
Abstract
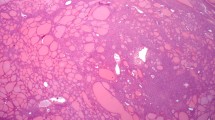
Solitary fibrous tumors (SFTs) are rare tumors in the head and neck, and even more so in the parotid gland. The mass-like clinical presentation and histologic features result in frequent misclassification, resulting in inappropriate clinical management. There are only a few reported cases in the English literature. Twenty-one patients with parotid gland solitary fibrous tumor were compiled from the English literature (Medline 1960–2011) and integrated with this case report. The patients included 11 males and 11 females, aged 11–79 years (mean, 51.2 years), who presented with a parotid gland painless mass gradually increasing in size or with compression symptoms, with a mean duration of symptoms of 24.7 months. The mean tumor size was 4.5 cm. Grossly, all tumors were described as well-circumscribed to encapsulated, firm, homogenous white to tan masses. Seven patients had a preoperative fine needle aspiration performed, with the majority interpreted to represent pleomorphic adenoma or cementifying fibroma. Histologically, the tumors were well circumscribed, although many tumors showed focally entrapped normal salivary gland acini and ducts at the edge. The tumors were cellular, arranged in haphazard short interlacing fascicles of spindled to epithelioid cells. The spindled cells showed tapering cytoplasm with monotonous, round to oval nuclei with coarse nuclear chromatin distribution. Keloid-like to wiry collagen was present between the neoplastic cells. Mitoses were identified in most cases, while necrosis was absent. Isolated, patulous vessels were present, but a well developed “hemangiopericytoma-like” vascular pattern was not seen. Three tumors were classified as malignant, showing marked nuclear pleomorphism and increased mitoses. When immunohistochemistry was performed, all tumors showed strong and diffuse vimentin, with a majority showing CD34, bcl-2 and CD99 immunoreactivity; all cases tested were negative for S100 protein, cytokeratin, EMA, CAM5.2, smooth muscle actin, muscle specific actin, desmin, MYOD1, myogenin, CD117, GFAP, CD31, FVIII-RAg, collagen IV, p63, p53, calponin, caldesmon, CD56, NFP, and ALK-1. The principle differential diagnoses include pleomorphic adenoma, myoepithelioma, nodular fasciitis, schwannoma, fibromatosis coli, spindle cell “sarcomatoid” carcinoma, and spindle cell melanoma. All patients were managed with surgery, while two patients also received radiation therapy. Metastatic disease was identified in one patient immediately after excision. All patients with follow-up were alive without evidence of disease (n = 18), but the average follow-up is only 1.9 years. One patient is alive with disease at 12 months. Parotid gland SFT is a rare tumor, usually presenting in middle aged adults as a slowly growing mass. Characteristic histologic appearance with CD34 and bcl-2 immunoreactivity support the diagnosis. Surgery is the treatment of choice to yield a good outcome.










Similar content being viewed by others


References
Gold JS, Antonescu CR, Hajdu C, Ferrone CR, Hussain M, Lewis JJ, et al. Clinicopathologic correlates of solitary fibrous tumors. Cancer. 2002;94:1057–68.
Brunnemann RB, Ro JY, Ordonez NG, Mooney J, El-Naggar AK, Ayala AG. Extrapleural solitary fibrous tumor: a clinicopathologic study of 24 cases. Mod Pathol. 1999;12:1034–42.
Cho KJ, Ro JY, Choi J, Choi SH, Nam SY, Kim SY. Mesenchymal neoplasms of the major salivary glands: clinicopathological features of 18 cases. Eur Arch Otorhinolaryngol. 2008;265(Suppl 1):S47–56.
Ferreiro JA, Nascimento AG. Solitary fibrous tumour of the major salivary glands. Histopathology. 1996;28:261–4.
Gerhard R, Fregnani ER, Falzoni R, Siqueira SA, Vargas PA. Cytologic features of solitary fibrous tumor of the parotid gland. A case report. Acta Cytol. 2004;48:402–6.
Guerra MF, Amat CG, Campo FR, Perez JS. Solitary fibrous tumor of the parotid gland: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:78–82.
Hanau CA, Miettinen M. Solitary fibrous tumor: histological and immunohistochemical spectrum of benign and malignant variants presenting at different sites. Hum Pathol. 1995;26:440–9.
Kim HJ, Lee HK, Seo JJ, Kim HJ, Shin JH, Jeong AK, et al. MR imaging of solitary fibrous tumors in the head and neck. Korean J Radiol. 2005;6:136–42.
Kumagai M, Suzuki H, Takahashi E, Matsuura K, Furukawa M, Suzuki H, et al. A case of solitary fibrous tumor of the parotid gland: review of the literatures. Tohoku J Exp Med. 2002;198:41–6.
Manglik N, Patil S, Reed MF. Solitary fibrous tumour of the parotid gland. Pathology. 2008;40:89–91.
Messa-Botero OA, Romero-Rojas AE, Chinchilla Olaya SI, az-Perez JA, Tapias-Vargas LF. Primary malignant solitary fibrous tumor/hemangiopericytoma of the parotid gland. Acta Otorrinolaringol Esp. 2011;62:242–5.
Mohammed K, Harbourne G, Walsh M, Royston D. Solitary fibrous tumour of the parotid gland. J Laryngol Otol. 2001;115:831–2.
Ridder GJ, Kayser G, Teszler CB, Pfeiffer J. Solitary fibrous tumors in the head and neck: new insights and implications for diagnosis and treatment. Ann Otol Rhinol Laryngol. 2007;116:265–70.
Sato J, Asakura K, Yokoyama Y, Satoh M. Solitary fibrous tumor of the parotid gland extending to the parapharyngeal space. Eur Arch Otorhinolaryngol. 1998;255:18–21.
Sreetharan SS, Prepageran N. Benign fibrous tumour of the parotid gland. Asian J Surg. 2005;28:45–7.
Suarez Roa ML, Ruiz Godoy Rivera LM, Meneses GA, Granados-Garcia M, Mosqueda TA. Solitary fibrous tumor of the parotid region. Report of a case and review of the literature. Med Oral. 2004;9:82–8.
Takahama A Jr, Leon JE, de Almeida OP, Kowalski LP. Nonlymphoid mesenchymal tumors of the parotid gland. Oral Oncol. 2008;44:970–4.
Thompson M, Cheng LH, Stewart J, Marker A, Adlam DM. A paediatric case of a solitary fibrous tumour of the parotid gland. Int J Pediatr Otorhinolaryngol. 2004;68:481–7.
Wiriosuparto S, Krassilnik N, Bhuta S, Rao J, Firschowitz S. Solitary fibrous tumor: report of a case with an unusual presentation as a spindle cell parotid neoplasm. Acta Cytol. 2005;49:309–13.
Yang XJ, Zheng JW, Ye WM, Wang YA, Zhu HG, Wang LZ, et al. Malignant solitary fibrous tumors of the head and neck: a clinicopathological study of nine consecutive patients. Oral Oncol. 2009;45:678–82.
Orvidas LJ, Kasperbauer JL, Lewis JE, Olsen KD, Lesnick TG. Pediatric parotid masses. Arch Otolaryngol Head Neck Surg. 2000;126:177–84.
Thompson M, Cheng LH, Stewart J. Solitary fibrous tumour of the parotid gland. J Laryngol Otol. 2002;116:319.
Wagner E. Das tuberkelahnliche lymphadenom (der cytogene oder reticulirte tuberkel). Arch Heilk (Leipig). 1870;11:497.
Klemperer P, Rabin CB. Primary neoplasms of the pleura: a report of five cases. Arch Pathol. 1931;11:385–412.
Chan JK. Solitary fibrous tumour–everywhere, and a diagnosis in vogue. Histopathology. 1997;31:568–76.
Rodriguez-Gil Y, Gonzalez MA, Carcavilla CB, Santamaria JS. Lines of cell differentiation in solitary fibrous tumor: an ultrastructural and immunohistochemical study of 10 cases. Ultrastruct Pathol. 2009;33:274–85.
Fletcher CD. The evolving classification of soft tissue tumours: an update based on the new WHO classification. Histopathology. 2006;48:3–12.
Guillou L, Fletcher JA, Fletcher CDM, Mandahl N. Extrapleural solitary fibrous tumour and haemangiopericytoma. In: Fletcher CDM, Unni KK, Mertens F, editors. Pathology and genetics of tumours of soft tissue and bone. Lyon: IARC Press; 2002. p. 86–90.
Gengler C, Guillou L. Solitary fibrous tumour and haemangiopericytoma: evolution of a concept. Histopathology. 2006;48:63–74.
Thompson LD, Miettinen M, Wenig BM. Sinonasal-type hemangiopericytoma: a clinicopathologic and immunophenotypic analysis of 104 cases showing perivascular myoid differentiation. Am J Surg Pathol. 2003;27:737–49.
Goodlad JR, Fletcher CD. Solitary fibrous tumour arising at unusual sites: analysis of a series. Histopathology. 1991;19:515–22.
Jeong AK, Lee HK, Kim SY, Cho KJ. Solitary fibrous tumor of the parapharyngeal space: MR imaging findings. AJNR Am J Neuroradiol. 2002;23:473–5.
Rudolph P, Schubert B, Wacker HH, Parwaresch R, Schubert C. Immunophenotyping of dermal spindle cell tumors: diagnostic value of monocyte marker Ki-M1p and histogenetic considerations. Am J Surg Pathol. 1997;21:791–800.
Thompson LD, Fanburg-Smith JC, Wenig BM. Nodular fasciitis of the external ear region: a clinicopathologic study of 50 cases. Ann Diagn Pathol. 2001;5:191–8.
Cox DP, Daniels T, Jordan RC. Solitary fibrous tumor of the head and neck. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:79–84.
Suster S, Nascimento AG, Miettinen M, Sickel JZ, Moran CA. Solitary fibrous tumors of soft tissue. A clinicopathologic and immunohistochemical study of 12 cases. Am J Surg Pathol. 1995;19:1257–66.
England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol. 1989;13:640–58.
Acknowledgments
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Southern California Permanente Medical Group or The Permanente Medical Group. There is no financial conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bauer, J.L., Miklos, A.Z. & Thompson, L.D.R. Parotid Gland Solitary Fibrous Tumor: A Case Report and Clinicopathologic Review of 22 Cases from the Literature. Head and Neck Pathol 6, 21–31 (2012). https://doi.org/10.1007/s12105-011-0305-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12105-011-0305-8