
Abstract
This study explores the influence of electronic clinical pathways (ECPs) on nurses’ daily activities, especially nursing communication, in a university hospital. Although an electronic clinical pathway enables medical-treatment processes to be standardized by interacting with different occupations, few studies have been conducted from the managerial perspective. We interviewed a doctor in the Department of Medical Information Systems and eight nurses who make entries and use ECPs. The results of the interview indicated that some nurses learned about the medical processes using electronic clinical pathways. The results also showed that the assessment abilities for patient care could decline, if the nurses failed to incorporate the electronic clinical pathways into their daily routines.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Nurses must work to improve their knowledge and skills to keep up with the rapid advance of medicine. Hospitals, especially university hospitals, now face the difficult situation of understanding the medical-treatment workflow. This can cause a communication problem among the nurses. It is important to manage this problem by efficiently tracking the medical records and providing an atmosphere that encourages communication.
Clinical pathways (CPs) were expected to solve the problem of tracking records. CPs are management plans for medical treatments that display goals for patients, and provide the order and timing of the treatment needed to efficiently achieve these goals [1]. CPs apply the critical-path concept, a project-management scheduling method, to medicine. This approach is intended to improve the quality of the medical-staff activity through processes that delineate standardized medical treatments. CPs were originally conceived to resolve financial issues in hospitals [2]; however, they were gradually adapted to facilitate managerial activities.
After they were brought to Japan, CPs were extended past the idea of standardization. If a medical treatment was carried out by various medical staff, standardized processes strengthened the team care by clarifying the respective roles. Risk management was also introduced by standardizing the medical treatments. Medical processes in CPs are fully described when the treatments are conducted. Finally, CPs are used for informed consent by describing the flow for the patient from the beginning to the end [3]. However, studies of the organizational changes that occur after deploying CPs have hardly been conducted.
The purpose of this study is to discuss the influences of electronic clinical pathways (ECPs) on a university hospital. We particularly focused on the issues of nursing communication related to ECPs. We formulated two research questions to clarify the topics covered this study.
-
RQ1: What kind of benefit/risk factors are shown in the university hospital?
-
RQ2: How are the factors related to each other?
2 Related Work
2.1 Clinical Pathway Studies
CPs define the optimal sequence and timing of interventions by medical staff, e.g., diagnoses or procedures by doctors or nurses [1]. Conventional studies revealed that CPs have various functions to improve daily activities. A CP improves the delivery of evidence-based care [4, 5, 8], shortens the patient’s length of stay [2, 4], reduces the nursing records [5, 8], and improves the patient’s education [4]. CPs also facilitate staff-to-staff and staff-to-patient communications [5, 6]. By analyzing the variances in the CPs, nurses learn to differentiate between typical cases and exceptional cases. CPs have the potential to be both a knowledge-management tool and an education tool for medical staff [7, 9, 16].
2.2 Electronic Clinical Pathway Studies
Paper-based clinical pathways have been integrated into electronic medical records in recent years as ECPs. A few studies on ECP interfaces [10] or implementations [11–13] have been conducted. Balatsoukas and colleagues proposed user-friendly and usable function requirements for ECP implementations [10]. Wakamiya and Yamauchi identified seventeen requirements for ECP implementations based on interviews [11].
ECPs have become useful tools in conveying medical-treatment information to the patient, and sharing patient information in shift reports [14, 15]. However, there are fewer studies about the effects of ECPs and incorporating ECP management into daily activities. Hence, our study group has investigated the effects of ECPs from the standpoint of organizational knowledge management [17]. Sugihara clarified that nurses who have experience composing ECP reports tend to acquire managerial knowledge, especially when training apprentices [17].
This paper enlarges the range of informants from composers to users, and discusses the effects of the ECPs on daily activities. This study focuses on nursing-communication issues because about 70 % of medical incidents are caused by communication failures [18]. Similarly, in Japan, mis-tracked medical records or mis-shared information were the causes of approximately 20 % of medical incidents. Out of 40,156 incidents, 910 were from mis-tracked medical records and 6,508 were from mis-shared information, with 595 overlapping incidents [19].
3 Methods
3.1 Case Outline
We chose Miyazaki University Hospital (MUH) as the field for this study because almost all departments in this hospital have adopted ECPs that combine clinical pathways and electronic medical records; others have merely attempted to use ECPs as prototypes. The input/output devices are stationary computers, personal digital assistants, and smartphones. Nurses usually input vital data, e.g., blood pressure readings, using bedside PDAs, and write long entries, e.g., observation comments, on the computer at the staff station.
MUH is the largest hospital in the Miyazaki prefecture. In a seven-story building with 632 beds, it had 18 departments in 2015. MUH introduced paper-based CPs from 2004 to 2007; they have since converted to ECPs. Almost all of the departments in this hospital employ ECPs.
3.2 Study Design
We employed a case study as an exploratory style. This study consisted of two steps: a semi-structured interview and a modified grounded-theory approach (M-GTA). First, a 30-min semi-structured interview was conducted at MUH; the informants were a doctor and eight nurses. Second, after the interview data was fully transcribed, it was analyzed using the M-GTA. M-GTA, developed in Japan, is an analysis technique for qualitative data [20, 21].
The transcripts were read as many times as possible to identify any commonalities and differences among the data; similar data were classified into the same categories. During this process, when a category was recognized as similar to another one, they were combined into one category. This analysis process was repeated until no new categories could be formed; i.e., until theoretical saturation was reached. The relationship among the categories was depicted by considering the cause-effect characteristics of the comments.
4 Results
4.1 Integrated Categories
Twenty-six concepts were generated by the analysis. These concepts were divided into seven categories.
The first category is reducing the time and effort of keeping medical records. Nurses do not need to rewrite the nursing-care plans for an ECP-adopted patient because the nursing records on the patient’s condition already appear in the ECP. Before ECPs were introduced, a nurse had to contact the doctor to find out why a blank record appeared in the medical records.
The second is that the medical process can be learned while composing ECP records. Various medical staff (doctors, nurses, dietitians, etc.) participate in making ECPs. Nurses who make ECPs can learn about the various medical cases through information and knowledge sharing with staff in different roles.
The third is expected spillover effects associated with ECP use. The spillover effect is related to on-the-job training. When a patient begins to receive a medical treatment, senior nurses use ECPs as an orientation tool for apprentices.
The fourth is signs of deterioration caused by ECP use. By reducing the recording time and effort, nurses may lose opportunities to increase their knowledge and skills.
The fifth category is knowledge-acquisition channels for nursing. Nurses acquire knowledge through receiving on-the-job training, reading and writing nursing texts, questioning doctors or senior nurses, and participating in seminars. The process of composing ECP reports provides an opportunity to communicate with doctors and senior nurses.
The sixth involves management policies in the Department of Nursing. The MUH Department of Nursing has introduced various policies to improve the quality of nursing and care; they especially encourage apprentice training. Although these policies have mainly focused on daily nursing activities, some of them have indirectly functioned as practice using the ECPs. For instance, mentoring the apprentices worked as a double-check when inputting ECP records. Moreover, senior nurses were able to convey their knowledge of ECP use, in addition to their nursing methods.
The seventh is an ideal model of the nurse. Some nurses and apprentices have an ideal model of a nurse. The model must possess extensive medical knowledge and skills, be trusted by patients, and be self-disciplined.
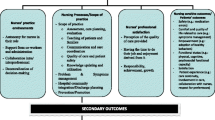
4.2 Relationships Among Categories
This section explains the relationships among the categories. Four relationship lines are shown in Fig. 1: (a) a solid arrow, (b) a dotted arrow, (c) a dotted line with round start and end points, and (d) a solid line with round start and end points.

Electronic clinical pathway interface for medical staff
A solid arrow represents temporal cause and effect. For example, since ECPs were first deployed, their role has changed from a cost-cutting tool to a tool for learning the medical workflow, as shown in Reducing time and medical records to Learning the medical process through making ECP records.
A dotted arrow represents the possibility of spillover effects. For example, nurses suggested that spare time produced by reducing the time for tracking medical records could lead to enriched patient care, as indicated in Reducing time and medical records to Expected spillover effects associated with ECPs.
A dotted line with round start and end points represents a possible influence of one category on another. ECPs provoked a negative influence when some nurses merely used them to reduce the time for writing medical records. Nurses could lose opportunities to increase their knowledge and skills. MUH has had no incidents, owing to the management of the nursing department; i.e., Signs of deterioration caused by ECP use to Management policies in Department of Nursing (Fig. 2).

Relationships among generated categories
A solid line with round start and end points represents an influence of one category on another. Nurses who have an ideal nurse model want to approach it, so they study hard using the available knowledge-acquisition channels; i.e., Channels of knowledge acquisition for nursing to An ideal model of the nurse.
5 Discussion
The results of this study indicated that introducing ECPs reduces the time and mitigates the burden of writing medical records. These results are equivalent to conventional studies [18]. Before ECP deployment, it was essential for nurses to contact doctors to know the reason for blank doctor’s orders. Basic procedures and medicines are already recorded in the ECPs so the nurses do not need to call the doctor. This effect could signify a reduction in unnecessary communication and fewer overlooked records. One study suggested that the SBAR system (Situation Background Assessment Recommendation) potentially decreases communication failures, which are the leading cause of inadvertent patient harm [19]. From the viewpoint of decreasing unnecessary confirmations, we considered that ECPs are preventing miscommunications.
On the other hand, this benefit has a negative aspect in that nurses lose the opportunities to discuss medical treatments in detail with the doctor. Consequently, the nurses gradually lose opportunities to acquire in-depth knowledge, in terms of assessing a patient’s condition through deep communication. This leads to the risk of deterioration for apprentices due to a lack of communication among the staff. Our previous investigation clarified that nurses who made ECP records acquired medical knowledge and learned how to embed ECPs into the workflow by themselves [17]. If an apprentice is faced with a deeply rooted symptom, he/she may overlook the true cause from the outcome on the ECP; an unexpected outcome is difficult to identify in comparison with symptoms of common diseases. Decreasing doctor-nurse communication is equivalent to reducing the opportunities to share knowledge with each other.
However, incidents caused by losing the assessment ability were not observed at the hospital. We consider two probable reasons. The time after deployment is not sufficient to erode the nursing abilities. Another reason is that the chief nurses manage to work around the problem. Therefore, it is essential to conduct a follow-up investigation to uncover the reason.
6 Conclusion
In this paper, we presented a field study from a university hospital, focusing on nursing communication; the subjects make and use ECPs in daily nursing. The results of our study showed that ECPs have both benefit and risk factors. The answers to the research questions are as follows:
-
RQ1. The benefit factors of ECPs are improved on-the-job training for apprentices, and a mitigated burden of keeping medical records, whereas they risk miscommunications among the medical staff.
-
RQ2. Ten connections were classified into four major influences; temporal cause and effect, possibility of spillover effects, possibility of influencing each other, and influencing each other. The main results were that a factor related to composing ECP records connects to opportunities for efficiently learning about medical processes. Afterwards, the connections crystallized to channels of knowledge acquisition among the medical staff, especially for the nurses.
Managers and/or engineers in the medical field could consider two possible applications for these results. Medical managers might investigate methods of measuring ECPs’ risk factors. Engineers could implement a function to enhance the benefits (e.g., effectively learning the medical processes beyond the boundaries among the medical staff) and reduce the risks (e.g., by promoting communication). However, this study employed interviews to a few nurses and a doctor, as a qualitative approach. We need to follow up with quantitative research, such as questionnaires, to determine the overall trends.
References
Every, N.R., Kopecky, S.: Critical pathways: A review. Circulation 101(4), 461–465 (2000)
Zehr, K.J., Dawdon, P.B., Yang, S.C., Heitmiller, R.F.: Standardized clinical care pathways for major thoracic cases reduce hospital costs. Ann. Thorac. Surg. 66(3), 914–919 (1998)
Soejima, H.: Iryō Kiroku Ga Kawaru Ketteiban Kurinikaru Pasu (in Japanese). Tōkyō: Igaku Shoin (2004). Print
Renholm, M., Leino-Kilpi, H., Suominen, T.: Critical pathways: A systematic review. J. Nurs. Adm. 32(4), 196–202 (2002)
Campbell, H., Hotchkiss, R., Baradshaw, N., Porteous, M.: Integrated care pathways. BMJ Br. Med. J. 316(7125), 133 (1998)
Vanhaecht, K., Bollmann, M., Bower, K., Gallagher, C., Gardini, A., Guezo, J., Van Zelm, R.: Prevalence and use of clinical pathways in 23 countries—An international survey by the European Pathway Association. J. Integr. Pathways 10(1), 28–34 (2006)
Cabitza, F., Simone, C., Sarini, M.: Knowledge artifacts as bridges between theory and practice: The clinical pathway case. In: Ackerman, M., Dieng-Kuntz, R., Simone, C., Wulf, V. (eds.) Knowledge Management in Action. IFIP, vol. 270, pp. 37–50. Springer, Heidelberg (2008)
de Luc, K.: Care pathways: An evaluation of their effectiveness. J. Adv. Nurs. 32(2), 485–496 (2000)
Coffey, R.J., Richards, J.S., Remmert, C.S., LeRoy, S.S., Schoville, R.R., Baldwin, P.J.: An introduction to critical paths. Qual. Manage. Healthc. 14(1), 46–55 (2005)
Balatsoukas, P., Williams, R., Davies, C., Ainsworth, J., Buchan, I.: User interface requirements for web-based integrated care pathways: evidence from the evaluation of an online care pathway investigation tool. J. Med. Syst. 39(11), 1–15 (2015)
Wakamiya, S., Yamauchi, K.: What are the standard functions of electronic clinical pathways? Int. J. Med. Inform. 78(8), 543–550 (2009)
de Luc, K., Todd, J.: E-pathways: Computers and the Patient’s Journey Through Care. Radcliffe Publishing, Abingdon (2003)
Gooch, P., Roudsari, A.: Computerization of workflows, guidelines, and care pathways: A review of implementation challenges for process-oriented health information systems. J. Am. Med. Inform. Assoc. 18(6), 738 (2011)
Patel, V.L., Kushniruk, A.W., Yang, S., Yale, J.F.: Impact of a computer-based patient record system on data collection, knowledge organization, and reasoning. J. Am. Med. Inform. Assoc. 7(6), 569–585 (2000)
Hyde, E., Murphy, B.: Computerized clinical pathways (care plans): Piloting a strategy to enhance quality patient care. Clin. Nurse Spec. 26(5), 277–282 (2012)
Yang, H., Li, W., Liu, K., Zhang, J.: Knowledge-based clinical pathway for medical quality improvement. Inf. Syst. Front. 14(1), 105–117 (2012)
Sugihara, T., Sakanishi, H., Gofuku, A., Umemoto, K., Suzuki, M., Araki, K.: Potential of electronic clinical pathways as triggers for eliciting implicit knowledge. In: Proceedings of the 41st Annual Conference of the IEEE Industrial Electronics Society (IECON2015), pp. 410–415 (2015)
Leonard, M., Graham, S., Bonacum, D.: The human factor: The critical importance of effective teamwork and communication in providing safe care. Qual. Saf. Health Care. 13(suppl 1), i85–i90 (2004)
Japan Council for Quality Health Care.: “iryou ziko joho syu-syu- tou zigyou hiyarihatto 2009–2015”, 7 June 2016. http://www.med-safe.jp/mpsearch/SearchReport.action
Kinoshita, Y.: Raibu Kōgi M-GTA: Jissenteki Shitsuteki Kenkyūhō: Shūseiban Guraundeddo Seorī Apurōchi No Subete. Tōkyō: Kōbundō (2007). Print
Kinoshita, Y.: Guraundeddo Seorī Apurōchi No Jissen: Shitsuteki Kenkyū Eno Sasoi. Tōkyō: Kōbundō (2003). Print
Acknowledgments
Our research was partly supported by the Grant-in-Aid for Scientific Research (21330089, 24330118, 26502008, 15K16168) of the JSPS. We would like to thank the doctor and nurses of Miyazaki University Hospital for their cooperation.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer International Publishing Switzerland
About this paper
Cite this paper
Kanehira, T., Sugihara, T., Suzuki, M., Gofuku, A., Araki, K. (2016). Exploring Risk-Benefit Factors of Electronic Clinical Pathways Regarding Nursing Communication. In: Duffy, V. (eds) Digital Human Modeling: Applications in Health, Safety, Ergonomics and Risk Management. DHM 2016. Lecture Notes in Computer Science(), vol 9745. Springer, Cham. https://doi.org/10.1007/978-3-319-40247-5_43
Download citation
DOI: https://doi.org/10.1007/978-3-319-40247-5_43
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-40246-8
Online ISBN: 978-3-319-40247-5
eBook Packages: Computer ScienceComputer Science (R0)