
Abstract
This chapter takes as its starting point theorizing around nutrition and food system transitions thought to be increasingly occurring in urban Africa, and how this may be linked to a growing non-communicable disease burden. We focus specifically on the secondary city context by analysing household survey data gathered from six cities across Ghana, Kenya and Uganda during 2013–2015. We asked how diet composition and diversity, food sources and food security varied by socio-economic status, using expenditure and demographic data to create a proxy for household well-being. In this way, we investigate one of the claimed keystones affecting urban food systems and dietary health in sub-Saharan Africa—that of obesogenic urban food environments. Our findings indicate that the socio-economic status of a household was the most important factor influencing household dietary diversity and food security status, i.e. better-off households were more likely to feel food secure and eat from a greater variety of food groups. In addition, the number of income sources was additionally associated with higher dietary diversity. We also found that a household’s involvement in agriculture had only a small positive effect on food security in one city and was associated with a reduction in dietary diversity scores. Our findings emphasize the importance of supporting aggregated national and international statistics on agricultural production and trade with detailed local analyses that focus on actual household food access and consumption. We also see reasons to be cautious about making causal claims regarding consumption change and obesogenic urban environments as the major contributor to a rising obesity and non-communicable disease burden in Africa.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others
Keywords
Introduction
In their analysis of the stage of food system transformation in sub-Saharan Africa (SSA), Steven Haggblade et al. (2016) place Ghana and Kenya in the middle tier, with Uganda on the bottom tier at a stage of early food system transition. They draw upon the work of Barry Popkin (2001, 2015; Popkin et al., 2012), Carlos Augusto Monteiro et al. (2013), David Tschirley and Thomas Reardon (Reardon et al., 2013; Tschirley et al., 2015), as well as public health research into obesity and other non-communicable diseases (NCDs) such as diabetes, hypertension and heart disease (Abrahams et al., 2011; Mayega et al., 2012; Steyn & Mchiza, 2014) in their analysis. According to Haggblade et al. (2016), a food or dietary transition entails “increased consumption of dairy and meat products, higher demand for fresh fruits and vegetables, and increased demand for processed and prepared convenience foods” (p. 220) and a transformation towards a highly marketized and industrialized agri-food industry. This kind of food system transition draws heavily from the South African experience, which is held out as the most advanced transformation, with much-debated consequences for overweight, obesity, diabetes and hypertension (Haggblade et al., 2016).
Another dimension of this interpretation of a food system transition includes eating outside the home more, consuming more energy-dense snack foods, more fried foods and more carbonated drinks, and greater capture of the food value chain by supermarkets and big food industry (Haggblade et al., 2016; Popkin et al., 2012). As Popkin notes, “Concurrent shifts are seen in two dimensions of the food system: the rapid growth of modern retailing and consumption of consumer packaged foods and beverages and the shift of the food value chain from traditional traders and retailers to one where supermarkets and food manufacturers directly source food from farmers and traders” (Popkin, 2014, p. 91). In addition, while informal small and medium-sized enterprises still dominate the sector of food processing as well as urban retailing of processed food in SSA, the emergence and rapid growth of large-scale enterprises in both sectors have recently been clearly documented (Reardon et al., 2021). Drivers of these food system changes are thought to be urbanization (an increasing share of the population living in urban areas) (Satterthwaite et al., 2010) and per capita income increases (Haggblade et al., 2016), which Julian May terms as important “keystone” socio-economic interactions that work together to “reconfigure the food system in SSA” (May, 2018, p. 6). May describes four keystone influences that are reworking African food systems: economic growth and rapid urbanization; inequality and a growing middle class; obesogenic urban food environments; and a rising prevalence of NCDs (May, 2018). May notes, drawing also from Popkin’s work, that urban residents are more prone to purchase convenience foods, highly processed foods, to eat out, to consume more sweetened or salty and fatty foods and to drink more carbonated products (May, 2018). Often these claims of such trends are based on national and international datasets of agricultural production, of supermarket and agribusiness presence, of Gross Domestic Product (GDP) data and of supply within the urban environment, or with data from the capital city (Mackay, 2019b). We explore these claims of food system transition at the finer-grained scale of households in six secondary cities of Ghana, Kenya and Uganda by analysing food sourcing strategies, which food groups were actually consumed, dietary diversity and food insecurity experience, disaggregated by socio-economic status (SES). In addition, we analyse how these three countries and six cities compare, given their experience of diet-related health problems and their purported different stages in food system change.
The chapter continues with a short description of the country and city contexts before describing the methodology. We then present the results of our analysis of household food environments and experience of food insecurity disaggregated by SES. By food environment, we refer to the definition by Christopher Turner et al. (2018, p. 95), with the focus on both access and consumption, whereby the food environment denotes “the interface where people interact with the wider food system to acquire and consume foods”. We close the chapter with a consideration of the implications of our findings and cross-country analysis, before making some conclusions.
Positioning of the Research
To further contextualize our case countries of Ghana, Kenya and Uganda, this section provides a brief overview of their urban context, their food security and nutritional status, and their health and NCD experience. Kenya and Uganda border each other in East Africa, whereas Ghana is situated in West Africa. The World Bank considers Ghana and Kenya as lower/middle-income countries and Uganda as a low-income country (World Bank, 2016). The UN’s Human Development Index (UN, 2020) puts Ghana at 0.596 (rank 142), Kenya at 0.579 (rank 147) and Uganda at 0.528 (rank 159) in the world, implying they are in fairly similar positions. The study cities included Tamale and Techiman in Ghana, Kisumu and Thika in Kenya, and Mbale and Mbarara in Uganda.
The largest two cities in terms of population were Kisumu and Tamale (Table 10.1). The other cities had about 100,000 inhabitants when surrounding peri-urban and rural areas that are part of official census data are excluded. In terms of character, Thika, only 56 kilometres from the capital of Nairobi, is an industrial town, with a fair share of manufacturing industries (Omondi et al., 2017). Techiman is an agricultural and market town, similar in this way to Mbale. Kisumu, Tamale and Mbarara are regional centres of trade and administration, with significant agricultural trading and agro-processing activity. Food prices are generally cheaper in Techiman than in Tamale, cheaper in Thika than Kisumu, and cheaper in Mbale than Mbarara, due to these areas being closer to agricultural heartlands.
As Arabella Fraser et al. (2017, p. 106) note in an analysis of the need for more resilient urban development in SSA, “smaller urban centres are greatly under studied”. David Satterthwaite also argues for the need to research patterns and processes in smaller cities, noting that more than half of SSA’s urban population lives in cities of fewer than 500,000 and many in urban areas much smaller than this, with these smaller cities often growing most rapidly (Satterthwaite, 2017). About 44% of Ghana’s population (data from 2000) lived in urban areas, whereas 23% of Kenya’s population (2009 data) and just 16% of Uganda’s population (2014 data) were urban residents (Satterthwaite, 2017). Looking at the distribution of this urban population across city size shows the majority living in cities of less than half a million (Table 10.2). In fact, 67% of Uganda’s urban population and 64% of Ghana’s lived in cities of fewer than 200,000 inhabitants. Kenya has a few more large cities (the capital, Nairobi, in particular) than Ghana and Uganda and thus only 44% of its urban population residing in cities of less than 200,000.
Given this context, and the prediction that a large share of the world’s future growth will occur in urban Africa and Asia (Tacoli, 2017), many researchers and organizations are now raising concerns about a growing urbanization of poverty and food insecurity in Africa (Cobbinah et al., 2015; Dodman et al., 2017; Tacoli, 2017). As Cecilia Tacoli (2017) emphasizes, food security in urban Africa is closely tied to income and thus to the employment situation, but non-income dimensions of poverty (such as cooking space, farming space, social networks, rural linkages, infrastructural, environmental or geographic conditions) all play an important role in urban food poverty and in the multiple dimensions of malnutrition. A number of researchers have been raising concerns about an overemphasis on the production side of food security and have called for a disaggregated analysis of actual access to and consumption of food within a household (Crush & Battersby, 2016; Mackay, 2019a; Nichols, 2017; Tacoli, 2017). This chapter forms a contribution to such knowledge gaps on food security, dietary diversity and food sourcing at the secondary city level within SSA. Recent findings have added weight to the view that food can be a useful lens to assess urban food, livelihood and health systems and how they interrelate, providing a possible entry point for improved urban planning (Battersby & Watson, 2019a, 2019b).
Finally, linking to the opening discussion about the links between a diet/nutrition transition and an epidemiological shift from communicable towards non-communicable diseases, what is currently known for cities of Ghana, Kenya and Uganda? In a recent systematic review of 48 studies encompassing more than 48,000 individuals across Ghana, Richard Ofori-Asenso et al. (2016) found overweight prevalence levels in urban Ghana of 27% and obesity prevalence of 21%. The World Health Organization’s (WHO’s) Global Health Observatory data repository describes adult (over 18 years old) Ghanaian prevalence of raised blood pressure at 19%, diabetes at 5% and obesity at 10% (female obesity 15%). Kenyan prevalence of raised blood pressure was 20%, diabetes 4%, obesity 6% (9% in females). Ugandan prevalence of raised blood pressure was also 20%, diabetes 3% and obesity 4% (7% in females) in 2016 (WHO, 2020). The same database notes that 43% of all deaths in 2016 in Ghana were due to NCDs, with the Kenyan figure at 27% and the Ugandan at 33% (WHO, 2020).
We were not able to find prevalence measures for NCDs disaggregated to the study cities for Ghana and Kenya, but our own measurement of BMI data in the Ugandan cities found a 26% prevalence of overweight in Mbale (number of adults: 1,248), 28% in Mbarara (number of adults: 948). The obesity prevalence was 14% in Mbale and 22% in Mbarara (Mackay et al., 2018). Females were more affected than males, with 18% female obesity in Mbale (of 810 women) and 27% obesity in Mbarara (of 636 women) (Mackay et al., 2018). According to the International Diabetes Foundation’s online atlas, both Ghana and Uganda had an age-adjusted diabetes prevalence level of 2.5% in 2019, while the Kenyan figure was 3.1% prevalence (IDF, 2019). These figures give a brief overview of the NCD experiences of these countries. These figures also suggest that, despite Uganda being at a less advanced stage of claimed food system and nutritional transitions, with still high urban food insecurity and low dietary diversity (as discussed in the introduction), the prevalence of NCDs equate with (in some cases even exceed) those of Ghana and Kenya. This suggests a need for caution in making causal assumptions about food system transitions, nutritional transitions and obesogenic food environments causing epidemiologic shifts. Indeed, much research has been investigating the link between early-life and in-utero undernutrition (linked to poverty) and later life predisposition of obesity and other NCDs—known by many as Barker’s hypothesis, or the development origins of disease (Barker, 1997).
Methodology
Sampling and Data Collection
The data was gathered as part of a collaborative research project between the Universities of Lund, Umeå and the Swedish University of Agricultural Sciences and the University of Ghana, the University of Nairobi, Kenya and Makerere University, Uganda. Since the Ugandan survey added a health section and included the measurement of adult heights and weights, ethical approval was obtained from the Umeå Regional Ethical Review Board and the Uganda National Council of Science and Technology. The household survey was conducted in October 2013 (Ghana), November and December 2013 (Kenya) and from June to August 2015 (Uganda), with the support of the African Food Security Urban Network (AFSUN). AFSUN granted permission to build from its already tested Household Food Security Baseline Survey instrument, which had been used to survey livelihood circumstances and food access in 11 cities across nine southern African countries in 2008 and 2009 (Crush et al., 2012). The choice of countries and cities in our study was purposive, based on a combination of contacts, practicalities and understanding of local food-related urban conditions. As such, they are not considered representative of all secondary cities in each country, nor of all SSA countries. Thus, we do not generalize our results beyond our study cases, although we believe that our findings may have relevance for other secondary SSA cities.
Further details of the systematic random sampling of every third household across a city neighbourhood, the use of tablet computers and open data kit software as a method of standardizing data entry and minimizing data collection errors and facilitating daily data checking algorithms, as well as the selection of city quadrants in the cases where all neighbourhoods could not be surveyed (specifically Tamale and Kisumu) have been discussed in previous research (Ayerakwa, 2017; Crush et al., 2012; Mackay, 2018; Omondi et al., 2017). A total of 6,013 households were surveyed, encompassing a total of 20,813 individuals.
Sample and Variables
Table 10.3 provides a summary description of the survey sample from each city as well as the explanatory variables and codes used in our modelling. The “food transfers” variable relates to whether the household reported receiving food from rural- or urban-based friends or relatives during the year preceding the survey. The “engagement in agriculture” variable presents the proportion of households who reported farming or gardening some of their crops or livestock from either an urban area, a rural area, or both, during the year prior to survey. The “income diversity” variable counts the number of different income sources that the household head reported drawing from during the preceding year. The mean number of income sources ranged from 1.3 in Ugandan cities to 1.8 in Kisumu, suggesting that a number of families tried to draw from multiple strategies in these contexts. During the survey, we also asked for the location where the main meal of each household member had been eaten the preceding day and asked respondents about the various places that they sourced food from and what other sourcing strategies they had.
Socio-Economic Status Groupings
The SES indicator in Table 10.3 is based on responses to survey questions about expenditures made monthly (such as rent, food, utilities, transportation costs, etc.) and annually (such as school fees, books, uniforms, medical expenses, insurance costs, funeral- or wedding-related). We calculated a monthly expenditure total (monthly costs, plus one-twelfth of the total annual costs reported for each household) per adult equivalent (deemed as of working age, i.e. 16–60 years of age) in the household. Calculating “per adult equivalent” takes into account the age structure and demographic makeup of the household, including the number of dependents per working-age adult. An adult equivalent score is calculated by assigning adult household members (16–60 years) a value of one, with children (0–15 years of age) given a value of 0.5 and elderly household members (>60 years) given a value of 0.75. Techiman, Kisumu and Mbarara all had a mean adult equivalent score of 3.6, whereas Thika scored 4 and Mbale scored 2.8. Our computed monthly expenditure variable was converted to US dollars,Footnote 1 then divided by household adult equivalent to allow a fair comparison across households and cities/countries. In order to equate the dollar purchasing power across the countries, the Ghanaian and Kenyan costs were adjusted using 2015 consumer price index values (translated into US dollars) to match to the time of the Ugandan survey to enable fair cross-country comparison.
For each country, households were then grouped into quartiles using this US dollar monthly expenditure per adult equivalent, with the first (0–25%, or the poorest 25% in each city), second (26–50%), third (51–75%) and fourth (>75%, or the best-off 25% in each city) quartiles corresponding to low-income, mid-lower, mid-upper and upper-income households, respectively. The resulting variable is called the SES quartile (Table 10.3) and allows fair cross-comparison across households, cities and countries, and was the variable used as a proxy for the SES of a household, better reflecting the living conditions of a family than an assessment based on self-reported income or on expenditure alone. The cut-off points for the SES quartiles for each country are shown in Table 10.4. Ghana and Kenya had roughly similar percentile cut-off points and the Ugandan levels were approximately half the Ghanaian and Kenyan values. This difference is another indicator of how Uganda is somewhat further behind Ghana and Kenya in its economic development, as noted in our introduction. Using this method, our analysis and modelling thus consider other aspects of well-being, such as household size and number of dependents, rather than purely monetary indicators, and additionally analyses households’ dietary and food security circumstances.
Food Insecurity Data
The questionnaire survey also gathered data on the experience of food insecurity using the internationally validated measure of the Household Food Insecurity Access Score (HFIAS) and the associated grouping in prevalence categories of food secure, mildly food insecure, moderately food insecure and severely food insecure known as the Household Food Insecurity Access Prevalence (HFIAP) recognized by the Food and Agriculture Organization and other international agencies (Coates et al., 2007). We use these categories in the modelling (see statistical modelling section below), but simplified into two groups. Households were grouped as food secure if they fell into the HFIAP categories of food secure or mildly food insecure. The food insecure households consisted of those that were moderately and severely food insecure. Summary description of these data per city is shown in Table 10.4. Notable is that households in Kisumu and Mbale reported greater food insecurity (Table 10.5). This is not surprising: as stated earlier, Uganda is further behind Ghana and Kenya in its urbanization, its dietary transition and general development (Haggblade et al., 2016), and Kisumu is known to struggle with informality, rapid population growth, poor infrastructural and transport connections resulting in higher food prices, as well as being a net importer of food (Wagah et al., 2018).
Dietary Diversity Data
Twelve food groups were used in the Household Dietary Diversity section of the survey. These included: (1) cereals/grains (such as maize, sorghum, millet, rice or wheat); (2) roots and tubers (such as potatoes, sweet potatoes, cassava, yam); (3) vegetables; (4) fruits; (5) meat or meat products, including poultry and game; (6) eggs; (7) fish, shellfish or fish products; (8) legumes (including beans), nuts or seeds; (9) milk or other dairy products; (10) oil, fat and butter (11) sugar, honey or sweeteners; and (12) condiments, spices, tea and coffee. This data allowed calculation of the Household Dietary Diversity Score (HDDS), following the guidelines by the Food and Nutrition Technical Assistance Project (FANTA), an international collaborative initiative spearheaded by USAID (Swindale & Bilinsky, 2006). HDDS provides a measure of the diversity of a household’s diet, with zero being the minimum score (consumed nothing during the 24 hours prior to the survey) and 12 being the maximum.
Additional only to the Ugandan survey, we did ask specific questions about the consumption of fried snacks, doughnuts, chips and fried meats, and the consumption of sugar and carbonated drinks (sugar-sweetened beverages). We also measured the heights and weights of willing adults in order to gain a body mass index (BMI) measure.
Table 10.5 summarizes the food insecurity and dietary diversity data, allowing a city/country cross-comparison. Notable from this is that the Ugandan cities had a slightly less diverse diet than the Ghanaian and Kenyan cities, especially Mbale. The low-diversity, carbohydrate-focused diet of Uganda has been found in a number of other studies (Ngaruiya et al., 2017; Raschke & Cheema, 2008).
Analytical Process and Statistical Modelling
Data was analysed using SPSS version 20. The data on the composition of the household food baskets, household experience of food insecurity and household dietary diversity, as well as the main sources of food, was all analysed against our SES proxy. In terms of our analytical process, we first explored the descriptive statistics of household dietary diversity and household food insecurity and compared differences in mean using ANOVA. Furthermore, consumption data, split by food groups and food sources were compared across SES quartiles using the Mann Whitney U test. We then performed a logistic regression model on the household food security, and a Poisson regression model on the household dietary diversity data. Our aim with the modelling was to explore the factors that may be associated with food security and dietary diversity.
In modelling the HFIAP data, we were interested in exploring the relationship between food security status and our SES proxy, as well as other socio-economic and geographic variables. We were also interested in exploring how these factors may differ across the country and city contexts. Our dependent variable is binary, taking the value of one if a household was food secure and zero if a household was food insecure (see Table 10.5 for city-level descriptive). A logistic regression model is appropriate in modelling the relationship between a binary dependent variable and selected explanatory variables (Cramer, 2003; Wooldridge, 2013). A description of the variables used in the models can be viewed in Table 10.3. Inclusion of these variables was motivated by literature on food security.
In modelling household dietary diversity scores, we included all 12 food groups (values 0–12). Thus, the dependent variable is a non-negative count variable that takes relatively few values. An appropriate model to use with such data is a Poisson regression model (Cramer, 2003). The modelling of HDDS is looking to explain factors that may be contributing to an increase in dietary diversity.
Initially, we tested whether consumption of healthier food groups (such as fruits, proteins, vitamin-rich groups) differed from consumption of less healthy food groups (such as oils/fats, sugars/sweeteners, condiments) to explore whether different factors might influence consumption of different kinds of diets. This was in recognition that a straightforward numerical increase in HDDS does not necessarily indicate a healthier dietary consumption if many of the additional food groups were oils, sugars or condiments. We also tested whether removing the food group of cereals/grains from the HDDS (where the HDDS dependent variable would thus run from 0 to 11) reduced possible skewing effects since a majority (80–99% of households, see Table 10.6) consumed this food group (with the exception of Techiman, where 78–87% consumed cereals/grains). However, all of these models produced the same significant explanatory variables with the same effect directions, just with a variation in the magnitude of the effect. We concluded that modelling the overall change in all 12 food groups was the best methodological approach, which also did not entail making judgements open to debate in terms of which foods are healthier or less healthy.
Limitations
The data is cross-sectional data at one point in time. As such, it presents a snapshot only and does not show change over time. The use of expenditure data as a proxy for the SES of a household has limitations, but has nevertheless been shown to provide a more accurate assessment of a household’s circumstances than self-reporting of incomes. Laura Howe et al. (2008), for example, note that it is “widely asserted that consumption expenditure is a better marker of long-term SEP [socio-economic position] than income”, in low-income countries in particular.
The 24-hour recall of diet content has certain limitations in terms of respondent memory, awareness of all household members’ food consumption during the preceding day and willingness to divulge information (similar critique may be levied at the household food insecurity questionnaire). Yet, these two internationally tested and validated measures of household food environments are still held to be important diet quality (energy content) and food security tools to assess food access in a review by Jef Leroy et al. (2015).
There were likely some limitations imposed by the means of collecting the food group data: this was not measured but self-reported and therefore vulnerable to variation in respondent recall and by how detailed individual enumerators were when asking about oil, vegetables mixed into sauces, etc. Our data was also limited to the gathering of information under the 12 food group categories and we did not ask how foods were cooked (fried in oil versus boiled, for example). We also recognized that a higher dietary diversity does not necessarily equate linearly to a healthier diet, but rather depends on which food groups were being consumed, as well as how they were cooked. Our data could also not account for allocation within a household, nor portion size assessments.
There were also some limitations in the food sourcing data in the way that certain categories in the questionnaire were grouped, in particular putting the “small shop” category together with “restaurant or takeaway”. It was our feeling from carrying out the surveys, and from our own knowledge of local dietary and food access practices in these cities, that the majority of responses here related to small local shops, not to restaurants, fast food chains or takeaways. Similarly, the merging into one category of “informal markets” with “street foods” as a food source is also slightly misleading. Again, our experience indicates that these responses related to the traditional neighbourhood/city centre marketplaces, where the majority across all countries and cities still bought the bulk of their food.
Findings
In Ghana, Tamale residents spent 41% of their monthly expenditures on food and Techiman 39% (data not shown). The Kenyan cities of Kisumu and Thika had the highest share of monthly expenditure going towards food at 46 and 45%, respectively. Households in Mbale and Mbarara reported the lowest share of food expenditure at 33 and 35%, respectively.
Exploring the descriptive data on which specific food groups were consumed by households of different SES shows that the largest difference between the lowest and the highest SES was in the consumption of milk (+30% points [pp]) and meat (+41 pp) in Tamale, milk (+28 pp in Kisumu) and fruit (+28 pp) and meat (+28 pp) in Thika (calculated from Table 10.6). Whereas in Uganda the greatest difference between the lowest and highest SES was a 28% higher consumption of sugar (calculated from Table 10.6). A majority (>78%) of all SES consumed food made from cereals and grains (Table 10.6 [note that the second and third quartiles are not shown in table]). Table 10.5 also shows low consumption of vegetables in the Ugandan cities and fairly low consumption of fruits across all countries. The proportion of the best-off households (fourth quartile) consuming meat/meat products or fish/fish products remained less than 50% in Kenya and Uganda. Milk and milk products were increasingly consumed with rising SES across all cities and countries. A higher proportion of households in Kisumu and Thika reported consuming sugar compared to the other four cities, across all wealth groups. The experience of the research team indicates most Kenyans and Ugandans prefer their tea or coffee with sugar, which may explain some of the high proportion consuming sugar. Generally, consumption of oils and fats was reported by a large share of households in Kisumu and Thika compared to other cities. These data already indicate some dietary transformation towards consumption of more fruits, meat and milk products with rising SES, but also towards less healthy food groups as household welfare improves.
In keeping with theories of how dietary diversity and food security might change with improved SES, Table 10.7 shows that the score of food insecurity diminished with increasing SES across all cities, although even the highest SES households in Kisumu and Mbale still experienced some food insecurity, in Kisumu (HFIAS: 7) and Mbale (HFIAS: 5.34) in particular. Table 10.7 also shows that the highest SES households had an approximately two food groups greater mean dietary diversity score than the lowest SES across all cities, which constitutes a reasonable difference within a maximum score of 12.
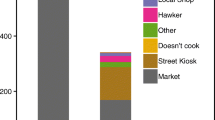
We also investigated the ways in which households accessed food (both market and non-market sources). Table 10.8 presents the results, showing that the traditional markets (including neighbourhood markets and city centre markets) were the most commonly used source across most cities, countries and SES. Small local shops were the second most used (note category limitations outlined above).
The category of central or neighbourhood market was the main source of food in all the cities, closely followed (in Kenya and Uganda in particular) by buying food from the nearest small shop (Table 10.8). Approximately 30–40% of households across all cities and countries were involved in growing some of their own food and this remained stable across SES (the second and third SES quartiles not shown). The likelihood of purchasing food from supermarkets increased with rising SES, although remaining fairly low (between 22 and 47% of the households in the highest SES quartile in both the Ugandan and Ghanaian cities). Kenyans, across all SES but especially in the highest SES, more commonly sourced food in supermarkets than Ghanaians or Ugandans. However, only a small proportion of the lowest SES households purchased food from supermarkets, especially in Techiman and Mbale. There may be a city-size or outlet availability factor influencing this data. The proportion of the highest SES quartile of households in all cities, except Thika, that purchased food from supermarkets, was more than double the proportion of the lowest SES households, but this better-off SES also continued to source food from the traditional markets (and even increasingly so in Ghana and Uganda).
Food transfers from friends and relatives were a source of food for between approximately 31% and 55% of households (Table 10.8). While in the Ghanaian and Kenyan cities the proportion receiving food transfers remained relatively similar across SES, in the Ugandan cities higher SES households more commonly received food transfers than lower SES households. This trend in Uganda has been discussed by other researchers as relating to the tendency for urban-based Ugandans to invest any spare income into rural land and rural-based farm relationships (Kangave et al., 2016; Reid, 2017). T. S. Jayne et al. (2016) found a similar situation in Kenya, where 36% of urban households in 2014 owned agricultural land, with the corresponding figure in Ghana being just 12%.
Finally, we analysed the BMI data for the Ugandan cities by SES quartiles (Table 10.9). These findings contrast with claims that body mass and problems with overweight and obesity increase with wealth (May, 2018). Instead, they show all SES being affected by overweight and obesity, in Mbarara in particular. This data is also striking when assessed against the household dietary and food insecurity status of the cities shown in previous tables.
Factors Influencing Household Food Security
The modelling of food security is shown in Table 10.10. It indicates that the SES of a household had the largest magnitude and most significant effect on household food security across the six cities. For example, in the Ghanaian cities, with other factors held constant, a household in the upper SES group had an odds ratio of 3.5, meaning it was 3.5 times more likely to be food secure compared to a low SES household. The upper-mid and mid-lower households were 1.9 and 1.4 times, respectively, more likely to be food secure than the lowest SES households. This pattern and magnitude were broadly similar in both of the Kenyan and Ugandan cities (Table 10.10).
Household involvement in agriculture had varying influence on household food security in the three countries. There was a positive and statistically significant relation between agriculture and food security only in Ghana, and only in households that had been involved in both rural and urban agriculture during the preceding year. Such Ghanaian households were 1.8 times more likely to be food secure than those that did not practise any agriculture. The only other statistically significant implication of agriculture on food security was in Uganda where the effect was negative, opposite to that in Ghana. In Uganda the households that engaged only in urban agriculture were 0.63 times less likely to be food secure compared to households that did not practise agriculture (Table 10.10).
Other country contrasts appear in the model, but most were not highly significant or had a small magnitude effect, such as the age of the household head in Kenya, or being more food secure in multiple adult households (1.2 times more likely) in Uganda compared to single adult households. City differences were significant in Kenya and Uganda, where those living in Thika had a 4.1 times greater likelihood of being food secure than those who lived in Kisumu (Table 10.10). Similarly, those living in Mbarara were 1.6 times more likely to be food secure than those living in Mbale.
The clearest message from Table 10.9, however, across these three countries and six secondary cities, was that our SES quartile was most significant and had the greatest magnitude of influence on whether a household felt food secure.
Factors Influencing Household Dietary Diversity
The Poisson regression modelling of household dietary diversity is presented in Table 10.11.
Similar to the findings for factors influencing food security, the analysis of factors influencing household dietary diversity in Table 10.11 indicates that, across all three countries and all six secondary cities, being in a higher SES quartile household was significantly and positively associated with better dietary diversity. Such a finding is not unexpected and fits with the literature. To specify, other factors held constant, being in an upper SES household increased the HDDS by 187% in Ghana, by 140% in Kenya and 133% in Uganda compared to the lowest SES quartile. In addition, the diversity of income sources was significantly associated with an increase in dietary diversity, with the effect being 51% and 32% in Uganda and Ghana, respectively, but just 12% in Kenya (Table 10.11).
Yet, a number of other explanatory variables seemed to influence household dietary diversity in comparison with the influences on household food security (previous model, Table 10.10), and there was more variation across the countries on which factors had a significant influence on dietary diversity in comparison with the influences on food security. City variations in modelling dietary diversity were also apparent, significant in all three countries: being a resident of Techiman increased household dietary diversity by 78% compared to Tamale, while households in Thika were 69% more likely to have a higher dietary diversity score than their Kisumu counterparts. Mbarara households had 90% higher HDDS than Mbale households (Table 10.11), other factors being held constant. In the Kenyan cities, the household structure, gender and age of the household head had significant and positive effects on the HDDS. A Kenyan household with multiple adults increased dietary diversity by 18% compared to households with single adults. Additionally, male-headed households had 32% higher dietary diversity than female-headed households (Table 10.11).
Of interest was the relation of agriculture with dietary diversity. The engagement of households in agricultural activities had a statistically significant and negative effect on dietary diversity in both the Ghanaian and Kenyan cities, but no effect in Uganda (Table 10.10). Those households that had engaged in rural agriculture during the preceding year had a lower dietary diversity score by 49 and 29% in Ghana and Kenya, respectively. In the same countries, engagement in both urban and rural agriculture reduced dietary diversity by 47 and 30%, respectively (Table 10.10).
The Complexity of Change in Secondary City Food Systems
In this chapter, we have analysed how diet composition and diversity, food sources and food security varied by the SES of a household (a proxy for well-being calculated from monthly and annual expenditure data and considering the age structure and composition of household members) in six secondary cities across Ghana, Kenya and Uganda. We find that food security and dietary diversity improved with increasing SES. This finding is supported by numerous other studies, for example, in a recent review of urban food environment change in Africa by Michelle Holdsworth and Edwige Landais that also highlights the importance of “wealth” (Holdsworth & Landais, 2019) and Tacoli’s study noting the importance of “income” (Tacoli, 2017). We suggest, more precisely, that what is important here is actually cash availability, that is disposable income. Such a growth in disposable income is why we think that having multiple income sources was positively correlated with dietary diversity.
From the modelling, we find an association of better food security and higher dietary diversity with greater SES, across all three SSA countries and all six secondary cities. The SES variable alone accounted for a significant magnitude of the difference in the experience of food security in all contexts: the more money a household spent, the more food secure they felt. The significantly lower level of food security found in Kisumu in comparison to Thika (Table 10.5) was expected, since Kisumu is characterized by a high number of informal settlements and is a net food importer and thus food is more expensive, as noted in the introduction and found by Wagah et al. (2018).
The effect of engagement in agriculture (either in rural areas or within an urban area, or both) by urban-based households did not have a statistically significant positive impact on food security in our model (Table 10.10), except in Ghana and then only for households who farmed in both a rural and an urban area (thus households more likely to have more resources, assets and/or contacts). In Uganda, households that practised urban agriculture had a negative association with food security (Table 10.10). Although these findings do not necessarily provide strong support for the thesis that own crop or livestock production improves food security, the practice should not be regarded as unimportant. As shown already in Table 10.8, approximately 30–40% of all households across all SES groups noted growing their own food as an important food source, and authors’ previously published studies in these cities note the common and persistent engagement in agriculture across SES, with indications that this even increases with SES whereby the better-off urban residents invest in agriculture as a diversification and a livelihood security strategy (Mackay, 2019a; Omondi et al., 2017; Turner & Jirström, 2014). Had farming households not engaged in agriculture, their food security status would likely have been much worse.
Considering the modelling of the factors influencing household dietary diversity, we found additional important influences beyond our SES proxy. Consistent across all countries was the role of the number of income sources. For every numeric increase in income sources, a household experienced a 12% increase in HDDS in Kenya, 32% in Ghana and a full 52% in Uganda (Table 10.11). This was after controlling for the number of adults and dependents in the household, the number of working-age members and other socio-economic and geographic factors. Households with more diversified income sources are likely more cushioned from shocks, job loss or other such change in circumstance, thus they might be expected to have been able to purchase a greater variety of food groups (resulting in higher dietary diversity scores) than those with fewer income sources. Why the role of having multiple income sources seems to have lower magnitude in the Kenyan context in comparison with the Ghanaian and Ugandan situations is intriguing and would benefit from further investigation.
The other, perhaps somewhat counter-intuitive finding relating to the modelling of household dietary diversity was the negative relationship with engagement in agriculture in Ghana and Kenya, and the non-significant effect of agriculture on dietary diversity in Uganda. Our contextual experience and other studies (Mackay, 2018, 2019a, 2019b), together with findings from other literature describing a varied and uneven link between farm production diversity and household dietary diversity (Sibhatu & Qaim, 2018), support the case that the lack of positive relation between engaging in agriculture and higher dietary diversity is likely because much of this agricultural activity is concentrated around producing the most commonly consumed food groups, in particular maize, cooking bananas, sweet potatoes and green leafy vegetables. Consumption of this agricultural produce would not broaden the dietary diversity score, since these are the most commonly eaten food groups across all contexts and all SES, and even for households not engaging in agriculture.
In summary, our findings do indicate a small decline in food insecurity and a more considerable increase in dietary diversity with a rise in SES, as theory and many other studies, such as the work of Haggblade et al. (2016), and Popkin et al. (2012; Popkin, 2001, 2015) predict. As Table 10.7 shows, the difference in mean food insecurity scores from the lowest to the highest SES amounted to 3–4 HFIAS points, and the difference in mean household dietary diversity between the lowest and the highest SES amounted to two (out of a total of 12) food groups across all cities and countries. Greater cash availability and a general increase in household circumstances (both indicated in our SES quartile variable) do seem to translate into more food secure circumstances and a greater diversity of food groups being consumed (not necessarily directly equivalent to healthy foods, as previously noted).
Yet our findings on the sourcing of food, the continuing use of the traditional marketplaces even for better-off households, the similar level of receipt of food transfers regardless of SES and the consistent engagement (even slight increase) in agriculture with greater SES may nuance how ideas of nutrition transition, or of the supermarketization of Africa, of fundamental shifts in urban food systems, of the declining relevance of land to farm, or of increasing separation of urban and rural livelihoods play out in the SSA urban context (Haggblade et al., 2016; May, 2018; Popkin, 2001, 2015; Reardon et al., 2003). Our Kenyan cities, however, do show a greater patronage of more Western-style supermarket shopping than our Ghanaian and Ugandan cities. Our focus on secondary cities may explain some of these differences in food systems. Our secondary study cities were of a rather small size compared to many capital cities or megacities, which are often the focus of research. They also lacked, except in Kisumu, the large concentrations of abject poverty (slum areas) often to be found in capitals and megacities. Our secondary cities also, due to their smaller areal spread, their infrastructure and linkages, may also allow easier access to the peri-urban and nearby rural areas than capital and megacities. These factors may signify some reasons for a possible modification of trajectories of food system change compared to those identified from large cities or from national aggregate data. However, as Reardon et al. (2021) recently note, the traditional small-scale retail and food service sectors, which our study concurs are dominant food sources in these SSA cities, are beginning to supply more ultra-processed (packaged and unpackaged) food. Our study shows that small neighbourhood stores are an important food source, and previous work by Mackay (2019a) also notes that local shop owners, with whom an individual has built a personal relationship, play a crucial role in providing food access on credit in times of stress. Thus, as Reardon et al. (2021) also note, research investigations and policy interventions should not focus only on supermarkets and large-scale processors/retailers but also consider the role of small shops and small and medium enterprises in SSA in food system change.
In addition, our descriptive data on consumption of the different food groups by SES quartile generally show an increase in consumption of all food groups with rising SES. In contrast to some of the postulations reported in May’s (2018) analysis of keystones that are reconfiguring African food systems, we do not see evidence that consumption of staple foods declines with improved circumstances in our city/country contexts (these rather increased, Table 10.5). May’s paper does recognize that consumption patterns will vary by country context and tradition. However, our data is limited by not being able to distinguish between different types of staple cereals and grains (more nutritious millets and sorghums to less nutritious or polished wheats or rice), nor the level of polishing and processing. Reardon et al. (2021), in their overview of African food system change, also point out the importance of distinguishing between types of staples, their nutrient content and their degree of processing.
Cross-city, cross-country comparison of the food consumption data by SES revealed similar broad patterns and trends of rising consumption with rising SES, despite the countries being positioned differently regarding their stage of economic development and food system transformation in the literature (Haggblade et al., 2016). However, some country differences were apparent, with the Ugandan cities reporting significantly less consumption of fruits and vegetables (remaining low even at the highest wealth quartile) than their Ghanaian (specifically Techiman) and Kenyan counterparts, the Ghanaian cities reporting higher consumption of fish than the Kenyan and Ugandan households, and the Kenyan households reporting significantly higher consumption of lower nutritional value foods (Table 10.5). While some of these differences may be a feature of data collection variations, some are indicative of different socio-cultural context and traditional dietary behaviours. The higher use of oils/fats, sugar/sweeteners and condiments, tea and coffee in Thika and Kisumu deserves further investigation.
Finally, although there was insufficient space within this chapter to analyse links to obesity or other NCDs in detail, and we did not have such data for our Ghanaian and Kenyan samples, our findings should be viewed together with the obesity/NCD data that were presented in the introduction and within Table 10.9. Our findings from the BMI data in Uganda do not strongly support claims that body mass rises with wealth and related overconsumption of particularly less healthy foods (Table 10.9). This data is striking when viewed against the household dietary and food security status of these cities presented earlier, showing more than half of households experiencing food insecurity (Table 10.4) and dietary diversity scores averaging 3–6 across all SES (Table 10.6) in Mbale and Mbarara. Viewing these BMI data also against the responses gathered in relation to our additional questioning regarding the consumption of sugar-sweetened beverages, fried foods, fast foods, regular snacking and eating out in the Ugandan cities revealed these to be uncommon habits (Mackay et al., 2018). These findings do not match well with postulations from some research on nutrition transition and food system transformation of keystone factors contributing to rising NCD experience, such as those framed by May (2018). Our findings support others who have raised the importance of understanding the social environments, local perceptions and contextual factors and of the need for deep qualitative investigation (Holdsworth & Landais, 2019; Mackay, 2020).
Conclusion
Food insecurity in secondary cities in Ghana, Kenya and Uganda is a serious challenge. In the six cities studied, a large share—between 40 and 80% (Table 10.5)—of the households felt themselves to be either moderately or severely food insecure. The Ghanaian cities were more food secure than the Kenyan (Kisumu in particular) and Ugandan cities. While variation among households was found to be clearly associated with their SES, the overall picture was some degree of food insecurity being an experiential reality, even for residents in the better-off strata.
Food security and having a diverse diet are multidimensional and require a multipronged approach, yet we find cash availability is one of the most important drivers of food security, in agreement with findings from other researchers (Holdsworth & Landais, 2019; May, 2018; Tacoli, 2017; Tschirley et al., 2015). Thus, efforts must be made to ensure that populations are able to have a reliable and liveable source of income or—even more importantly in the case of dietary diversity—multiple sources of income. This links to labour market conditions and employment and entrepreneurial opportunities, and the conditions for informal livelihoods (Mackay, 2019a; Tacoli, 2017). Important policy implications here thus relate to removing restrictions on, or punishments for, informality; working creatively with informal livelihoods; as well as trying to influence food consumption patterns by nudging consumer behaviour through subsidizing healthier food products; or by taxation and hierarchical marketing charges based on nutritional content, as Holdsworth and Landais (2019) and Reardon et al. (2021) also note.
While the effects of own food production (crop or livestock) on food security and dietary diversity was weak in our models, this does not mean it is not important. The food security situation of those engaged in agriculture would likely have been worse had they not farmed. Policies supportive of small-scale farming, as well as those increasing the possibility for multiple livelihood opportunities, offer a strategy to combat food insecurity and may encourage more diverse diets.
Our study provides a detailed analysis of how food system and nutritional change are manifesting at the household level in secondary cities of three SSA countries at slightly different stages of development. While we find processes in line with key tenets of the concept of food system and nutritional transition, we also find difference in terms of food sourcing strategies and eating behaviours. We see reason to be cautious (from the Ugandan data) about making direct causal claims regarding consumption change and obesogenic urban environments being the major contributors to a rising obesity and NCD burden in these developing countries. There needs to be an awareness among researchers, planners and decision-makers of the wider social and macro-environmental determinants of food environments and of health and disease than simply individual behaviours (food consumption) (Holdsworth & Landais, 2019). There is a need to recognize how poverty, insecure livelihoods and “unequal and unjust socioeconomic and health systems” (Mackay, 2020, p. 13) operate, together with features of the built environment, and in interaction with an individual’s (historic and present) experience of hunger and undernutrition (Barker’s development origins theory), to influence NCD expression over and above current food intake. A holistic perspective is essential.
Notes
- 1.
One US dollar was equivalent to 2.37 Ghanaian cedis (October–November 2013); one US dollar was equivalent to 86.8 Kenyan shillings (November–December 2013); one US dollar was equivalent to 3,421 Ugandan shillings (July–August 2015). The expenditures for Ghana and Kenya were adjusted using the consumer price index to 2015 values.
References
Abrahams, Z., Mchiza, Z., & Steyn, N. (2011). Diet and mortality rates in Sub-Saharan Africa: Stages in the nutrition transition. BMC Public Health, 11(1), 801.
Ayerakwa, H. (2017). Urban households’ engagement in agriculture: Implications for household food security in Ghana’s medium sized cities. Geographical Research Special Issue, 55(2), 217–230.
Barker, D. J. (1997). Maternal nutrition, fetal nutrition, and disease in later life. Nutrition, 13(9), 807–813.
Battersby, J., & Watson, V. (2019a). The planned ‘city-region’ in the New Urban Agenda: An appropriate framing for urban food security? Town Planning Review, 90(5), 497–518.
Battersby, J., & Watson, V. (Eds.). (2019b). Urban food systems governance and poverty in African cities. Routledge.
Coates, J., Swindale, A., & Bilinsky, P. (2007). Household food insecurity access scale (HFIAS) for measurement of household food access: Indicator guide (version 3). FHI 360/FANTA.
Cobbinah, P., Erdiaw-Kwasie, M., & Amoateng, P. (2015). Africa’s urbanisation: Implications for sustainable development. Cities, 47, 62–72.
Cramer, J. (2003). Logit models from economics and other fields. Cambridge University Press.
Crush, J., & Battersby, J. (Eds.). (2016). Rapid urbanisation, urban food deserts and food security in Africa. Springer.
Crush, J., Frayne, B., & Pendleton, W. (2012). The crisis of food insecurity in African cities. Journal of Hunger and Environmental Nutrition, 7(2–3), 271–292.
Dodman, D., Leck, H., Rusca, M., & Colenbrander, S. (2017). African urbanisation and urbanism: Implications for risk accumulation and reduction. International Journal of Disaster Risk Reduction, 26, 7–15.
Fraser, A., Leck, H., Parnell, S., Pelling, M., Brown, D., & Lwasa, S. (2017). Meeting the challenge of risk-sensitive and resilient urban development in sub-Saharan Africa: Directions for future research and practice. International Journal of Disaster Risk Reduction, 26, 106–109.
Ghana Statistical Service (GSS). (2012). 2010 population and housing census final results. Government of Ghana.
Haggblade, S., Duodu, K., Kabasa, J., Minnaar, A., Ojijo, N., & Taylor, J. (2016). Emerging early actions to bend the curve in sub-Saharan Africa’s nutrition transition. Food and Nutrition Bulletin, 37(2), 219–241.
Holdsworth, M., & Landais, E. (2019). Urban food environments in Africa: Implications for policy and research. Proceedings of the Nutrition Society, 78(4), 513–525.
Howe, L., Hargreaves, J., & Huttly, S. (2008). Issues in the construction of wealth indices for the measurement of socio-economic position in low-income countries. Emerging Themes in Epidemiology, 5(1), 3.
International Diabetes Foundation (IDF). (2019). IDF diabetes Atlas Ninth Edition 2019. International Diabetes Foundation.
Jayne, T., Chamberlin, J., Traub, L., Sitko, N., Muyanga, M., Yeboah, F., Anseeuw, W., Chapoto, A., Wineman, A., Nkonde, C., & Kachule, R. (2016). Africa’s changing farm size distribution patterns: The rise of medium-scale farms. Agricultural Economics, 47(S1), 197–214.
Kangave, J., Nakato, S., Waiswa, R., & Zzimbe, P. (2016). Boosting revenue collection through taxing high net worth individuals: The case of Uganda (International Centre for Tax and Development [ICTD] Working Paper No. 45). Institute of Development Studies.
Kenya National Bureau of Statistics (KNBS). (2012). 2009 Kenya population and housing census-analytical report on urbanization (Vol. VIII). Republic of Kenya.
Leroy, J., Ruel, M., Frongillo, E., Harris, J., & Ballard, T. (2015). Measuring the food access dimension of food security: A critical review and mapping of indicators. Food and Nutrition Bulletin, 36(2), 167–195.
Mackay, H. (2018). Mapping and characterising the urban agricultural landscape of two intermediate-sized Ghanaian cities. Land Use Policy, 70, 182–197.
Mackay, H. (2019a). Food sources and access strategies in Ugandan secondary cities: An intersectional analysis. Environment and Urbanization, 31(2), 375–396.
Mackay, H. (2019b). Food, farming and health in Ugandan secondary cities (PhD dissertation). Department of Geography, Umeå University.
Mackay, H. (2020). Of fatness, fitness and finesse: Experiences and interpretations of non-communicable diseases in urban Uganda. Cities and Health (published online).
Mackay, H., Mugagga, F., Kakooza, L., & Chiwona-Karltun, L. (2018). Doing things their way? Food, farming and health in two Ugandan cities. Cities and Health, 1(2), 147–170.
May, J. (2018). Keystones affecting sub-Saharan Africa’s prospects for achieving food security through balanced diets. Food Research International, 104, 4–13.
Mayega, R., Makumbi, F., Rutebemberwa, E., Peterson, S., Östenson, C., Tomson, G., & Guwatudde, D. (2012). Modifiable socio-behavioural factors associated with overweight and hypertension among persons aged 35 to 60 years in eastern Uganda. PLoS One, 7(10), e47632.
Monteiro, C., Moubarac, J., Cannon, G., Ng, S., & Popkin, B. (2013). Ultra-processed products are becoming dominant in the global food system. Obesity Review, 14, 21–28.
Ngaruiya, C., Hayward, A., Post, L., & Mowafi, H. (2017). Obesity as a form of malnutrition: Over-nutrition on the Uganda “malnutrition” agenda. Pan African Medical Journal, 28(1), Article 49.
Nichols, C. (2017). Millets, milk and maggi: Contested processes of the nutrition transition in rural India. Journal of Agriculture and Human Values, 34(4), 871–885.
Ofori-Asenso, R., Agyeman, A., Laar, A., & Boateng, D. (2016). Overweight and obesity epidemic in Ghana—A systematic review and meta-analysis. BMC Public Health, 16(1), 1239.
Omondi, S., Oluoch-Kosura, W., & Jirström, M. (2017). The role of urban-based agriculture on food security: Kenyan case studies. Geographical Research, 55(2), 231–241.
Popkin, B. (2001). The nutrition transition and obesity in the developing world. Journal of Nutrition, 131(3), 871S-873S.
Popkin, B., Adair, L., & Ng, S. (2012). Global nutrition transition and the pandemic of obesity in developing countries. Nutrition Reviews, 70(1), 3–21.
Popkin, B. (2014). Nutrition, agriculture and the global food system in low- and middle-income countries. Food Policy, 47, 91–96.
Popkin, B. (2015). Nutrition transition and the global diabetes epidemic. Current Diabetes Reports, 15(9), 64.
Raschke, V., & Cheema, B. (2008). Colonisation, the New World Order, and the eradication of traditional food habits in East Africa: Historical perspective on the nutrition transition. Public Health Nutrition, 11(7), 662–674.
Reardon, T., Timmer, C., Barrett, C., & Berdegue, J. (2003). The rise of supermarkets in Africa, Asia, and Latin America. American Journal of Agricultural Economics, 85(5), 1140–1146.
Reardon, T., Tschirley, D., Minten, B., Haggblade, S., Timmer, C., & Liverpool-Tasie, S. (2013). The emerging ‘quiet revolution’ in African agrifood systems. Brief prepared for Harnessing Innovation for African Agriculture and Food Systems: Meeting Challenges and Designing for the 21st Century; African Union Conference Centre; 25–26 November, Addis Ababa, Ethiopia.
Reardon, T., Tschirley, D., Liverpool-Tasie, S., Awokuse, T., Fanzo, J., Minten, B., Vos, R., Dolislager, M., Sauer, C., Dhar, R., Vargas, C., Lartey, A., Raza, A., & Popkin, B. (2021). The processed food revolution in African food systems and the double burden of malnutrition. Global Food Security, 28, 100466.
Reid, R. (2017). A history of modern Uganda. Cambridge University Press.
Satterthwaite, D. (2017). The impact of urban development on risk in sub-Saharan Africa’s cities with a focus on small and intermediate urban centres. International Journal of Disaster Risk Reduction, 26, 16–23.
Satterthwaite, D., McGranahan, G., & Tacoli, C. (2010). Urbanization and its implications for food and farming. Philosophical Transactions of the Royal Society B: Biological Sciences, 365(1554), 2809–2820.
Sibhatu, K. T., & Qaim, M. (2018). Meta-analysis of the association between production diversity, diets, and nutrition in smallholder farm households. Food Policy, 77, 1–18.
Steyn, N., & Mchiza, Z. (2014). Obesity and the nutrition transition in sub-Saharan Africa. Annals of the New York Academy of Sciences, 1311(1), 88–101.
Swindale, A., & Bilinsky, P. (2006). Household dietary diversity score (HDDS) for measurement of household food access: Indicator guide (version 2). FHI 360/FANTA.
Tacoli, C. (2017). Food (in) security in rapidly urbanising, low-income contexts. International Journal of Environmental Research and Public Health, 14(12), 1554.
Tschirley, D., Reardon, T., Dolislager, M., & Snyder, J. (2015). The rise of a middle class in Eastern and Southern Africa. Journal of International Development, 27(5), 628–646.
Turner, C., Aggarwal, A., Walls, H., Herforth, A., Drewnowski, A., Coates, J., Kalamatianou, S., & Kadiyala, S. (2018). Concepts and critical perspectives for food environment research: A global framework with implications for action in low- and middle-income countries. Global Food Security, 18, 93–101.
Turner, C., & Jirström, M. (2014). Staple foods in urban and peri-urban agriculture. In U. Magnussson & K. Follis Bergman (Eds.), Urban and peri-urban farming in low-income countries—Challenges and knowledge gaps (pp. 37–41). SLU Global.
Uganda Bureau of Statistics. (2016). National population and housing census 2014. Uganda Bureau of Statistics. Main Report.
United Nations (UN). (2020). Global human development indicators. United Nations Development Programme.
Wagah, G., Obange, N., & Okello Ogindo, H. (2018). Food poverty in Kisumu, Kenya. In J. Battersby & V. Watson (Eds.), Urban food systems governance and poverty in African cities (pp. 223–235). Routledge.
World Health Organization (WHO). (2006). Global database on body mass index: BMI classification. http://www.assessmentpsychology.com/icbmi.htm.
World Health Organization (WHO). (2020). Global health observatory (GHO) data. https://www.who.int/data/gho/info/gho-odata-api.
Wooldridge, J. (2013). Introductory econometrics: A modern approach (5th ed.). Nelson Education Canada.
World Bank. (2016). New country classifications by income level: 2016–2017. World Bank Data Team.
Acknowledgements
The authors would like to thank AFSUN for permission to use the AFSUN Household Food Security Baseline Survey instrument as part of this research. We would especially extend our gratitude to Cameron McCordic, Balsillie School of International Affairs, Canada, for coordinating the survey in Ghana and Kenya and his training to Heather Mackay to run the survey in Uganda. Our thanks go also to Frank Mugagga in Uganda, Daniel Bruce Sarpong and Fred Dzanku in Ghana, and Willis Oluoch-Kosura and Stephen Wambugu in Kenya for support in running the field surveys. We also thank Hayford Ayerakwa for feedback on an early draft. Last but not least, we are grateful to Agneta Hörnell, from the Department of Food, Nutrition and Culinary Science, Umeå University, Sweden, for comments and advice.
Funding
This work was supported by the Swedish International Development Cooperation Agency [grant number SWE-2011-028] and the Swedish Research Council for Environment, Agricultural Sciences and Spatial Planning [grant numbers 250-2014-1227 and 225-2012-609].
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Open Access This chapter is licensed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license and indicate if changes were made.
The images or other third party material in this chapter are included in the chapter's Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the chapter's Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
Copyright information
© 2023 The Author(s)
About this chapter

Cite this chapter
Mackay, H., Omondi, S.O., Jirström, M., Alsanius, B. (2023). Analysing Diet Composition and Food Insecurity by Socio-Economic Status in Secondary African Cities. In: Riley, L., Crush, J. (eds) Transforming Urban Food Systems in Secondary Cities in Africa. Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-030-93072-1_10
Download citation
DOI: https://doi.org/10.1007/978-3-030-93072-1_10
Published:
Publisher Name: Palgrave Macmillan, Cham
Print ISBN: 978-3-030-93071-4
Online ISBN: 978-3-030-93072-1
eBook Packages: Social SciencesSocial Sciences (R0)