
Abstract
Background
The purpose of this study was to describe clinical characteristics and outcome of mammographically and clinically detected new cancers in patients with previously diagnosed ductal carcinoma in situ (DCIS).
Method
Our database was searched to identify patients with a primary diagnosis of DCIS. Those with prior evidence of invasive carcinoma were excluded from the analysis. Cumulative incidence of new cancers was estimated according to the method of Gray. Survival times were estimated using the Kaplan Meier product limit method.
Results
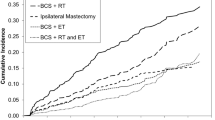
A total of 799 patients diagnosed and treated for DCIS were included in the analysis. Median age at diagnosis was 54 years (range 22–88 years) and median tumor size was 1.4 cm (range 0.2–15 cm). After a median follow-up of 2.9 years, 45 patients (5.6%) had a second event: 14 (31%) with in-situ and 31 (69%) with invasive disease. Median disease-free interval was 3.5 years (range 0.5–20.8 years). The majority of second events (63%) occurred in the opposite breast (P = 0.048) and the cumulative incidence at 5 years was 6.6%. Overall survival at 5 years was 97.4%; that for the second event was 76.1%. For mammography and self-palpation, respectively, the 5-year survival by method of detection of the second event was 63.2% and 100% (P = 0.08 with a 33% power to detect a difference).
Conclusion
Second events following DCIS occurs primarily in the opposite breast and have a negative impact on survival.


Similar content being viewed by others


References
Schnitt SJ, Silen W, Sadowsky N, et al. Ductal carcinoma in situ (intraductal carcinoma of the breast). N Engl J Med 1988; 318:898–903
Miller FR, Soule HD, Tait L, et al. Xenograft model of progressive human proliferative breast disease. J Natl Cancer Inst 1993; 85:1725–1732
Ernster VL, Ballard-Barbash R, Barlow WE, et al. Detection of ductal carcinoma in situ in women undergoing screening mammography. J Natl Cancer Inst 2002; 94:1546–1554
Leonard GD, Swain SM. Ductal carcinoma in situ, complexities and challenges. J Natl Cancer Inst 2004; 96:906–920
Silverstein MJ, Barth A, Poller DN, et al. Ten-year results comparing mastectomy to excision and radiation therapy for ductal carcinoma in situ of the breast. Eur J Cancer 1995; 31:1425–1427
Fisher B, Land S, Mamounas E, et al. Prevention of invasive breast cancer in women with ductal carcinoma in situ: an update of the National Surgical Adjuvant Breast Project experience. Semin Oncol 2001; 28:400–418
Bijker N, Meijnen P, Peterse JL, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma-in-situ: ten-year results of European Organisation for Research and Treatment of Cancer randomized phase III Trial 10853—A study by the EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. J Clin Oncol 2006; 24:3381–3387
Gray RJ. A class of K-sample tests for comparing the cumulative incidence of a competing risk. Ann Stat 1988; 16:1141–1154
R Development Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. ISBN 3-900051-07-0, URL http://www.R-project.org (2006)
Bob Gray (2004). cmprsk: Subdistribution analysis of competing risks. R package version 2.1-5. http://www.r-project.org, http://www.biowww.dfci.harvard.edu/~gray
Silverstein MJ, Lagios MD, Craig PH, et al. A prognostic index for ductal carcinoma in situ. Cancer 1996; 77:2267–2274
Webber VL, Heise H, Neifield JP, Costa J. Risk of subsequent breast carcinoma in a population of patients with in-situ breast carcinoma. Cancer 1981; 47:2928–2923
Claus EB, Stowe M, Carter D, Holford T. The risk of a contralateral breast cancer among women diagnosed with ductal and lobular carcinoma in situ: data from the Connecticut Tumor Registry. The Breast 2003; 12:451–456
Lehman CD, Gatsonis C, Kuhl CK, et al. ACRIN Trial 6667 Investigators Group. MRI evaluation of the contralateral breast in women with recently diagnosed breast cancer. N Engl J Med 2007; 356:1295–1303
Qaseem A, Snow V, Sherif K, et al. Clinical efficacy assessment subcommittee of the American College of Physicians. Screening mammography for women 40 to 49 years of age: a clinical practice guideline from the American College of Physicians. Ann Intern Med 2007; 146:516–526
Bodai BI, Boyd B, Brown L, et al. Total cost comparison of 2 biopsy methods for nonpalpable breast lesions. Am J Manag Care 2001; 7:527–538
Secker-Walker RH, Vacek PM, Hooper GJ, Plante DA, Detsky AS. Screening for breast cancer: time, travel, and out-of-pocket expenses. J Natl Cancer Inst 1999; 91:702–708
Liberman L, Feng TL, Dershaw DD, Morris EA, Abramson AF. US-guided core breast biopsy: use and cost-effectiveness. Radiology 1998; 208:717–723
Acknowledgments
Supported in part by the Susan G. Komen Foundation and the Nellie B. Connally Fund for Breast Cancer Research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Presented in part at the American Society of Breast Disease conference, San Francisco, California, 2007
Rights and permissions
About this article
Cite this article
Dawood, S., Broglio, K., Gonzalez-Angulo, A.M. et al. Development of New Cancers in Patients with DCIS: The M.D. Anderson Experience. Ann Surg Oncol 15, 244–249 (2008). https://doi.org/10.1245/s10434-007-9661-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-007-9661-8