
Abstract
Introduction
The ACOSOG Z0011 trial has been described as practice-changing. The goal of this study was to determine the impact of the trial on surgeon practice patterns at our institution.
Methods
This is a review of practice patterns comparing the year before release of Z0011 to the year after an institutional multidisciplinary meeting discussing the results. Patients meeting Z0011 inclusion criteria were identified. Clinicopathologic data were compared between the cohorts.
Results
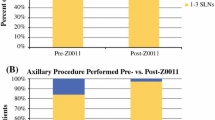
There were 658 patients with clinical T1-2 tumors planned for breast conservation: 335 in the pre-Z0011 cohort and 323 post-Z0011. Sixty-two (19 %) patients were sentinel lymph node (SLN) positive in the pre-Z0011 group versus 42 (13 %) post-Z0011 (p = 0.06). Before Z0011, 85 % (53/62) of SLN-positive patients underwent axillary node dissection (ALND) versus 24 % (10/42) after Z0011 (p < 0.001). After Z0011, surgeons were more likely to perform ALND on patients with larger tumors (2.2 vs. 1.5 cm, p = 0.09), lobular histology (p = 0.01), fewer SLNs (1 vs. 3, p = 0.09), larger SLN metastasis size (4 vs. 2.5 mm, p = 0.19), extranodal extension present (20 vs. 6 %, p = 0.16), or a higher probability of positive non-SLNs (p = 0.03). Surgeons were less likely to perform intraoperative nodal assessment post-Z0011 (26 vs. 69 %, p < 0.001) resulting in decreased median operative times for SLN-negative patients (79 vs. 92 min, p < 0.001).
Conclusions
Surgeons at our institution have implemented Z0011 results for the majority of patients; however, clinicopathologic factors still impact the decision to perform ALND. Z0011 results have significantly impacted practice by decreasing rates of ALND, use of intraoperative nodal evaluation, and operative times.

Similar content being viewed by others


References
Fisher B, Bauer M, Margolese R, et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med. 1985;312(11):665–73.
Giuliano A, Kirgan D, Guenther J, Morton D. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg. 1994;220(3):391–9.
Giuliano A, Dale P, Turner R, Morton D, Evans S, Krasne D. Improved axillary staging of breast cancer with sentinel lymphadenectomy. Ann Surg. 1995;222(3):394–9.
National Comprehensive Cancer Network (NCCN) Clinical practice guidelines in oncology: breast. version 2.2008; 2008.
Lyman G, Giuliano A, Somerfield M, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol. 2006;24(1):210–1.
Yi M, Giordano S, Meric-Bernstam F, et al. Trends in and outcomes from sentinel lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database. Ann Surg Oncol. 2010;17(Suppl 3).
Bilimoria K, Bentrem D, Hansen N, et al. Comparison of sentinel lymph node biopsy alone and completion axillary lymph node dissection for node-positive breast cancer. J Clin Oncol. 2009;27(18):2946–53.
Hwang R, Gonzalez-Angulo A, Yi M, et al. Low locoregional failure rates in selected breast cancer patients with tumor-positive sentinel lymph nodes who do not undergo completion axillary dissection. Cancer. 2007;110(4):723–30.
Giuliano A, Hunt K, Ballman K, et al. Axillary dissection vs. no axillary dissection in women with invasive breast cancer and sentinel node metastasis. JAMA. 2011;305(6):569–75.
Giuliano A, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg. 2010;252(3):426–32.
Morrow M, Giuliano A. To cut is to cure: can we really apply Z11 in practice? Ann Surg Oncol. 2011;18(9):2413–5.
Caudle A, Hunt K, Kuerer H, et al. Multidisciplinary considerations in the implementation of the findings from the American College of Surgeons Oncology Group (ACOSOG) Z0011 study: a practice-changing trial. Ann Surg Oncol. 2011;19(8):2407–12.
National Comprehensive Cancer Network (NCCN) Clinical practice guidelines in oncology: breast, Version 2011; 2011.
National Comprehensive Cancer Network (NCCN) Clinical practice guidelines in oncology: breast, Version 2012; 2012.
Krishnamurthy S, Sneige N, Bedi D, et al. Role of ultrasound-guided fine-needle aspiration of indeterminate and suspicious axillary lymph nodes in the initial staging of breast carcinoma. Cancer. 2002;95(5):982–8.
Mittendorf E, Hunt K, Boughey J, et al. Incorporation of sentinel lymph node metastasis size into a nomogram predicting nonsentinel lymph node involvement in breast cancer patients with a positive sentinel lymph node. Ann Surg. 2012;255(1):109–15.
Setton J, Cody H, Tan L, et al. Radiation field design and regional control in sentinel lymph node-positive breast cancer patients with omission of axillary dissection. Cancer. 2011.
Haffty B, Hunt K, Harris J, Buchholz T. Positive sentinel nodes without axillary dissection: implications for the radiation oncologist. J Clin Oncol. 2011;29(34):4479–81.
Mittendorf E, Sahin A, Tucker S, et al. Lymphovascular invasion and lobular histology are associated with increased incidence of isolated tumor cells in sentinel lymph nodes from early-stage breast cancer patients. Ann Surg Oncol. 2008;15(12):3369–77.
Kim T, Guiuliano A, Lyman G. Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma: a meta-analysis. Cancer. 2006;106(1):4–16.
Lucci A, McCall L, Beitsch P, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol. 2007;25(24):3657–63.
Shih Y, Xu Y, Cormier J, et al. Incidence, treatment costs, and complications of lymphedema after breast cancer among women of working age: a 2-year follow-up study. J Clin Oncol. 2009;27(12):2007–14.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Caudle, A.S., Hunt, K.K., Tucker, S.L. et al. American College of Surgeons Oncology Group (ACOSOG) Z0011: Impact on Surgeon Practice Patterns. Ann Surg Oncol 19, 3144–3151 (2012). https://doi.org/10.1245/s10434-012-2531-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-012-2531-z