
Abstract
Ureteral stents have a major role in urology and are used mainly to achieve correct renal drainage. Ureteral stents are very effective and their use in recent decades has clearly increased. However, more than 80% of patients with an ureteral stent present associated symptoms, such as pain, lower urinary tract symptoms (LUTS), sexual dysfunction… leading to an important drop in the quality of life (QoL). Our objective is to describe ureteral stent related symptoms and their impact on the quality of life of patients.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
The ureteral stent is a tubular device with multiple lateral holes that is placed inside the ureter to prevent or treat an obstruction in order to ensure the permeability of the urinary tract. In 1967, Zimskind et al. [1] described the endoscopic placement of the first permanent ureteral stents. Subsequently, Finney et al. [2] improved the shape of the device by describing the double J stent (DJS).
Its main indications are unblocking the upper urinary tract of both extrinsic and intrinsic causes, allowing healing after a urinary anastomosis or ureteral trauma and as prevention of obstruction after endourological techniques or iatrogenic ureteral injury [3, 4].
With the endourological techniques increase, their routine use has raised. Its placement prior to ureterorenoscopy (URS) is not generally necessary, although some studies report a better stone-free rate and fewer intraoperative complications [5, 6]. Randomized prospective trials have found that routine stenting after uncomplicated URS (complete stone removal) is not necessary; stenting might be associated with higher post-operative morbidity and costs [7,8,9,10].
Although in the first published scientific literature, no side effects associated with its use were described, Pollard and Macfarlane [11] in 1988 presented the first series that describes the morbidity associated with ureteral stents, with a decrease in quality of life in 80% of patients and 90% of urinary symptoms associated with the stent (SRS). Subsequent studies confirmed similar morbidity rates [12, 13], confirming the side effects associated with its use.
The objective of this chapter is to evaluate the impact on the quality of life of patients with ureteral stents.
2 Symptoms Related to Ureteral Stents
The main symptoms related to urinary stents are:
2.1 Lower Urinary Tract
Storage symptoms of the lower urinary tract are the most prevalent ones in patients with ureteral stents and that cause the greatest loss of quality of life. They are related to the bladder mucosa irritation, produced by mechanical scratching of the stent and, it has been related to the spasmodic contractions of the ureter produced by the presence of an inner foreign body. There are also factors related to the type of stent selected:
Ureteral stent length: A published randomized clinical trial [14] confirmed that urgency and dysuria were common with longer stents and negatively affected the patients’ quality of life. Along the same lines, Taguchi et al. [15] and Al-kandari [16] also found greater urgency, dysuria, as well as a worse quality of life in patients with ureteral stents that crossed the bladder midline. The gold standard for measuring the required stent length remains the insertion of a graduated ureteral catheter, measuring the distance between ureteropelvic junction (UPJ) and ureterovesical junction (UVJ) [17]. Lee at al [18] correlated the length of the stent with the height of the patient. On the other hand, Ho et al. [19] proposed a mathematical formula (length = 0.125 × body height + 0.5 cm) to calculate the length of the stent.
Calibre of urinary stents: Another aspect evaluated, is whether the thickness of the ureteral stent can influence the worsening of symptoms and the deterioration of the patient’s quality of life. Candela et al. [20] compared stent diameter and composition with patient symptoms occurring from stent placed for a variety of reasons. They did not find a difference in terms of patient tolerance. Erturk et al. [21] performed a study comparing pain and storage urinary symptoms in patients undergoing stent positioning of different sizes after ureteroscopy. They showed no differences between the studied groups. Similarly Chandhoke et al. [22] in a study conducted with patients having shock wave lithotripsy (SWL) noted no significant differences in terms of pain and irritation using stents of two different diameters. Along the same lines, Damiano et al. [23] found no differences between stents of different diameters, but they did reflect a higher frequency of migration in those with a smaller diameter.
Distal coil shape: As the distal coil of the stent is hypothesized to be in part responsible for SRS, several design alterations have been proposed to reduce SRS. A loop, a tail and a simple suture in several trials have replaced the conventional distal coil [24].
Stent composition: The stent composition can influence symptoms depending on its biocompatibility and the tissue reaction. Currently used biomaterials for stent construction are synthetic polymers or (proprietary) copolymers such as silicone, polyethylene, polyurethane, C-Flex®, Silitek®, Pellethane®, Vertex® and Percuflex™ [24]. The most biocompatible material is silicone, but its high coefficient of friction can make stent insertion difficult [25]. Scarneciu et al. [26] used the Flanagan life scale (QOLS) as a tool for evaluating quality of life with different stent materials (40.98% aliphatic polyurethane, hydrophilic polyurethane coating (20.72%), carbothane (17.82%).), silicon (20.46%). None of the materials proved to be superior in terms of symptomatology.
2.2 Pain
Pain is one of the symptoms that occurs in up to 80% of patients, predominantly in the lower back associated with urination. Intravesical pressure increases with detrusor contraction and this pressure increase can be transmitted by reflux to the renal unit, triggering flank pain [27]. Suprapubic pain can result from local bladder irritation by the distal coil or as a secondary sign of associated complication such as encrustation or infection [14]. Different stents have been designed with anti-reflux mechanisms to reduce the pain associated with reflux; at the distal end of the stent, a valve mechanism allows drainage of the kidney but closes with increasing intravesical pressure [28]. Ritter et al. [29] compared the antireflux stent with a conventional stent, without finding significant differences, probably due to a small sample size (29 patients). However, Ecke et al. [30] reached a significantly lower complication rate and higher acceptance rate with an antirefluxive stent. Although many promising designs have been developed, these have not entered routine clinical practice yet [24] (Fig. 1).

Encrustations on stent
2.3 Urinary Tract Infection
Patients with ureteral stents are prone to urinary tract infection. Therefore, antibiotics should be administered prophylactically before stent placement and removal [31]. The ureteral stent acts as a foreign body and therefore bacteria often colonize them, usually within the first 2 weeks after stent placement.
Colonization rates of the ureteral stent are 100% in patients with permanent stents and 69.3% in patients with temporary stents [32, 33]. However, long-term therapy does not provide benefit in patients with asymptomatic bacteriuria. Additionally, diabetes mellitus, chronic renal failure and pregnancy were associated with a higher risk of stent related bacteriuria [34]. Biofilm formation on the stent surface has been implicated as an important step in the process of stent associated UTI, stent encrustation and SRS. The impact of biofilms on stent morbidity has been discussed controversially [35]. Within this biofilm, microorganisms are protected from host defences and antibiotics, which may lead to an accelerated development of antibiotic resistance.
Coatings have been proven to prevent or reduce biofilm formation to a clinically relevant extent [36]. The associated symptoms of long-lasting DJS and the influence of biofilm formation have also been evaluated. Biofilm formation on ureteral stents does not seem to be the relevant driver of symptoms. Long-term Double-J stenting provides a valuable treatment option, if stent-associated symptoms are low during the initial indwelling period. Thus, symptoms remain stable over the long-term course and the majority of patients are satisfied with the treatment [37].
The indwelling time is the most important risk factor for encrustation [24], that can make it difficult or impossible to remove it. The encrustation and cellular adherence, which, in turn, promotes urinary tract infection, can induce impaired healing in case of ureteral damage [38]. Cadieux et al. [39] show that although triclosan-eluting stents did not show a clinical benefit in terms of urine and stent cultures or overall case symptoms compared with controls, it resulted in decreased antibiotic prescription and significantly fewer symptomatic infections. Urine pH and supersaturation also play a very important role, the incidence of embedded stent could be minimized by acidifying the urine and increasing urinary crystallization inhibitors. Torrecilla et al. [40] describe a significant decrease in encrustation in the group that received treatment with L-methionine and phytate compared to the control group. Removal of embedded ureteral stents requires careful planning to avoid fragmentation.
3 Assessment of the Quality of Life of Patients with Urinary Stents
According to the World Health Organization (WHO), QoL is described as the individual’s perception of their life positions under the perspective of the culture and value system in which they are inserted, including individual goals, expectations, standards and priorities [41]. Different tools have been designed to determine the quality of life in different settings.
The most widely used tool to assess the impact on quality of life in patients with ureteral stents is the Ureteral Stent Symptom Questionnaire (USSQ) specifically designed to obtain a psychometrically valid measure to evaluate symptoms and impact on quality of life of ureteral stents. It was developed and published by Joshi et al. [42] in 2003 as a valid instrument to evaluate the impact and compare different types of stent in six health domains: three specific to the stent (voiding symptoms, pain, additional problems) and three general aspects (general health status, work environment and sexual life) in 38 items.
Another widely used tool has been the International Prostate Symptom Score (IPSS), which is the most widely used questionnaire to quantify the symptoms derived from benign prostatic hyperplasia. It is not a specific to evaluate the impact of the stent. However, it has been widely used for this purpose, especially prior to the publication of the USSQ. It consists of eight questions: three filling symptoms questions, four emptying symptoms questions, and one quality of life question.
Other questionnaires to assess health-related quality of life (HRQoL) in the general population are the SF-36 health questionnaire, EuroQoL 5D, and the Flanagan’s Quality of Life Scale. The SF-36 [43] is made up of 36 items that assesses eight scales: Physical function, physical role, bodily pain, general health, vitality, social function, emotional role, and mental health. As a limitation of the questionnaire, it does not include some important health aspects such as sleep disorders, cognitive function, family function and sexual function. Another frequently used questionnaire, the EuroQoL-5D (EQ-5D) [44] assesses five dimensions of health status: mobility, personal care, daily activities, pain/discomfort and anxiety/depression and includes the visual analog pain scale (VAS).
The use of these tools has made it possible to quantify the impact on quality of life produced by urinary stents.
3.1 Impact on Quality of Life in Patients of Ureteral Stent
Ureteral stent placement has a variable degree of impact across all general health domains. Many patients report fatigue, dependence to perform daily activities, and even reduce their social life while presenting symptoms associated with the stent. The stent can also lead to a worsening in the quality of sleep and the appearance of anxiety [45].
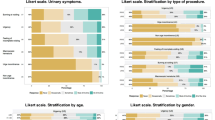
Studies that have used the USSQ questionnaire have shown that patients with ureteral stents present an increase in LUTS with a significantly reduced quality of life on the scales of body pain, perception of general health, mental health, social functioning and physical functioning.
There is some controversy regarding stent tolerance based on the age of the patient. Irani et al. observed that stents are less well tolerated by younger patients [46]. However, Joshi et al. [12] did not observe any correlation between urinary symptoms and the age of the patients [47].
The fall in the sexual sphere has an important impact on the quality of life. The use of DJS can produce various symptoms within the sexual sphere such as pain during sexual intercourse, dyspareunia, ejaculodynia, erectile dysfunction or decreased libido among others. The study by Joshi et al. [12] revealed that 35% of sexually active patients had pain during sexual intercourse. Sexual health, although affected by stents, might have been perceived as a lesser problem. It seems not a major problem with short stent indwelling time (week 1) but it becomes important as the stent endures. The impact of stents was not only related to the pain during sexual activity, but also appeared to be affecting overall sexual satisfaction.
Other studies such as that of Leibovici et al. [48], described that 62.6% of sexually active patients had pain during intercourse (32% men), ejaculodynia (46%), dyspareunia (62%), erectile dysfunction (20%), decreased libido (38% men and 66% women) and fear that intercourse would be harmful to the DJS (54% women). Globally, women presented more problems than men did. A meta-analysis carried out by Lu et al. [49] in which five prospective studies were included, to analyse sexual health after an endourological procedure or stent, showed that in patients without a double-J stent, the change in sexual function after endourological procedures was not significant in men nor women. However, in patients with indwelling double-J stent, sexual function scores significantly declined after the procedure in both men and women. One study reported that sexual deterioration in women recovered 1 month after stent removal [50]. In another study, the IIEF score remained unchanged on the tenth day after stent removal when compared with the preoperative baseline value [51]. These results suggest that sexual function was impaired after employing a stent but recovered soon following stent removal.
On the other hand, Zhu et al. [52] and Giannarini et al. [53] showed impairment in sexual health in patients compared to that in healthy individuals at 4 weeks after stent placement. By contrast, some studies showed no significant difference when comparing sexual health at the fourth week after placement with the fourth week after removal [54]. A slight improvement of symptoms after stent removal may account for these results.
The described symptoms related to the ureteral stent can be the cause of sick leave, depending on the type of work activity, with a significant impact on the productivity of the active population [13].
Joshi et al. [12] found that 26% of patients who wore DJS for 4 weeks spent more than 2 days in bed (range 3–14 days) and 42% had to reduce activities by more than 3 half days or more (4–28 half days). Similarly, the presence of the stent resulted in a reduction in the quality of work.
Along the same lines, Leibovici et al. [48] found that 45% of patients lost some days of work during the first 2 weeks after stent placement. At 30 and 45 days after placement, 30% and 32% respectively also lost days of work due to sick leave. All days off were attributed to DJS-related symptoms. Although there seems to be a progressive tolerance over time with less loss of workdays due to work leave [13].
4 Innovations for the Improvement of Stented Patients Quality of Life
Informing the patient about the symptoms and the impact on quality of life prior to the placement of a stent can help to understand the symptoms and improve their perception, as described by Abt et al. [55]. However, the influence of information on the incidence and extent of symptoms appears limited.
Management should be focused on the prevention and management of symptoms. In this sense, research has focused on new materials and stent designs that would be more compatible to the physiologic properties of the urinary tract and medications that can ameliorate the sensitivity and motor response of the bladder. All research efforts are focused on approaching the ideal conditions that a stent should meet. The ideal stent would provide adequate urinary drainage, resist migration, encrustation and bacterial colonization. It should be easy to insert and remove, minimize stent-related morbidity, and low cost. Resistant to compression, bio-durable and biocompatible.
The stent design aims to improve patient comfort, stent handling and reduce the incidence of urinary tract infections and encrustations. Modern science still offers many alternatives in order to invent the “ideal stent”. Thermo-expandable stents are increasingly being studied, thermo-expandable shape memory stents, stents made of biodegradable or bioabsorbable materials, coated stents with various substances as heparin, various enzymes, hydrogel, antibiotics and antifungal medication or anti-inflammatory medication [26].
References
Zimskind PD, Fetter TR, Wilkerson JL. Clinical use of long-term indwelling silicone rubber ureteral splints inserted cystoscopically. J Urol. 1967;97(5):840–4.
Finney RP. Experience with new double J ureteral catheter stent. J Urol. 1978;120(6):678–81.
Damiano R, Oliva A, Esposito C, De Sio M, Autorino R, D’Armiento M. Early and late complications of double pigtail ureteral stent. Urol Int. 2002;69(2):136–40.
Ringel A, Richter S, Shalev M, Nissenkorn I. Late complications of ureteral stents. Eur Urol. 2000;38(1):41–4.
Jessen JP, Breda A, Brehmer M, Liatsikos EN, Millan Rodriguez F, Osther PJS, et al. International Collaboration in Endourology: multicenter evaluation of prestenting for ureterorenoscopy. J Endourol. 2016;30(3):268–73.
Assimos D, Crisci A, Culkin D, Xue W, Roelofs A, Duvdevani M, et al. Preoperative JJ stent placement in ureteric and renal stone treatment: results from the Clinical Research Office of Endourological Society (CROES) ureteroscopy (URS) Global Study. BJU Int. 2016;117(4):648–54.
Song T, Liao B, Zheng S, Wei Q. Meta-analysis of postoperatively stenting or not in patients underwent ureteroscopic lithotripsy. Urol Res. 2012;40(1):67–77.
Haleblian G, Kijvikai K, de la Rosette J, Preminger G. Ureteral stenting and urinary stone management: a systematic review. J Urol. 2008;179(2):424–30.
Nabi G, Cook J, N’Dow J, McClinton S. Outcomes of stenting after uncomplicated ureteroscopy: systematic review and meta-analysis. BMJ. 2007;334(7593):572.
Moon TD. Ureteral stenting—an obsolete procedure? J Urol. 2002;167(5):1984.
Pollard SG, Macfarlane R. Symptoms arising from double-J ureteral stents. J Urol. 1988;139(1):37–8.
Joshi HB, Stainthorpe A, MacDonagh RP, Keeley FX, Timoney AG, Barry MJ. Indwelling ureteral stents: evaluation of symptoms, quality of life and utility. J Urol. 2003;169(3):1065–9; discussion 1069.
Ordaz-Jurado G, Budía-Alba A, Bahilo-Mateu P, López-Acón JD, Trassierra-Villa M, Boronat-Tormo F. [Impact in the quality of life of the patients with double J catheter]. Arch Esp Urol. 2016;69(8):471–8.
Miyaoka R, Monga M. Ureteral stent discomfort: etiology and management. Indian J Urol. 2009;25(4):455–60.
Taguchi M, Yoshida K, Sugi M, Matsuda T, Kinoshita H. A ureteral stent crossing the bladder midline leads to worse urinary symptoms. Cent Eur J Urol. 2017;70(4):412–7.
Al-Kandari AM, Al-Shaiji TF, Shaaban H, Ibrahim HM, Elshebiny YH, Shokeir AA. Effects of proximal and distal ends of double-J ureteral stent position on postprocedural symptoms and quality of life: a randomized clinical trial. J Endourol. 2007;21(7):698–702.
Barrett K, Ghiculete D, Sowerby RJ, Farcas M, Pace KT, Honey RJD. Intraoperative radiographic determination of ureteral length as a method of determining ideal stent length. J Endourol. 2017;31(S1):S-101.
Lee C, Kuskowski M, Premoli J, Skemp N, Monga M. Randomized evaluation of Ureteral Stents using validated Symptom Questionnaire. J Endourol. 2005;19(8):990–3.
Ho C-H, Chen S-C, Chung S-D, Lee Y-J, Chen J, Yu H-J, et al. Determining the appropriate length of a double-pigtail ureteral stent by both stent configurations and related symptoms. J Endourol. 2008;22(7):1427–31.
Candela JV, Bellman GC. Ureteral stents: impact of diameter and composition on patient symptoms. J Endourol. 1997;11(1):45–7.
Erturk E, Sessions A, Joseph JV. Impact of ureteral stent diameter on symptoms and tolerability. J Endourol. 2003;17(2):59–62.
Chandhoke PS, Barqawi AZ, Wernecke C, Chee-Awai RA. A randomized outcomes trial of ureteral stents for extracorporeal shock wave lithotripsy of solitary kidney or proximal ureteral stones. J Urol. 2002;167(5):1981–3.
Damiano R, Autorino R, De Sio M, Cantiello F, Quarto G, Perdonà S, et al. Does the size of ureteral stent impact urinary symptoms and quality of life? A prospective randomized study. Eur Urol. 2005;48(4):673–8.
Beysens M, Tailly TO. Ureteral stents in urolithiasis. Asian J Urol. 2018;5(4):274–86.
Denstedt JD, Wollin TA, Reid G. Biomaterials used in urology: current issues of biocompatibility, infection, and encrustation. J Endourol. 1998;12(6):493–500.
Scarneciu I, Lupu S, Pricop C, Scarneciu C. Morbidity and impact on quality of life in patients with indwelling ureteral stents: a 10-year clinical experience. Pak J Med Sci. 2015;31(3):522–6.
Koprowski C, Kim C, Modi PK, Elsamra SE. Ureteral stent-associated pain: a review. J Endourol. 2016;30(7):744–53.
Kim HW, Park C-J, Seo S, Park Y, Lee JZ, Shin DG, et al. Evaluation of a polymeric flap valve-attached ureteral stent for preventing vesicoureteral reflux in elevated intravesical pressure conditions: a pilot study using a porcine model. J Endourol. 2016;30(4):428–32.
Ritter M, Krombach P, Knoll T, Michel MS, Haecker A. Initial experience with a newly developed antirefluxive ureter stent. Urol Res. 2012;40(4):349–53.
Ecke TH, Bartel P, Hallmann S, Ruttloff J. Evaluation of symptoms and patients’ comfort for JJ-ureteral stents with and without antireflux-membrane valve. Urology. 2010;75(1):212–6.
Wolf JS, Bennett CJ, Dmochowski RR, Hollenbeck BK, Pearle MS, Schaeffer AJ, et al. Best practice policy statement on urologic surgery antimicrobial prophylaxis. J Urol. 2008;179(4):1379–90.
Riedl CR, Plas E, Hübner WA, Zimmerl H, Ulrich W, Pflüger H. Bacterial colonization of ureteral stents. Eur Urol. 1999;36(1):53–9.
Kehinde EO, Rotimi VO, Al-Hunayan A, Abdul-Halim H, Boland F, Al-Awadi KA. Bacteriology of urinary tract infection associated with indwelling J ureteral stents. J Endourol. 2004;18(9):891–6.
Akay AF, Aflay U, Gedik A, Sahin H, Bircan MK. Risk factors for lower urinary tract infection and bacterial stent colonization in patients with a double J ureteral stent. Int Urol Nephrol. 2007;39(1):95–8.
Betschart P, Zumstein V, Buhmann MT, Albrich WC, Nolte O, Güsewell S, et al. Influence of biofilms on morbidity associated with short-term indwelling ureteral stents: a prospective observational study. World J Urol. 2019;37(8):1703–11.
Stewart PS. Mechanisms of antibiotic resistance in bacterial biofilms. Int J Med Microbiol. 2002;292(2):107–13.
Betschart P, Zumstein V, Buhmann MT, Altenried S, Babst C, Müllhaupt G, et al. Symptoms associated with long-term double-J ureteral stenting and influence of biofilms. Urology. 2019;134:72–8.
Kram W, Buchholz N, Hakenberg OW. Ureteral stent encrustation. Pathophysiology. Arch Esp Urol. 2016;69(8):485–93.
Cadieux PA, Chew BH, Nott L, Seney S, Elwood CN, Wignall GR, et al. Use of triclosan-eluting ureteral stents in patients with long-term stents. J Endourol. 2009;23(7):1187–94.
Torrecilla C, Fernández-Concha J, Cansino JR, Mainez JA, Amón JH, Costas S, et al. Reduction of ureteral stent encrustation by modulating the urine pH and inhibiting the crystal film with a new oral composition: a multicenter, placebo controlled, double blind, randomized clinical trial. BMC Urol. 2020;20(1):65.
WHOQOL—Measuring Quality of Life| The World Health Organization [Internet]. [citado 10 de diciembre de 2020]. https://www.who.int/toolkits/whoqol.
Joshi HB, Newns N, Stainthorpe A, MacDonagh RP, Keeley FX Jr, Timoney AG. Ureteral stent symptom questionnaire: development and validation of a multidimensional quality of life measure. J Urol. 2003;169(3):1060–4.
Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–83.
Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53–72.
Vega Vega A, García Alonso D, García Alonso CJ. Evaluación de clínica y calidad de vida con catéteres ureterales de tipo doble pig-tail. Actas Urol Esp. 2007;31(7):738–42.
Irani J, Siquier J, Pirès C, Lefebvre O, Doré B, Aubert J. Symptom characteristics and the development of tolerance with time in patients with indwelling double-pigtail ureteric stents. BJU Int. 1999;84(3):276–9.
Ucuzal M, Serçe P. Ureteral stents: impact on quality of life. Holist Nurs Pract. 2017;31(2):126–32.
Leibovici D, Cooper A, Lindner A, Ostrowsky R, Kleinmann J, Velikanov S, et al. Ureteral stents: morbidity and impact on quality of life. Isr Med Assoc J. 2005;7(8):491–4.
Lu J, Lu Y, Xun Y, Chen F, Wang S, Cao S. Impact of endourological procedures with or without double-J stent on sexual function: a systematic review and meta-analysis. BMC Urol. 2020;20(1):13.
Eryildirim B, Tuncer M, Kuyumcuoglu U, Faydaci G, Tarhan F, Ozgül A. Do ureteral catheterisation procedures affect sexual functions? A controlled prospective study. Andrologia. 2012;44(Suppl 1):419–23.
Mosharafa A, Hamid MAE, Tawfik M, Rzzak OAE. Effect of endourological procedures on erectile function: a prospective cohort study. Int Urol Nephrol. 2016;48(7):1055–9.
Zhu C, Qu J, Yang L, Feng X. The Chinese linguistic validation of the Ureteral Stent Symptom Questionnaire. Urol Int. 2019;102(2):194–8.
Giannarini G, Keeley FX, Valent F, Manassero F, Mogorovich A, Autorino R, et al. Predictors of morbidity in patients with indwelling ureteric stents: results of a prospective study using the validated Ureteric Stent Symptoms Questionnaire. BJU Int. 2011;107(4):648–54.
Tanidir Y, Mangir N, Sahan A, Sulukaya M. Turkish version of the Ureteral Stent Symptoms Questionnaire: linguistic and psychometric validation. World J Urol. 2017;35(7):1149–54.
Abt D, Warzinek E, Schmid H-P, Haile SR, Engeler DS. Influence of patient education on morbidity caused by ureteral stents. Int J Urol. 2015;22(7):679–83.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2022 The Author(s)
About this chapter

Cite this chapter
Bargues-Balanzá, M., Ordaz-Jurado, G., Budía-Alba, A., Boronat-Tormo, F. (2022). Ureteral Stents. Impact on Patient’s Quality of Life. In: Soria, F., Rako, D., de Graaf, P. (eds) Urinary Stents. Springer, Cham. https://doi.org/10.1007/978-3-031-04484-7_5
Download citation
DOI: https://doi.org/10.1007/978-3-031-04484-7_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-04483-0
Online ISBN: 978-3-031-04484-7
eBook Packages: MedicineMedicine (R0)