):320–32.
Hilliard TN, Regamey N, Shute JK, Nicholson AG, Alton EW, Bush A, et al. Airway remodelling in children with cystic fibrosis. Thorax. 2007;62(12):1074–80.
Murphy G, Docherty AJ. The matrix metalloproteinases and their inhibitors. Am J Respir Cell Mol Biol. 1992;7:120-.
Ratjen F, Hartog C, Paul K, Wermelt J, Braun J. Matrix metalloproteases in BAL fluid of patients with cystic fibrosis and their modulation by treatment with dornase alpha. Thorax. 2002;57(11):930–4.
Courtney J, Ennis M, Elborn J. Cytokines and inflammatory mediators in cystic fibrosis. J Cyst Fibros. 2004;3(4):223–31.
Hardie WD, Bejarano PA, Miller MA, Yankaskas JR, Ritter JH, Whitsett JA, et al. Immunolocalization of transforming growth factor α and epidermal growth factor receptor in lungs of patients with cystic fibrosis. Pediatr Dev Pathol. 1999;2(5):415–23.
Booth BW, Adler KB, Bonner JC, Tournier F, Martin LD. Interleukin-13 induces proliferation of human airway epithelial cells in vitro via a mechanism mediated by transforming growth factor-α. Am J Respir Cell Mol Biol. 2001;25(6):739–43.
Spannhake EW. Interactions of pollutants with the epithelium. In: The pulmonary epithelium in health and disease. John Wiley & Sons; 2008. pp 275–99.
López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The hallmarks of aging. Cell. 2013;153(6):1194–217.
Naylor R, Baker D, Van Deursen J. Senescent cells: a novel therapeutic target for aging and age-related diseases. Clin Pharmacol Ther. 2013;93(1):105–16.
Hosgood HD, Menashe I, He X, Chanock S, Lan Q. PTEN identified as important risk factor of chronic obstructive pulmonary disease. Respir Med. 2009;103(12):1866–70.
Mercado N, Ito K, Barnes PJ. Accelerated ageing of the lung in COPD: new concepts. Thorax. 2015. https://doi.org/10.1136/thoraxjnl-2014-206084.
Holzenberger M, Dupont J, Ducos B, Leneuve P, Géloën A, Even PC, et al. IGF-1 receptor regulates lifespan and resistance to oxidative stress in mice. Nature. 2003;421(6919):182–7.
Kapahi P, Zid BM, Harper T, Koslover D, Sapin V, Benzer S. Regulation of lifespan in Drosophila by modulation of genes in the TOR signaling pathway. Curr Biol. 2004;14(10):885–90.
Johnson SC, Rabinovitch PS, Kaeberlein M. mTOR is a key modulator of ageing and age-related disease. Nature. 2013;493(7432):338–45.
Ito K, Colley T, Mercado N. Geroprotectors as a novel therapeutic strategy for COPD, an accelerating aging disease. Int J Chron Obstruct Pulmon Dis. 2012;7(4):641–52.
Hahn DR, Na C-L, Weaver TE. Reserve autophagic capacity in alveolar epithelia provides a replicative niche for influenza A virus. Am J Respir Cell Mol Biol. 2014;51(3):400–12.
Ito K, Barnes PJ. COPD as a disease of accelerated lung aging. CHEST J. 2009;135(1):173–80.
Aoshiba K, Zhou F, Tsuji T, Nagai A. DNA damage as a molecular link in the pathogenesis of COPD in smokers. Eur Respir J. 2012;39(6):1368–76.
Brightling CE, Monteiro W, Ward R, Parker D, Morgan MD, Wardlaw AJ, et al. Sputum eosinophilia and short-term response to prednisolone in chronic obstructive pulmonary disease: a randomised controlled trial. Lancet. 2000;356(9240):1480–5. https://doi.org/10.1016/S0140-6736(00)02872-5.
Athanazio R. Airway disease: similarities and differences between asthma, COPD and bronchiectasis. Clinics (Sao Paulo). 2012;67(11):1335–43.
Sutherland ER, Martin RJ. Airway inflammation in chronic obstructive pulmonary disease: comparisons with asthma. J Allergy Clin Immunol. 2003;112(5):819–27. https://doi.org/10.1016/S0091 (quiz 28).
Cantin AM, Hartl D, Konstan MW, Chmiel JF. Inflammation in cystic fibrosis lung disease: pathogenesis and therapy. J Cyst Fibros. 2015;14(4):419–30. https://doi.org/10.1016/j.jcf.2015.03.003.
Stankiewicz W, Dabrowski MP, Chcialowski A, Plusa T. Cellular and cytokine immunoregulation in patients with chronic obstructive pulmonary disease and bronchial asthma. Mediators Inflamm. 2002;11(5):307–12. https://doi.org/10.1080/09629350210000015719.
Burrows B, Knudson RJ, Cline MG, Lebowitz MD. Quantitative relationships between cigarette smoking and ventilatory function. Am Rev Respir Dis. 1977;115(2):195–205. https://doi.org/10.1164/arrd.1977.115.2.195.
Haldar P, Pavord ID, Shaw DE, Berry MA, Thomas M, Brightling CE, et al. Cluster analysis and clinical asthma phenotypes. Am J Respir Crit Care Med. 2008;178(3):218–24. https://doi.org/10.1164/rccm.200711-1754OC.
Voit EO. A systems-theoretical framework for health and disease: inflammation and preconditioning from an abstract modeling point of view. Math Biosci. 2009;217(1):11–8. https://doi.org/10.1016/j.mbs.2008.09.005.
Franceschi C, Campisi J. Chronic inflammation (inflammaging) and its potential contribution to age-associated diseases. J Gerontol A Biol Sci Med Sci. 2014;69(Suppl 1):4–9. https://doi.org/10.1093/gerona/glu057.
Medzhitov R. Inflammation. new adventures of an old flame. Cell. 2010;140(6):771–6. https://doi.org/10.1016/j.cell.2010.03.006.
Goldstein B, Faeder JR, Hlavacek WS. Mathematical and computational models of immune-receptor signalling. Nat Rev Immunol. 2004;4(6):445–56. https://doi.org/10.1038/nri1374.
Li NY, Verdolini K, Clermont G, Mi Q, Rubinstein EN, Hebda PA, et al. A patient-specific in silico model of inflammation and healing tested in acute vocal fold injury. PLoS One. 2008;3(7):e2789. https://doi.org/10.1371/journal.pone.0002789.
Brauer F, Kris C. Dynamical systems for biological modeling: an introduction. Boca Raton: CRC Press; 2015.
Pigozzo AB, Macedo GC, Santos RW, Lobosco M. On the computational modeling of the innate immune system. BMC Bioinform. 2013;14(Suppl 6):7. https://doi.org/10.1186/1471-2105-14-S6-S7.
Lee J, Adler FR, Kim PS. A mathematical model for the macrophage response to respiratory viral infection in normal and asthmatic conditions. Bull Math Biol. 2017. https://doi.org/10.1007/s11538-017-0315-0.
Chernyavsky IL, Croisier H, Chapman LA, Kimpton LS, Hiorns JE, Brook BS, et al. The role of inflammation resolution speed in airway smooth muscle mass accumulation in asthma: insight from a theoretical model. PLoS One. 2014;9(3):e90162. https://doi.org/10.1371/journal.pone.0090162.
James AL, Elliot JG, Jones RL, Carroll ML, Mauad T, Bai TR, et al. Airway smooth muscle hypertrophy and hyperplasia in asthma. Am J Respir Crit Care Med. 2012;185(10):1058–64. https://doi.org/10.1164/rccm.201110-1849OC.
Brook BS, Peel SE, Hall IP, Politi AZ, Sneyd J, Bai Y, et al. A biomechanical model of agonist-initiated contraction in the asthmatic airway. Respir Physiol Neurobiol. 2010;170(1):44–58. https://doi.org/10.1016/j.resp.2009.11.006.
Moulton DE, Goriely A. Possible role of differential growth in airway wall remodeling in asthma. J Appl Physiol (1985). 2011;110(4):1003–12. https://doi.org/10.1152/japplphysiol.00991.2010.
Schlender A, Alperin PE, Grossman HL, Sutherland ER. Modeling the impact of increased adherence to asthma therapy. PLoS One. 2012;7(12):e51139. https://doi.org/10.1371/journal.pone.0051139.
Smith AM, Adler FR, Ribeiro RM, Gutenkunst RN, McAuley JL, McCullers JA, et al. Kinetics of coinfection with influenza A virus and Streptococcus pneumoniae. PLoS Pathog. 2013;9(3):e1003238. https://doi.org/10.1371/journal.ppat.1003238.
Smith AM, McCullers JA, Adler FR. Mathematical model of a three-stage innate immune response to a pneumococcal lung infection. J Theor Biol. 2011;276(1):106–16. https://doi.org/10.1016/j.jtbi.2011.01.052.
Markovetz MR, Corcoran TE, Locke LW, Myerburg MM, Pilewski JM, Parker RS. A physiologically-motivated compartment-based model of the effect of inhaled hypertonic saline on mucociliary clearance and liquid transport in cystic fibrosis. PLoS One. 2014;9(11):e111972. https://doi.org/10.1371/journal.pone.0111972.
Brown BN, Price IM, Toapanta FR, DeAlmeida DR, Wiley CA, Ross TM, et al. An agent-based model of inflammation and fibrosis following particulate exposure in the lung. Math Biosci. 2011;231(2):186–96.
Donovan GM. Multiscale mathematical models of airway constriction and disease. Pulm Pharmacol Ther. 2011;24(5):533–9. https://doi.org/10.1016/j.pupt.2011.01.003.
Politi AZ, Donovan GM, Tawhai MH, Sanderson MJ, Lauzon AM, Bates JH, et al. A multiscale, spatially distributed model of asthmatic airway hyper-responsiveness. J Theor Biol. 2010;266(4):614–24. https://doi.org/10.1016/j.jtbi.2010.07.032.
Venegas JG, Winkler T, Musch G, Vidal Melo MF, Layfield D, Tgavalekos N, et al. Self-organized patchiness in asthma as a prelude to catastrophic shifts. Nature. 2005;434(7034):777–82. https://doi.org/10.1038/nature03490.
Amin SD, Majumdar A, Frey U, Suki B. Modeling the dynamics of airway constriction: effects of agonist transport and binding. J Appl Physiol (1985). 2010;109(2):553–63. https://doi.org/10.1152/japplphysiol.01111.2009.
Cilfone NA, Perry CR, Kirschner DE, Linderman JJ. Multi-scale modeling predicts a balance of tumor necrosis factor-α and interleukin-10 controls the granuloma environment during Mycobacterium tuberculosis infection. PLoS One. 2013;8(7):e68680. https://doi.org/10.1371/journal.pone.0068680.
Fallahi-Sichani M, El-Kebir M, Marino S, Kirschner DE, Linderman JJ. Multiscale computational modeling reveals a critical role for TNF-α receptor 1 dynamics in tuberculosis granuloma formation. J Immunol. 2011;186(6):3472–83. https://doi.org/10.4049/jimmunol.1003299.
Ceresa M, Olivares AL, Fernandez Suelves S, Noailly J, Gonzalez Ballester MA. Multi-scale immunological and biomechanical model of emphysema progression. Conf Proc IEEE Eng Med Biol Soc. 2017;2017:2712–5. https://doi.org/10.1109/EMBC.2017.8037417.
Ceresa M, Olivares AL, Noailly J, González Ballester MA. Coupled immunological and biomechanical model of emphysema progression. Front Physiol. 2018;9:388. https://doi.org/10.3389/fphys.2018.00388.
Cilfone NA, Kirschner DE, Linderman JJ. Strategies for efficient numerical implementation of hybrid multi-scale agent-based models to describe biological systems. Cell Mol Bioeng. 2015;8(1):119–36. https://doi.org/10.1007/s12195-014-0363-6.
Marino S, Kirschner DE. A multi-compartment hybrid computational model predicts key roles for dendritic cells in tuberculosis infection. Computation (Basel). 2016. https://doi.org/10.3390/computation4040039.
Warsinske HC, Wheaton AK, Kim KK, Linderman JJ, Moore BB, Kirschner DE. Computational modeling predicts simultaneous targeting of fibroblasts and epithelial cells is necessary for treatment of pulmonary fibrosis. Front Pharmacol. 2016;7:183. https://doi.org/10.3389/fphar.2016.00183.
Bouchnita A, Bocharov G, Meyerhans A, Volpert V. Hybrid approach to model the spatial regulation of T cell responses. BMC Immunol. 2017;18(Suppl 1):29. https://doi.org/10.1186/s12865-017-0205-0.
Cevenini E, Caruso C, Candore G, Capri M, Nuzzo D, Duro G, et al. Age-related inflammation: the contribution of different organs, tissues and systems. How to face it for therapeutic approaches. Curr Pharm Des. 2010;16(6):609–18.
Weinberg EJ, Schoen FJ, Mofrad MR. A computational model of aging and calcification in the aortic heart valve. PLoS One. 2009;4(6):e5960. https://doi.org/10.1371/journal.pone.0005960.
Mc Auley MT, Mooney KM. Computationally modeling lipid metabolism and aging: a mini-review. Comput Struct Biotechnol J. 2015;13:38–46. https://doi.org/10.1016/j.csbj.2014.11.006.
Mooney KM, Morgan AE, Mc Auley MT. Aging and computational systems biology. Wiley Interdiscip Rev Syst Biol Med. 2016;8(2):123–39. https://doi.org/10.1002/wsbm.1328.
Mc Auley MT, Mooney KM. Computational systems biology for aging research. Interdiscip Top Gerontol. 2015;40:35–48. https://doi.org/10.1159/000364928.
Witten TM. Modeling cellular aging: an introduction—mathematical and computational approaches. In: Rattan SIS, Hayflick L, editors. Cellular ageing and replicative senescence. vol 4. New York: Springer International Publishing; 2016. pp. 117–41.
Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008;454(7203):428–35. https://doi.org/10.1038/nature07201.
Weber GF, Chousterman BG, He S, Fenn AM, Nairz M, Anzai A, et al. Interleukin-3 amplifies acute inflammation and is a potential therapeutic target in sepsis. Science. 2015;347(6227):1260–5. https://doi.org/10.1126/science.aaa4268.
Serhan CN, Chiang N, Dalli J. The resolution code of acute inflammation: novel pro-resolving lipid mediators in resolution. Semin Immunol. 2015;27(3):200–15. https://doi.org/10.1016/j.smim.2015.03.004.
Chiang N, Dalli J, Colas RA, Serhan CN. Identification of resolvin D2 receptor mediating resolution of infections and organ protection. J Exp Med. 2015;212(8):1203–17. https://doi.org/10.1084/jem.20150225.
Medzhitov R, Shevach EM, Trinchieri G, Mellor AL, Munn DH, Gordon S, et al. Highlights of 10 years of immunology in nature reviews immunology. Nat Rev Immunol. 2011;11(10):693–702. https://doi.org/10.1038/nri3063.
Reyes M, Quintanilla C, Burrows R, Blanco E, Cifuentes M, Gahagan S. Obesity is associated with acute inflammation in a sample of adolescents. Pediatr Diabetes. 2015;16(2):109–16. https://doi.org/10.1111/pedi.12129.
Wang X, Zhu M, Hjorth E, Cortés-Toro V, Eyjolfsdottir H, Graff C, et al. Resolution of inflammation is altered in Alzheimer’s disease. Alzheimers Dement. 2015;11(1):40–50. https://doi.org/10.1016/j.jalz.2013.12.024.
Kotas ME, Medzhitov R. Homeostasis, inflammation, and disease susceptibility. Cell. 2015;160(5):816–27. https://doi.org/10.1016/j.cell.2015.02.010.
Acknowledgements
The authors thank NSF for supporting this work through a Grant CMMI-1430379.
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible Editor: Andrew Roberts.
Rights and permissions
About this article

Cite this article
Aghasafari, P., George, U. & Pidaparti, R. A review of inflammatory mechanism in airway diseases. Inflamm. Res. 68, 59–74 (2019). https://doi.org/10.1007/s00011-018-1191-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-018-1191-2