
Abstract
Background and Study Aims
The formation of a communication between liver abscesses and intrahepatic bile ducts is an uncommon cause of bile leak. The surgical management of biliary fistulas is associated with high morbidity and mortality. We performed a prospective study of the endoscopic management of liver abscess communicating with bile ducts.
Patients and Methods
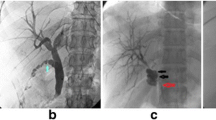
We studied 38 patients with liver abscesses that had ruptured into the intrahepatic bile ducts. The presence of a biliary fistula was suspected by jaundice and/or by the appearance of bile in percutaneous drainage effluent from a liver abscess and was confirmed by endoscopic retrograde cholangiopancreatography (ERCP). Subsequently, patients underwent treatment by endoscopic sphincterotomy and either biliary stenting or nasobiliary drainage. Nasobiliary drains or biliary stents (both 7-Fr) were placed according to standard techniques. Nasobiliary drains were removed when bile leakage stopped and closure of the fistula was confirmed by cholangiography; stents were removed after an interval of 4–6 weeks.
Results
Of the total of 586 patients with liver abscesses, seen over a 10-year period, there were 38 (30 amebic, 8 pyogenic) patients who developed a biliary fistula between the liver abscess cavity and the intrahepatic bile ducts (right intrahepatic bile ducts in 30 patients, left intrahepatic bile ducts in 8 patients). We performed either endoscopic sphincterotomy with insertion of a nasobiliary drain (n = 18) or endoscopic sphincterotomy with biliary stenting (n = 20). The fistulas healed in all patients after a median time of 6 days (range 4–40 days) after endoscopic treatment. The nasobiliary drainage catheters and stents were removed after 8–40 days of their placement.
Conclusions
Endoscopic therapy is an effective mode of treatment for biliary fistulas complicating liver abscesses.


Similar content being viewed by others


References
Gall JK, Vincent AL, Greene JN, Sandin RL, Sniffen JC. Amebic liver abscess. Infect Med. 2001;18:548–553.
Agarwal DK, Baijal SS, Roy S, Mittal BR, Gupta R, Choudhuri G. Percutaneous catheter drainage of amebic liver abscesses with and without intrahepatic biliary communication: a comparative study. Eur J Radiol. 1995;20:61–64.
Foutch PG, Harlan JR, Hoefer M. Endoscopic therapy for patients with a post-operative biliary leak. Gastrointest Endosc. 1993;39:416–421.
Davids PHP, Rauws EAJ, Tytgat GNJ, Huibregtse K. Postoperative bile leakage: endoscopic management. Gut. 1992;33:1118–1122.
Sugiyama M, Atomi Y. Pyogenic hepatic abscess with biliary communication. Am J Surg. 2002;183:205–208.
Griffin J, Jennings C, Owens A. Hepatic amoebic abscess communicating with the biliary tree. Br J Radiol. 1983;56:887–890.
Do H, Lambiase RE, Deyoe L, Cronan JJ, Dorfman GS. Percutaneous drainage of hepatic abscesses: comparison of results in abscesses with and without intrahepatic biliary communication. AJR Am J Radiol. 1991;157:1209–1212.
Bayraktar Y, Arslan S, Sivri B, Eryilmaz M, Akova M, Van Thiel DH, Kayhan B. Percutaneous drainage of hepatic abscesses: therapy does not differ for those with identifiable biliary fistula. Hepatogastroenterology. 1996;43:620–626.
Ibrarullah M, Agarwal DK, Baijal SS, Mittal BR, Kapoor VK. Amebic liver abscess with intra-biliary rupture. HPB Surg. 1994;7:305–313.
Sonsuz A, Basaranoğlu M, Sentürk H, Celik AF, Tanriover V. Amebic abscess of the caudate lobe with spontaneous rupture into the biliary tract. J Clin Gastroenterol. 1998;26:355–356.
Meng XY, Wu JX. Perforated amebic liver abscess: clinical analysis of 110 cases. South Med J. 1994;87:985–990.
Kumar N, Sreeniwas DV, Chowdhury V, Puri AS. Amoebic liver abscess communicating with intrahepatic bile duct. Trop Gastroenterol. 1995;16:47–49.
Sandeep SM, Banait VS, Thakur SK, Bapat MR, Rathi PM, Abraham P. Endoscopic biliary drainage in patients with amebic liver abscess and biliary communication. Indian J Gastroenterol. 2006;25:125–127.
Sharma BC, Agarwal N, Garg S, Kumar R, Sarin SK. Endoscopic management of liver abscesses and cysts that communicate with intrahepatic bile ducts. Endoscopy. 2006;38:249–253.
Conflict of interest
The authors have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sharma, B.C., Garg, V. & Reddy, R. Endoscopic Management of Liver Abscess with Biliary Communication. Dig Dis Sci 57, 524–527 (2012). https://doi.org/10.1007/s10620-011-1872-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10620-011-1872-y