
Abstract
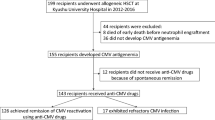
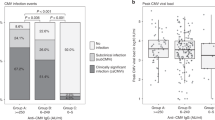
Late cytomegalovirus (CMV) disease beyond day 100 after hematopoietic stem cell transplantation (HSCT) has become an increasing problem after the introduction of preemptive ganciclovir (GCV) administration. To clarify the risk factors and outcome for late CMV reactivation and disease, we retrospectively analyzed the records of 101 Japanese adult patients who underwent allogeneic HSCT between 1998 and 2005 at our hospital. Fifty-one developed late positive CMV antigenemia, with a cumulative incidence of 53%. Recipient CMV seropositivity, the use of alemtuzumab, chronic GVHD, and high-dose steroids were significantly associated with late positive antigenemia. Eight patients developed late CMV disease, with a cumulative incidence of 8%, including retinitis and gastrointestinal disease. None progressed to a fatal disease. The use of alemtuzumab was identified as an independent significant risk factor for late CMV disease, although it was not associated with increased non-relapse mortality. Among the 51 patients with late positive antigenemia, 28 had consistently less than three positive cells, 25 of whom showed negative conversion without antiviral agents. In conclusion, late CMV antigenemia appeared to develop frequently, especially in patients with profound immune suppression; however, a fatal outcome could be prevented by optimal preemptive therapy. Low-level antigenemia may not require antiviral treatments.

Similar content being viewed by others

References
Boeckh M, Gooley TA, Myerson D, Cunningham T, Schoch G, Bowden RA. Cytomegalovirus pp65 antigenemia-guided early treatment with ganciclovir versus ganciclovir at engraftment after allogeneic marrow transplantation: a randomized double-blind study. Blood. 1996;88:4063–71.
Boeckh M, Leisenring W, Riddell SR, et al. Late cytomegalovirus disease and mortality in recipients of allogeneic hematopoietic stem cell transplants: importance of viral load and T-cell immunity. Blood. 2003;101:407–14.
Einsele H, Hebart H, Kauffmann-Schneider C, et al. Risk factors for treatment failures in patients receiving PCR-based preemptive therapy for CMV infection. Bone Marrow Transplant. 2000;25:757–63.
Nguyen Q, Champlin R, Giralt S, et al. Late cytomegalovirus pneumonia in adult allogeneic blood and marrow transplant recipients. Clin Infect Dis. 1999;8:618–23.
Krause H, Hebart H, Jahn G, Müller CA, Einsele H. Screening for CMV-specific T cell proliferation to identify patients at risk of developing late onset CMV disease. Bone Marrow Transplant. 1997;19:1111–6.
Wolf DG, Lurain NS, Zuckerman T, et al. Emergence of late cytomegalovirus central nervous system disease in hematopoietic stem cell transplant recipients. Blood. 2003;101:463–5.
Crippa F, Corey L, Chuang EL, Sale G, Boeckh M. Virological, clinical, and ophthalmologic features of cytomegalovirus retinitis after hematopoietic stem cell transplantation. Clin Infect Dis. 2001;32:214–9.
Kanda Y, Mineishi S, Saito T, et al. Pre-emptive therapy against cytomegalovirus (CMV) disease guided by CMV antigenemia assay after allogeneic hematopoietic stem cell transplantation: a single-center experience in Japan. Bone Marrow Transplant 2001;27:437–44.
Niiya H, Kanda Y, Saito T, et al. Early full donor myeloid chimerism after reduced-intensity stem cell transplantation using a combination of fludarabine and busulfan. Hematologica 2001;86:1071–4.
Kanda Y, Komatsu Y, Akahane M, et al. Graft-versus-tumor effect against advanced pancreatic cancer after allogeneic reduced-intensity stem cell transplantation. Transplantation. 2005;79:821–7.
Kanda Y, Oshima K, Asano-Mori Y, et al. In vivo alemtuzumab enables haploidentical HLA-mismatched hematopoietic stem cell transplantation without ex vivo graft manipulation. Transplantation. 2005;79:1351–7.
Kurihara T, Hayashi J, Matsuoka T, Ito A. HCMV pp65 antigenemia assay using indirect alkaline phosphatase staining method. Bio Med Res. 1995;16:125–9.
Asano-Mori Y, Oshima K, Sakata-Yanagimoto M, et al. High-grade cytomegalovirus antigenemia after hematopoietic stem cell transplantation. Bone Marrow Transplant. 2005;36:813–9.
Kanda Y, Mineishi S, Saito T, et al. Response-oriented preemptive therapy against cytomegalovirus disease with low-dose ganciclovir: a prospective evaluation. Transplantation. 2002;73:568–72.
Asano-Mori Y, Kanda Y, Oshima K, et al. Pharmacokinetics of ganciclovir in haematopoietic stem cell transplantation recipients with or without renal impairment. J Antimicrob Chemother. 2006;57:1004–7.
Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failure probabilities in the presence of competing risks: new representations of old estimators. Stat Med. 1999;18:695–706.
Chakrabarti S, Mackinnon S, Chopra R, et al. High incidence of cytomegalovirus infection after nonmyeloablative stem cell transplantation: potential role of alemtuzumab in delaying immune reconstitution. Blood. 2002;99:4357–63.
Hakki M, Riddell SR, Storek J, et al. Immune reconstitution to cytomegalovirus after allogeneic hematopoietic stem cell transplantation: impact of host factors, drug therapy, and subclinical reactivation. Blood. 2003;102:3060–7.
Acknowledgments
This research was supported by a Grant-in-Aid for Scientific Research from the Ministry of Health, Labour and Welfare.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Asano-Mori, Y., Kanda, Y., Oshima, K. et al. Clinical features of late cytomegalovirus infection after hematopoietic stem cell transplantation. Int J Hematol 87, 310–318 (2008). https://doi.org/10.1007/s12185-008-0051-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-008-0051-1