
Abstract
Background
Prophylactic central neck dissection (pCND) at the time of the total thyroidectomy (TT) remains controversial in clinically nodal-negative (cN0) papillary thyroid carcinoma. Our study was designed to examine the predictive factors and pattern of locoregional recurrence (LRR) after pCND in the context of the postoperative stimulated Tg (sTg) level.
Methods
A total of 341 patients who underwent TT and unilateral pCND were analyzed. Patients with an identifiable lesion on ultrasonography or whole-body scan within 6 months of surgery were excluded. LRR was defined as an identifiable lesion on USG, which was later confirmed by cytology/histology. Preablation sTg level was taken 2 months after surgery, whereas postablation sTg level was taken 8 months after surgery. Cox regression was used in the univariate and multivariate analyses to identify significant independent factors for LRR.
Results
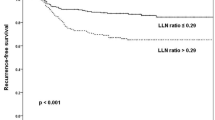
After a follow-up of 66.6 ± 38.6 months, 14 (4.1 %) suffered from LRR. The duration to first LRR was 36.4 ± 21.7 months. The estimated 5- and 10-year LRR rates were 5.1 and 6.1 %, respectively. Of these 14 LRR, 3 (21.4 %) involved the central compartment alone, 9 (64.3 %) involved the lateral compartment alone, and 2 (14.3 %) involved both central and lateral compartments. After adjusting for other clinicopathological factors, postablation sTg level ≥ 1 µg/L (hazard ratio 265.109, 95 % confidence interval 1.132–62075.644, p = 0.045) was the only independent predictor of LRR.
Conclusions
Annualized risk of LRR after pCND was approximately 1 % in the first 5 years and 0.2 % in the subsequent 5 years. Most (78.6 %) LRRs involved the lateral compartment. Postablation sTg ≥ 1 µg/L significantly predicted risk of LRR.

Similar content being viewed by others


Refereneces
SEER Cancer Statistics Review, 1975–2010. National Cancer Institute Surveillance Epidemiology and End Results. http://seer.cancer.gov/csr/1975_2010/. Assessed 29 Jun 2013.
Cancer incidence and mortality in Hong Kong 1983–2009. Hong Kong Cancer Registry, Hong Kong. http://www3.ha.org.hk/cancereg/e_stat.asp. Accessed 15 Feb 2013.
Lang B, Lo CY, Chan WF, Lam KY, Wan KY. Restaging of differentiated thyroid carcinoma by the sixth edition AJCC/UICC TNM staging system: stage migration and predictability. Ann Surg Oncol. 2007;14(5):1551–9.
Machens A, Hauptmann S, Dralle H. Lymph node dissection in the lateral neck for completion in central node-positive papillary thyroid cancer. Surgery. 2009;145:176–81.
Hwang HS, Orloff LA. Efficacy of preoperative neck ultrasound in the detection of cervical lymph node metastasis from thyroid cancer. Laryngoscope. 2011;121(3):487–91.
Roh JL, Park JY, Kim JM, Song CJ. Use of preoperative ultrasonography as guidance for neck dissection in patients with papillary thyroid carcinoma. J Surg Oncol. 2009;99(1):28–31.
Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–214.
Lang BH, Ng SH, Lau L, Cowling B, Wong KP, Wan KY. A systematic review and meta-analysis of prophylactic central neck dissection on short-term locoregional recurrence in papillary thyroid carcinoma after total thyroidectomy. Thyroid. 2013;23:1087–98.
Lang BH, Wong CK. A cost-minimization analysis comparing total thyroidectomy alone and total thyroidectomy with prophylactic central neck dissection in clinically nodal negative papillary thyroid carcinoma. Ann Surg Oncol. 2014;21(2):416–25.
Ryu IS, Song CI, Choi SH, Roh JL, Nam SY, Kim SY. Lymph node ratio of the central compartment is a significant predictor for locoregional recurrence after prophylactic central neck dissection in patients with thyroid papillary carcinoma. Ann Surg Oncol. 2014;21(1):277–83.
Barczyński M, Konturek A, Stopa M, Nowak W. Nodal recurrence in the lateral neck after total thyroidectomy with prophylactic central neck dissection for papillary thyroid cancer. Langenbecks Arch Surg. 2014;399(2):237–44.
Jeon MJ, Kim WG, Park WR, et al. Modified dynamic risk stratification for predicting recurrence using the response to initial therapy in patients with differentiated thyroid carcinoma. Eur J Endocrinol. 2013;170(1):23–30.
Kim TY, Kim WB, Kim ES, et al. Serum thyroglobulin levels at the time of 131I remnant ablation just after thyroidectomy are useful for early prediction of clinical recurrence in low-risk patients with differentiated thyroid carcinoma. J Clin Endocrinol Metab. 2005;90:1440–5.
Heemstra KA, Liu YY, Stokkel M, et al. Serum thyroglobulin concentrations predict disease-free remission and death in differentiated thyroid carcinoma. Clin Endocrinol (Oxf.). 2007;66:58-64.
Giovanella L, Ceriani L, Suriano S, Ghelfo A, Maffioli M. Thyroglobulin measurement before rh-TSH-aided 131I ablation in detecting metastases form differentiated thyroid carcinoma. Clin Endocrinol (Oxf.). 2008;69:659–63.
Lang BH, Chow SM, Lo CY, Law SC, Lam KY. Staging systems for papillary thyroid carcinoma: a study of 2 tertiary referral centers. Ann Surg. 2007;246(1):114–21.
Wong H, Wong KP, Yau T, Tang V, Leung R, Chiu J, Lang BH. Is there a role for unstimulated thyroglobulin velocity in predicting recurrence in papillary thyroid carcinoma patients with detectable thyroglobulin after radioiodine ablation? Ann Surg Oncol. 2012;19(11):3479–85.
Chan WF, Lang BH, Lo CY. The role of intraoperative neuromonitoring of recurrent laryngeal nerve during thyroidectomy: a comparative study on 1000 nerves at risk. Surgery. 2006;140:866–73.
Barczyński M, Konturek A, Stopa M, Nowak W. Prophylactic central neck dissection for papillary thyroid cancer. Br J Surg. 2013;100(3):410–8.
Kruijff S, Petersen JF, Chen P, et al. Patterns of structural recurrence in papillary thyroid cancer. World J Surg. 2014;38(3):653–9.
Hartl DM, Leboulleux S, Al Ghuzlan A, Baudin E, Chami L, Schlumberger M, Travagli JP. Optimization of staging of the neck with prophylactic central and lateral neck dissection for papillary thyroid carcinoma. Ann Surg. 2012;255(4):777–83.
Sancho JJ, Lennard TW, Paunovic I, Triponez F, Sitges-Serra A. Prophylactic central neck dissection in papillary thyroid cancer: a consensus report of the European Society of Endocrine Surgeons (ESES). Langenbecks Arch Surg. 2014;399(2):155–63.
Tuttle RM, Tala H, Shah J, et al. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. 2010;20(12):1341–9.
Castagna MG, Maino F, Cipri C, et al. Delayed risk stratification, to include the response to initial treatment (surgery and radioiodine ablation), has better outcome predictivity in differentiated thyroid cancer patients. Eur J Endocrinol. 2011;165(3):441–6.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lang, B.HH., Chan, D.T.Y., Wong, K.P. et al. Predictive Factors and Pattern of Locoregional Recurrence After Prophylactic Central Neck Dissection in Papillary Thyroid Carcinoma. Ann Surg Oncol 21, 4181–4187 (2014). https://doi.org/10.1245/s10434-014-3872-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-3872-6