
Abstract
Simulators have been traditionally used for centuries during medical training as the trainees have to improve their skills before practicing on a real patient. Nowadays mechatronic technology has open the way to more evolved solutions enabling objective assessment and dedicated pedagogic scenarios. Trainees can now practice in virtual environments on various body parts, with current and rare pathologies, for any kind of patient (slim, elderly ...). But medical students need kinesthetic feedback in order to get significant learning. Gestures to acquire vary according to medical specialties: needle insertion in rheumatology or anesthesia, forceps installation during difficult births ... Simulators reproducing such gestures require haptic interfaces with a variable rendered stiffness, featuring commonly called Variable Stiffness Actuators (VSA) which are difficult to embed with off-the-shelf devices. Existing solutions do not always fit the requirements because of their significant size. In contrast, pneumatic technology is low-cost, available off-the-shelf and has a better mass-power ratio. Its main drawback is its non-linear dynamics, which implies more complex control laws than with electrical motors. It also requires a compressed air supply. Ampère research laboratory has developed during the last decade haptic solutions based on pneumatic actuation, applied on a birth simulator, an epidural needle insertion simulator, a pneumatic master for remote ultrasonography, and more recently a needle insertion under ultrasonography simulator. This paper recalls the scientific approaches in the literature about pneumatic actuation for simulation and tools in the medical context. It is illustrated with the aforementioned applications to highlight the benefits of this technology as a replacement or for an hybrid use with classical electric actuators.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Simulators have been traditionally used for centuries during medical training as the trainees have to improve their skills before practicing on a real patient. Classical simulators feature training boxes, manikins, animals and corpses. Although these former simulators have been used for years, nowadays mechatronic technology has open the way to more evolved solutions enabling objective assessment and dedicated pedagogic scenarios. This evolution attempts to satisfy the need for efficient teaching tools invoked by public institutes such as the French H.A.S. [15] (Haute Autorité de la Santé), which asks to “never do [it] the first time on a patient”. Trainees can now practice in virtual environments on various body parts, with current and rare pathologies, for any kind of patient (slim, elderly ...). With these simulators, trainees can repeat a procedure several times without getting short of supplies (as in the case of surgery on corpses), get rapid and objective feedback from the simulator, and determine which skills they need to improve [43]. Medical students particularly need some haptic feedback to get significant learning, especially for the gestures that require kinesthetic feeling [35] (kinesthesia is the ability to sense the movement and position of the body limbs). Thanks to kinesthesia, haptic training, and in particular kinesthetic focused training, extends vision based training. Some haptic simulators are now available on the market and are used in various medical sectors [7].
Gestures to acquire vary according to medical specialties: needle insertion in rheumatology or anesthesia, forceps installation during difficult births ... Such gestures require haptic interfaces with a variable rendered stiffness which is sometimes difficult to reproduce with off-the-shelf devices (this kind of actuator is commonly called Variable Stiffness Actuator - VSA). Solutions have been proposed in the literature [8, 16, 22]. However, these solutions, based on electric or magneto-resistant fluids, do not always fit the training requirements because of their significant size. Unlike electric actuators, pneumatic cylinders are low-cost off-the-shelf components and are easy to mechanically embed. They also have a better mass-power ratio and they naturally provide a passive compliance thanks to the pressurized air contained inside their two chambers. Their drawbacks are their non-linear dynamics, which require more complex control laws than with electrical motors. They also require a compressed air supply. By modifying the pressure level in the actuator chambers, one can control the pneumatic stiffness in real-time over a large range of values starting from 0.1 N/mm, according to Takaiwa et al. in [44]. For instance, Semini et al. [38] introduced a VSA based on position-controlled hydraulic cylinders.
Position or force control of pneumatic cylinders is nowadays well mastered in the Fluid Power community as detailed in [7, 36]. However, their stiffness control was less evolved at the start of our research. This is why we have progressively introduced compliant pneumatic control laws and, by the way, widened the variety of actuation solutions for haptic interfaces. At first, in 2013, Abry et al. introduced in [4] a control law to handle the global closed loop compliance of a pneumatic cylinder using a backstepping approach. In this case, high frequency disturbances are absorbed by the natural compliance of the pressurized chambers while the control loop adjusts its stiffness. Starting from these works, Senac et al. designed a syringe simulator [39] and Herzig et al. extended the initial model to introduce a two degrees-of-freedom (DOF) pneumatic robot [19].
Several applications have been designed, based on these works. Concerning haptic medical training, we designed a birth simulator (introduced in Sect. 3.1), an epidural needle insertion simulator (see Sect. 3.2) and we are working on a needle insertion under ultrasonography simulator (not introduced in this paper as this work is in progress [5]). Concerning supporting medical tools, we are also working on an haptic bilateral pneumatic control and remote haptic control of an ultrasonography probe (see Sect. 3.3).
This paper recalls the scientific approaches in the literature about pneumatic actuation in Sect. 2 and illustrates, in Sect. 3, their application in the aforementioned simulators and medical tools.
2 Control Laws for Compliant Pneumatic Actuators
Many robotic applications require an interaction between a human and the end-effector of a robot, for instance, for human rehabilitation, for haptic interfaces, or for prosthetic devices. When these interactions occur, most of the time, a compliant behavior of the robot is required in order to avoid human injuries or to avoid damaging the robot itself. Nevertheless, these robots have also to be stiff for some tasks requiring precision. Haptic interfaces are robots (mechatronic systems) with this kind of properties, in order to interact with a simulated tool in a virtual environment or a teleoperated system. However, in practice, when the interface requires to be realistic (as close as the real tool it simulates), off the shelf haptic interfaces are not always suitable [24]. For practical reasons, in commercial simulators, electric actuators are commonly used, in order to reproduce the force feedback mimicking the response of the human body behavior to medical tool interaction. Indeed, the control laws for electric actuators are quite well mastered and easy to set up. However they have some drawbacks such as a low power to weight ratio and difficulties to provide at the same time a high torque at high speed, and mechanical limitations in their backdrivability. This limits their performances to render a variable stiffness. To ensure a compliant behavior of a robot, various Variable Stiffness Actuators (VSA) or Variable Impedance Actuators (VIA) have been developed during last decades. These actuators allow the equilibrium position and the stiffness to be tuned independently. Van Ham et al. present a state of the art in the design of VSA in [48]. Most of these actuators are designed with two internal motors and passive compliant elements. An advantage of this design is that the control of the the position and stiffness is obtained by controlling the positions of two electric motors. The main drawbacks of this kind of solution are their high cost as two electric actuators are needed to control only one DOF, and their limited stiffness range due to the use of passive stiffness components [21].
Another approach to obtain a compliant behavior for the robots is based on control strategies such as stiffness control [37], impedance control [20] or hybrid force position control [17]. Most of these strategies have been developed for electromechanical actuated robots. The disadvantages of the electromechanical actuation are that, in order to implement these control strategies, a force/torque sensor is needed. This sensor is required to measure the interaction force between the robot and the environment, which implies knowing in advance where this interaction occurs. Moreover, these sensors are often expensive and fragile. When force/torque sensors are not used, the actuators have to be backdrivable which means reducing gear ratios and, consequently, the torque or force range of the robot.
On the opposite side, pneumatic actuators are quite adequate to reproduce human body behavior as they provide a natural compliance thanks to the air compressibility in their chambers. They are commonly used as bi-stable position actuators but they also can be considered as Variable Stiffness Actuators (VSA) as their stiffness can be tuned by modifying the pressure in both chambers so that they can instantaneously react to stimuli without requiring a fast control loop. Unfortunately, their control is more complex than electric actuators as the air compressibility induces non-linear behaviors. The recent development of servovalves and modern robust non-linear control laws based on sliding mode [47] and backstepping [23] allowed the development of position or force controller. A state of the art in compliant control for pneumatic cylinder is provided in [46], most of them are based on a sliding mode controller and need two proportional servovalves for a single cylinder. Thus, since pneumatic cylinders are inexpensive and have a good power to weight ratio, there has been a recent surge of interest for this technology.
Hereinafter, we present a model of a pneumatic actuator and a control law which objective is to control its stiffness.
2.1 Servo+Cylinder Modeling
Figure 1 shows the actuator often used in our applications: an Airpel\(^{\textregistered }\) (Airpot\(^{\textregistered }\) Corp.). We fit it with sensors (pressure, position, and force) and supply it with air by means of a Festo\(^{\textregistered }\) MPYE-5-M5-010-B proportional servovalve. We usually embed our control laws in a dSPACE\(^{\textregistered }\) 1104 control board which acquires in real time sensor signals and generates the servovalve control signals. The code is generated with Matlab/Simulink\(^{\textregistered }\) which is suitable for control prototyping. A schematic of the whole architecture is shown in Fig. 2.

Airpel M16D100D model

Electropneumatic system
The actuator model can be obtained using two physical laws: the pressure dynamics of the chambers and the fundamental mechanical relation. The pressure evaluation of the chambers with variable volumes is obtained with the following assumptions [6]:
-
air is a perfect gas and its kinetic energy is negligible in the chamber,
-
the pressure and the temperature are homogeneous in each chamber,
-
the evolution of the gas in each chamber is polytropic and is characterized by coefficient k,
-
the temperature variation in chambers is negligible with respect to the supply temperature,
-
the temperature in each chamber can be considered equal to the supply temperature,
-
the mass flow rate leakages are negligible,
-
the supply and exhaust pressures are constant.
A fourth order state model of the pneumatic actuator can be written:
where the model variables andFootnote 1 parameters are listed in Table 1.
As ultra-low friction pneumatic cylinders are used, the stiction force \(F_{st}\) can be considered as negligible. Concerning servovalve dynamics, it can be neglected compared to the actuator ones. The pneumatic effort \(F_{pneu}\) corresponds to the pressure difference in both chambers: \(F_{pneu}=P_pS_p-P_nS_n\).
Two separate stiffnesses are defined: the closed-loop stiffness \(K_{cl} = - \dfrac{\partial \varSigma F}{\partial y}\) (where \(\varSigma F\) is the sum of every force applied on the cylinder rod), and the pneumatic stiffness, denoted \(K_{pneu} = k \left( \dfrac{P_pS_p}{L_p(y)} + \dfrac{P_nS_n}{L_n(y)} \right) \) (where \(L_p(y)=(\dfrac{l}{2}+y)\) and \(L_n(y)=(\dfrac{l}{2}-y)\)). The closed-loop stiffness denotes the electropneumatic actuator ability to reject a disturbance force, which, in the context of haptic interfaces, corresponds to the force \(F_e\) applied by the user. The pneumatic stiffness is a state of the electropneumatic actuator [40]. It illustrates the global pressurization in both chambers. This state can be controlled in order to optimize air consumption or to reduce air leakage.
We showed in [19] that, instead of controlling each mass flow rate entering each chamber, it is easier to define two virtual flow rates: the active mass flow rate, denoted \(q_{mA}\), and the pressurization mass flow rate \(q_{mT}\), using the reversible “A-T transform”:
2.2 Position and Stiffness Control Based on Backstepping
Position or force control of pneumatic cylinders is well mastered nowadays in the fluid power community, as detailed in [7, 36]. The control law exposed here (see Fig. 3) is based on a non-linear method: backstepping position control synthesis with a gain tuning strategy to control the stiffness [3]. It simultaneously controls both the actuator position and the pneumatic stiffness (it can also be used to control the actuator closed-loop stiffness [4]). A significant advantage of this control law is the use of only one servovalve per cylinder, in comparison to other ones which require two of them. The performance of this control law has been successfully compared in [18] with a “classical” impedance control law introduced in [27]. Controlling this stiffness allows to simulate different human organ behaviors such as rigid ones (bones) and soft ones (kidney ...). Indeed, most of the soft tissues in biomedical field are modeled with non constant or nonlinear stiffness, this is why real time tuning the closed-loop stiffness of the haptic simulators is needed. These controllers are also suitable for a medical simulator when the haptic interface is linked to a complex simulation model with numerous deformable objects. Indeed, in this specific case, the simulation software which has to compute the reference forces (or/and position) for the haptic interface, needs time to converge and cannot compute at a sufficiently high rate for an haptic control.

Backstepping position control scheme
The state model of the cylinder introduced in (1) can be modified to include \(F_{pneu}\) and \(K_{pneu}\). A new state model can thus be written as:
where \(A_1 = 2(k+1)\), \(A_2=k(k+1),\) \(B_1=\dfrac{2krT_a}{l}\), \(B_2=\dfrac{2k^2rT_a}{l}\) and \(B_3=k^2rT_a\)
The backstepping control law provides the two desired virtual flow rates \(q_{mA}\) and \(q_{mT}\) and ensures the system stability. \(q_{mA}\) allows to track a desired position \(y_d\) whereas \(q_{mT}\) allows to track a desired pneumatic stiffness evolution \(K_{pneud}\). The expressions of \(q_{mA}\) and \(q_{mT}\) derived from the backstepping method are detailed in [18].
2.3 Experimental Results
Figure 4 shows the results of an experiment performed with the aforementioned controller. Figure 4a shows the disturbance force applied on the cylinder rod (in blue) and the values of the desired closed-loop stiffness (in red). Figure 5b shows the actuator response to these disturbances where \(y_d\) is the constant desired position, y is the measured position and \(y_k=y_d+\dfrac{F_e}{K_{cl}}\) is computed to show the expected position of the cylinder when a disturbance is applied. One can observe a good tracking between y and \(y_k\) which means that the system reacts correctly to a position and stiffness references whatever disturbance. Experiments with a moving position reference have also been successfully performed. It demonstrates that it is possible to realize an actuator tracking a desired position which stiffness is tunable in real time.

Closed-loop stiffness tuning with the backstepping position controller (Color figure online)
We extended this strategy to multiple DOF systems in [19]. We applied it on a two-active-DOF pneumatic robot which is a part of the haptic interface embedded in the childbirth simulator presented in Sect. 3.1. In [19], the response to an external disturbance force and a strategy to ensure a desired closed-loop stiffness by tuning some gains are discussed. Simulation results and a comparison with a classical linear impedance controller without force sensor illustrate the interest of this approach.
3 Applications
This section illustrates how compliant pneumatic actuators are applied into medical tools and simulators.
3.1 Birthsim: A Simulator to Train on Difficult Childbirths
Since 2004, in order to train students in obstetrics and midwives, particularly for difficult childbirths, scientists have been proposing simulators more evolved than traditional passive manikins. For instance Lapeer et al. chose to develop an augmented environment to simulate obstetric forceps delivery [26]. Their simulator enables users to visualize their instruments inside the maternal pelvis. There is however no haptic interface to train on forceps extraction. Sielhorst et al. [41] and Abate et al. [1] have worked on delivery simulators coupling augmented reality with an haptic interface. The first one is based on a 6 DOF industrial robot to control the head trajectory. This kind of robot is easy to use but the range of the available forces is oversized for this kind of application. The second one uses an industrial exoskeleton haptic device, coupled with virtual reality goggles, which allows a perfect immersion of users and a good haptic feedback. However, as the user is the only one person immersed in the simulation, it is not appropriate for a team work practice. Some simulators are commercially available and one of the most advanced is the NOELLE simulator [12]. It is dedicated to team training but it is not adapted to evaluate a practitioner specific gestures.
During the past few years, Ampère laboratory has developed a childbirth simulator (called BirthSim) [42] which compensates for the limitations of existing ones. It has been designed especially to train and evaluate the instrumental delivery gestures. It consists of anthropomorphic models of maternal pelvis and fetal head. Obstetrics forceps are instrumented to measure their displacements [31]. Several scenarios have been implemented on the BirthSim simulator. Trainees can thus proceed to a risk free training on forceps blade placement and forceps extraction. A visualization interface is also available to let the trainee to see inside the pelvis and improve his gestures while using forceps.
The BirthSIM simulator now has two pneumatic actuated DOFs (cylinders 1 and 2 in Fig. 5a) to render the translation of the head of the fetus in the vertical symmetry plane and the efforts involved during deliveries. The rotation of the fetal head around the longitudinal axis of cylinder 2 is electrically controlled. A 2 DOF backstepping position control has been implemented, with gain tuning, in order to control the closed-loop stiffness and damping, as introduced earlier. Details and experimental results are available in [19].

BirthSim: difficult chilbirth haptic simulator
3.2 Perisim: Epidural Needle Insertion Simulator
Epidural anaesthesia, despite being a commonly used medical gesture performed mainly during childbirth delivery, remains a very complex and hard to learn gesture [25]. This is mainly due to the fact that the procedure is mostly performed blindly, relying solely on haptic cues and their interpretation by the anaesthetist. To perform such a gesture, the practitioner has to insert a Tuohy needle between two vertebrae while injecting a fluid using an epidural syringe. To perform the anaesthesia, the Tuohy needle has to go through several physical layers to finally reach the epidural space. Throughout the insertion, the anaesthetist experiences an increasing resistance coming both from the needle insertion and from fluid injection. This resistance reaches its maximum in the ligamentum flavum to then plummet creating what is commonly called the loss of resistance principle. It is this principle that allows physicists to know they reached the epidural space. Due to the relatively high forces exerted simultaneously on the needle and on the plunger of the syringe, the procedure is really demanding in term of precision as the epidural space is usually only about 4 mm wide. In consequence, this particular medical gesture has a quite steep learning curve and may require up to 90 attempts to be performed with only 80% efficiency [49], which cannot be enough for healthcare applications.
Some training support solutions have been developed in the form of manikins or complete robotic applications. Most of the proposed solutions have been listed and compared in [49], which considers 17 manikin based solutions and 14 computer based ones. According to this study, there existed no any ideal solution. Out of computer based solutions, we can highlight, for instance, the works of Manoharan et al. [29], Magill et al. [28], Dubey et al. [13] or Thao et al. [45], who introduced haptic simulators for this particular procedure. These simulators however, provide an incomplete representation of epidural anaesthesia. Concerning needle insertion, these solutions often developed a custom haptic interface to generate the necessary haptic cues but the only included simplified representation of the procedure, limited, for example, in terms of degrees of freedom or ignoring potential bone contacts. Regarding the loss of resistance, the simulations are very simplified (if present), only using on/off solenoid valves.
Vaughan et al. [49] have drawn some outlines as to what would be the perfect epidural needle insertion simulator. It has to be customisable (to represent various patient types) and should provide a haptic interface for the syringe manipulation (with the LOR feel), paired with a 3D interface for the needle insertion. However, most of the current simulation options are only able to reproduce what is called 100% (binary) loss of resistance behavior, which is encountered only in the “average” and “easy” cases. The difficult cases require a continuous feedback with a specific force feedback pattern.
Therefore, we designed an haptic simulator able to reproduce the rendering of the loss of resistance experience with a generic haptic interface paired with a pneumatic cylinder. In this simulator, the electric haptic interface (a Virtuose™6D from Haption) is here to reproduce the haptic cues generated by the needle insertion only. The pneumatic cylinder (an Airpel Anti Stiction\(^{\textregistered }\) double acting pneumatic cylinder), mounted on the effector of the Virtuose, is employed to emulate the syringe used in the real application and its purpose is to emulate the loss of resistance. The whole is visible in Fig. 6 (the Virtuose is partly hidden under the green cover, and the syringe simulation part is depicted in the right picture).

Complete prototype setup (left) and Pneumatic cylinder setup (right)
To tune accurately enough the prototype, we asked trained anaesthetists to try and assess it. It allowed us to apply some necessary adjustments to some simulation parameters, such as the values of the the resistant force created by the pneumatic cylinder. Once the parameters were set to obtain realistic simulations, we recorded complete procedures. The aim of the first experimental study was to know whether it would be possible to differentiate an experienced user from a novice through the use of this simulator.
We set up three kinds of patients for the first test sessions. The first patient type was the average patient, which represents an “easy” case and serves as a basis from which we derived the others. The parameters changed for the other patient types were: the length of the derma layer, the length of the epidural space layer, and the LOR speed (i.e. the speed of transition between the highest resistant force in the ligamentum flavum to the lowest in the epidural space). The patient characteristics are available in [39].
The tests were performed with 2 experts and 6 novices. Up to 24 variables were simultaneously recorded. Details results are available in [39]. On initial examination, we analyzed the success rate per patient type, the velocity of the needle tip along the insertion path. Finally we proposed an indicator computed by dividing the proportion of emptied syringe by the distance d traveled by the haptic interface from the puncture of the derma to the end of the procedure along the elastic plane normal vector. Only the unskilled users failed some attempts. The overall results show that novices obtain a success rate of 60% (versus 100% for the experts). Their success rate is better for the calcified/average cases and worse for the overweight ones. This indicates that the LOR phenomenon reproduction played an important role in how the unskilled users detected the epidural space. This confirmed the need for a customizable LOR rendering instead of a binary LOR behavior. Also, regarding the aforementioned indicator, the experts tend to have a much higher score than the novices, showing that they usually use a greater portion of the cylinder length (d being constant regardless of the patient type). This might be a way for the skilled users to retrieve as much haptic information as possible. This may help them knowing their current position with much more precision than only detecting the LOR. Furthermore, concerning the novices, the standard deviation of the indicator is also quite high showing a wide variety of use.
As a conclusion, the overall results of this first study are quite encouraging and indicate that such a simulator might be realistic enough to provide an efficient training tool in the future. However some points might need more work such as introducing a very distinct feel of cutting through the ligamentum flavum which, according to our experts, feels like friction and cracklings. Moreover, according to their feedback, when the needle is in the ligamentum flavum, the syringe plunger should give the impression that it is locked. Finally, we are preparing an automatic classification of the users method in order to provide rapid, objective and automatic user assessment. This requires more trials with more users in order to generate a representative training data set. We will also assess the relevancy of such a tool in a teaching environment.
3.3 Remote Ultrasonography Haptic Master
Nowadays, more than one out of four emergency admissions requires an ultrasound examination. This non-radiative and relatively low-cost imaging technique is routinely used to help physicians to deliver a preliminary diagnosis. Depending on state health policies, an ultrasound imaging diagnosis is performed either by trained physicians or by specialized sonographers. In both cases, the physician/sonographer must be close to the patient to maintain and hold the ultrasound probe on the designated anatomic area to perform the examination. The sonographer integrates the position of the probe and the motion of his hand to analyze the resulting 2D ultrasound images. Since the late 1990 s, in order to deliver equitable healthcare in medically isolated settings, several concepts of remote robotized ultrasonography have been developed, giving the sonographer the ability to move an ultrasound probe on a distant patient [10, 14]. TER [53] or Masuda [30] used fixed robots attached to a table. Current trends are light body-mounted robots [33, 34]: a paramedic holds the robot on the patient body while the distant sonographer controls the probe orientation using a dedicated input device, as in Fig. 7.
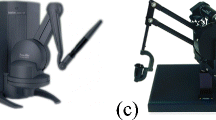
Ergonomics is a critical requirement as the sonographers should not be disturbed by the distance with their patient in order to only focus on the medical procedure. Hence, master devices have to provide sonographers with full transparency to perform a robotized remote ultrasound scanning as if they were next to the patient. The master device must be adapted to the sonographer’s hand and to his/her expertise. It is possible to use off-the-shelf 3D haptic interfaces, but their kinematic chain is totally different from the one offered by the standalone ultrasound probes sonographers are used to. This means that the practitioner has to adapt his/her hand motions to the proposed input devices, which therefore disturbs the medical act. We proposed in [11] to provide the sonographer with a master ultrasound probe with no mechanical link with the environment, similar to a standard ultrasound probe. The tele-echography device was developed by Prisme laboratory (see Fig. 8) and industrialized under patent in the AdEchoTech company. The system is divided into two parts: a slave robot on the patient side and a hand-free probe replica on the sonographer side without any mechanical connection between the two. A TCP/IP connection links the two parts.

Remote echography.

Adechotech melody system.
With the haptic master probe concept, trained doctors or specialized sonographers should need less training to control the distant robot [50], as when performing an ultrasound examination, sonographers need to feel the interaction between the probe and the patient’s body. Indeed, they need to feel when they touch hard body parts and when the body-probe interaction stiffness changes. This is even more true at distance as the practitioner does not have a direct view of the patient (only through a web camera). The master probe should thus be actuated to render the interaction forces (and stiffness) between the real remote ultrasound probe and the patient’s body. Even if it concerns only one dimension, this force-feedback is a real ergonomic and technological challenge: it is important to preserve weight and dimensions comparable to standard ultrasound probes. During first experiments with sonographers, we identified the following requirements, which correspond to classical dimensions of ultrasonography probes and measures performed on our first prototype:
-
a reversible mechanism with small dimensions (12 cm long, 6.5 cm wide and 3.5 cm thick at most),
-
in the z direction (orthogonal to the patient’s skin), a continuous force feedback level around 15 N,
-
a maximum force of 25 N, a stroke of 50 mm, with a maximum velocity of 200 mm/s.
We enhanced the aforementioned Melody robot by replacing the electric motor which performs the longitudinal (z) real probe motion by a linear motor, in order to ensure the reversibility of this motion. Moreover we added a force sensor which measures the reactive force of the patient’s body on the ultrasound probe. On the sonographer’s side, we first designed electrically actuated probe replicas, which could not fit as aforementioned. Neither a DC-motor [32], nor a custom brushless motor [9], nor a linear motor [52] were able to meet the requirements: without any reduction, electric motors cannot deliver a such desired force-feedback –without motion– in so tiny a (hand held) volume. This is why we proposed to use a pneumatic cylinder as internal VSA for the fake probe, introduced in a bilateral control scheme (proposed earlier in [51]), to remotely control the robot which holds the real ultrasound probe. Figure 9 displays the pneumatic haptic probe we designed. The whole probe measures 120 mm high, 65 mm wide and 35 mm deep, and weighs 240 g. It is bulky compared to modern ultrasonography probes. Nevertheless, this prototype was designed for the purposes of a feasibility study. Hence off-the-shelf low-priced components have been preferred over ergonomic constraints. Future designs will take ergonomics into account more comprehensively. Design details, first basic control approaches and experiment results are provided in [2]. They demonstrate the feasibility of a pneumatic actuation to provide haptic feedback for this kind of application, and highlight the need for a more evolved control law such as the one exposed in Sect. 2.2. Future experimentations featuring the whole teleoperation loop will be held to evaluate the overall quality of the whole system. Also, these results will be accompanied by a psychometric study determining whether users are able to recognize common medical cases.

Haptic pneumatic probe (with the rod completely in (top picture) and out (bottom picture).
4 Conclusion
In this paper, we illustrated the use of pneumatic actuators for medical applications. We recalled the properties of such actuators versus classical electric ones, and highlighted their interest for rendering haptic feedback, when controlled with advanced nonlinear control laws such as the one depicted in Sect. 2.2, in order to make them act as Variable Stiffness Actuators. We then presented several applications we have been working on, based on this approach: the childbirth simulator (birthSim), the epidural needle insertion simulator (periSim) and the haptic master probe for remote ultrasonography. The latter simulator is pneumatic based only, while the two others are hybrid: electric and pneumatic (birthSim and periSim). They all highlight the interest of such an approach, especially when the size and form constraints limit the feasibility of electric solutions.
Aside from Birthsim, these applications are in progress. The more advanced one is periSim as we are getting enough data to propose an effective and objective assessment method. The ultrasonography master probe requires further developments (such as the use of aforementioned nonlinear control law) and experiments in a teleoperation context to validate its effectiveness. We are also working on an intra-articular injection (it is one of the most used method by the rheumatologists to treat the shoulder pain) under ultrasonography simulator which will also use hybrid actuation. First results about the electric part are available in [5].
Notes
- 1.
It has to be noticed that this model is available also for a single rod cylinder. In the case of a double rod cylinder, \(S_p=S_n=S\) so \(F_{pext}=0\).
References
Abate, A.F., Acampora, G., Loia, V., Ricciardi, S., Vasilakos, A.V.: A pervasive visual-haptic framework for virtual delivery training. IEEE Trans. Inf. Technol. Biomed. 14(2), 326–334 (2010)
Abdallah, I., Gatwaza, F., Morette, N., Lelevé, A., Novales, C., Nouaille, L., Brun, X., Vieyres, P.: A pneumatic haptic probe replica for tele-robotized ultrasonography. In: Basu, A., Berretti, S. (eds.) ICSM 2018. LNCS, vol. 11010, pp. 79–89. Springer, Cham (2018). https://doi.org/10.1007/978-3-030-04375-9_7
Abry, F., Brun, X., Sesmat, S., Bideaux, E., Ducat, C.: Electropneumatic cylinder backstepping position controller design with real-time closed-loop stiffness and damping tuning. IEEE Trans. Control. Syst. Technol. 24(2), 541–552 (2016)
Abry, F., Brun, X., Sesmat, S., Bideaux, E.: Non-linear position control of a pneumatic actuator with closed-loop stiffness and damping tuning. In: Proceedings of the European Control Conference 2013 (2013)
Ma de los Angeles Alamilla, D., Moreau, R., Redarce, T.: A new method to render virtual walls for haptic systems: “tracking wall”. In: Proceedings of the: 7th International Conference on Mechatronics and Control Engineering (ICMCE 2018), Netherlands, Amsterdam (2018)
Andersen, B.W.: The Analysis and Design of Pneumatic Systems. Wiley, Hoboken (1967)
Carneiro, J.F., de Almeida, F.G.: Using two servovalves to improve pneumatic force control in industrial cylinders. Int. J. Adv. Manuf. Technol. 66(1–4), 283–301 (2013)
Cestari, M., Sanz-Merodio, D., Arevalo, J.C., Garcia, E.: Ares, a variable stiffness actuator with embedded force sensor for the atlas exoskeleton. Ind. Robot.: Int. J. 41(6), 518–526 (2014)
Charron, G., et al.: Robotic platform for an interactive tele-echographic system: the PROSIT ANR-2008 project. In: Proceedings of Hamlyn Symposium on Medical Robotics, London, UK (2010)
Conti, F., Park, J., Khatib, O.: Interface design and control strategies for a robot assisted ultrasonic examination system. In: Khatib, O., Kumar, V., Sukhatme, G. (eds.) Experimental Robotics. Springer Tracts in Advanced Robotics, vol. 79. Springer, Heidelberg (2014). https://doi.org/10.1007/978-3-642-28572-1_7
Courreges, F., Novales, C., Poisson, G., Vieyres, P.: Modelisation, commande geometrique et utilisation d’un robot portable de tele-echographie: Teresa. J. Eur. Syst. Autom. JESA 43(1), 165–196 (2009)
Deering, S., Brown, J., Hodor, J., Satin, A.J.: Simulation training and resident performance of singleton vaginal breech delivery. Obstet. Gynecol. 107(1), 86–89 (2006)
Dubey, V., Vaughan, N., Wee, M.Y.K., Isaacs, R.: Biomedical engineering in epidural anaesthesia research. In: Adriano Andrade, editor, Practical Applications in Biomedical Engineering. InTech, January 2013
Gourdon, A., Poignet, P., Poisson, G., Vieyres, P., Marche, P.: A new robotic mechanism for medical application. In: Proceedings of the IEEE/ASME International Conference on Advanced Intelligent Mechatronics (AIM 1999), pp. 33–38 (1999)
Granry, J.-C., Moll, M.-C.: état de l’art (national et international) en matière de pratiques de simulation dans le domaine de la santé. Technical report, Haute Autorité de la Santé (HAS) (2012)
Groothuis, S.S., Rusticelli, G., Zucchelli, A., Stramigioli, S., Carloni, R.: The variable stiffness actuator vsaUT-II: mechanical design, modeling, and identification. IEEE/ASME Trans. Mechatron. 19(2), 589–597 (2014)
Hayati S.: Hybrid position/force control of multi-arm cooperating robots. In: Proceedings of the 1986 IEEE International Conference on Robotics and Automation, vol. 3, pp. 82–89, April 1986
Herzig, N., Moreau, R., Leleve, A., Pham, M.T.: Stiffness control of pneumatic actuators to simulate human tissues behavior on medical haptic simulators. In: 2016 IEEE International Conference on Advanced Intelligent Mechatronics (AIM), pp. 1591–1597, July 2016
Herzig, N., Moreau, R., Redarce, T., Abry, F., Brun, X.: Nonlinear position and stiffness backstepping controller for a two degrees of freedom pneumatic robot. Control. Eng. Pract. 73, 26–39 (2018)
Hogan, N.: Stable execution of contact tasks using impedance control. In: Proceedings of the 1987 IEEE International Conference on Robotics and Automation, vol. 4, pp. 1047–1054, March 1987
Huang, Y., Vanderborght, B., Van Ham, R., Wang, Q., Van Damme, M., Xie, G., Lefeber, D.: Step length and velocity control of a dynamic bipedal walking robot with adaptable compliant joints. IEEE/ASME Trans. Mechatron. 18(2), 598–611 (2013)
Jafari, A., Tsagarakis, N.G., Sardellitti, I., Caldwell, D.G.: A new actuator with adjustable stiffness based on a variable ratio lever mechanism. IEEE/ASME Trans. Mechatron. 19(1), 55–63 (2014)
Khalil, H.K.: Nonlinear Systems I. Prentice Hall, Upper Saddle River (2002)
Kheddar, A., Devine, C., Brunel, M., Duriez, C., Sibony, O.: Preliminary design of a childbirth simulator haptic feedback. In: Proceedings of the IEEE Intelligent Robots and Systems Conference, vol. 4, pp. 3270–3275. IEEE (2004)
Konrad, C., Schupfer, G., Wietlisbach, M., Gerber, H.: Learning manual skills in anesthesiology: is there a recommended number of cases for anesthetic procedures? Anesth. Analg. 86(3), 635 (1998)
Lapeer, R.J., Chen, M.S., Villagrana, J.G.: Simulating obstetric forceps delivery in an augmented environment. In: Proceedings of AMI/ARCS Sattelite Workshop of MICCAI 2004, pp. 1–10 (2004)
Liu, H., Hirzinger, G.: Joint torque based Cartesian impedance control for the DLR hand. In: Proceedings of the IEEE/ASME International Conference on Advanced Intelligent Mechatronics, pp. 695–700 (1999)
Magill, J.C., Byl, M.F., Hinds, M.F., Agassounon, W., Pratt, S.D., Hess, P.E.: A novel actuator for simulation of epidural anesthesia and other needle insertion procedures. Simul. Healthc.: J. Soc. Simul. Healthc. 5(3), 179–184 (2010)
Manoharan, V., van Gerwen, D., van den Dobbelsteen, J.J., Dankelman, J.: Design and validation of an epidural needle insertion simulator with haptic feedback for training resident anaesthesiologists. In: 2012 IEEE Haptics Symposium (HAPTICS), pp. 341–348. IEEE (2012)
Masuda, K., Kimura, E., Tateishi, N., Ishihara, K.: Three dimensional motion mechanism of ultrasound probe and its application for tele-echography system. In: Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems, vol. 2, pp. 1112–1116 (2001)
Moreau, R., Pham, M.T., Silveira, R., Redarce, T., Brun, X., Dupuis, O.: Design of a new instrumented forceps: application to safe obstetrical forceps blade placement. IEEE Trans. Biomed. Eng. 54(7), 1280–1290 (2007)
Mourioux, G., Novales, C., Smith-Guerin, N., Vieyres, P., Poisson, G.: A free haptic device for tele-echography. In: Proceedings of International Workshop on Research and Education in Mechatronics (REM 2005), Annecy, June 2005
Najafi, F., Sepehri, N.: A novel hand-controller for remote ultrasound imaging. Mechatronics 18(10), 578–590 (2008)
Nouaille, L., Vieyres, P., Poisson, G.: Process of optimisation for a 4 DOF tele-echography robot. Robotica 30, 1131–1145 (2012)
Panait, L., Akkary, E., Bell, R.L., Roberts, K.E., Dudrick, S.J., Duffy, A.J.: The role of haptic feedback in laparoscopic simulation training. J. Surg. Res. 156(2), 312–316 (2009)
Rahman, R.A., He, L., Sepehri, N.: Design and experimental study of a dynamical adaptive backstepping-sliding mode control scheme for position tracking and regulating of a low-cost pneumatic cylinder. Int. J. Robust Nonlinear Control 26(4), 853–875 (2016)
Salisbury, J.K.: Active stiffness control of a manipulator in Cartesian coordinates. In: 1980 19th IEEE Conference on Decision and Control including the Symposium on Adaptive Processes, pp. 95–100, December 1980
Semini, C., Tsagarakis, N.G., Guglielmino, E., Focchi, M., Cannella, F., Caldwell, D.G.: Design of HyQ - a hydraulically and electrically actuated quadruped robot. Proc. Inst. Mech. Eng. Part I: J Syst. Control Eng. 225, 831–849 (2011)
Senac, T., Lelevé, A., Moreau, R.: Control laws for pneumatic cylinder in order to emulate the loss of resistance principle. In: IFAC 2017 World Congress, Proceedings of the 20th World Congress of the International Federation of Automatic Control, Toulouse, France. IFAC, IFAC, July 2017
Shen, X.R., Goldfarb, M.: Simultaneous force and stiffness control of a pneumatic actuator. J. Dyn. Syst. Meas. Control.-Trans. 129(4), 425–434 (2007)
Sielhorst, T., Blum, T., Navab, N.: Synchronizing 3D movements for quantitative comparison and simultaneous visualization of actions. In: Proceedings of the 4th IEEE/ACM International Symposium on Mixed and Augmented Reality, ISMAR 2005, pp. 38–47. IEEE Computer Society, Washington, DC (2005)
Silveira, R., Pham, M.T., Redarce, T., Betemps, M., Dupuis, O.: A new mechanical birth simulator: Birthsim. In: 2004 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS) (IEEE Cat. No. 04CH37566), vol. 4, pp. 3948–353, September 2004
Sutherland, C., Hashtrudi-Zaad, K., Sellens, R., Abolmaesumi, P., Mousavi, P.: An augmented reality haptic training simulator for spinal needle procedures. IEEE Trans. Biomed. Eng. 60(11), 3009–3018 (2013)
Takaiwa, M., Noritsugu, T.: Development of pneumatic human interface and its application for compliance display. In: Proceedings of 26th Annual Conference of the IEEE Industrial Electronics Society (IECON 2000), vol. 2, pp. 806–811 (2000)
Dang, T., Annaswamy, T.M., Srinivasan, M.A.: Development and evaluation of an epidural injection simulator with force feedback for medical training. Stud. Health Technol. Inform. 81, 97–102 (2001)
Toedtheide, A., Lilge, T., Haddadin, S.: Antagonistic impedance control for pneumatically actuated robot joints. IEEE Robot. Autom. Lett. 1(1), 161–168 (2016)
Utkin, V., Guldner, J., Shi, J.: Sliding Mode Control in Electro-Mechanical Systems. Taylor and Francis, Milton Park (2009)
Van Ham, R., Sugar, T.G., Vanderborght, B., Hollander, K.W., Lefeber, D.: Compliant actuator designs. IEEE Robot. Autom. Mag. 16(3), 81–94 (2009)
Vaughan, N., Dubey, N., Venketesh, M.Y., Wee, K., Isaacs, R.: A review of epidural simulators: where are we today ? Med. Eng. Phys. 35(9), 1235–1250 (2013)
Vieyres, P., et al.: The next challenge for WOrld wide robotized tele-echography experiment (WORTEX 2012): From engineering success to healthcare delivery. In: Proceedings of TUMI II, Congreso Peruano de Ingeniera Biomedical Bioingeniera, Biotecnologica y Fisica Medica, Lima, Peru, May 2013
Vieyres, P., Poisson, G., Courreges, F., Smith-Guerin, N., Novales, C., Arbeille, P.: A tele-operated robotic system for mobile tele-echography: the otelo project. In: Istepanian, R.S.H., Laxminarayan, S., Pattichis, C.S. (eds.) M-Health, Topics in Biomedical Engineering, pp. 461–473. Springer, Heidelberg (2006). https://doi.org/10.1007/0-387-26559-7_35
Vieyres, P., et al.: An anticipative control approach and interactive GUI to enhance the rendering of the distal robot interaction with its environment during robotized tele-echography: Interactive platform for robotized tele-echography. Int. J. Monit. Surveill. Technol. Res. 1(3), 1–19 (2013)
Vilchis Gonzales, A., et al.: TER: a system for robotic tele-echography. In: Niessen, W.J., Viergever, M.A. (eds.) MICCAI 2001. LNCS, vol. 2208, pp. 326–334. Springer, Heidelberg (2001). https://doi.org/10.1007/3-540-45468-3_39
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this paper

Cite this paper
Sénac, T. et al. (2019). Introducing Pneumatic Actuators in Haptic Training Simulators and Medical Tools. In: Antona, M., Stephanidis, C. (eds) Universal Access in Human-Computer Interaction. Multimodality and Assistive Environments. HCII 2019. Lecture Notes in Computer Science(), vol 11573. Springer, Cham. https://doi.org/10.1007/978-3-030-23563-5_27
Download citation
DOI: https://doi.org/10.1007/978-3-030-23563-5_27
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-23562-8
Online ISBN: 978-3-030-23563-5
eBook Packages: Computer ScienceComputer Science (R0)