
Abstract
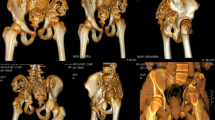
Gorham-Stout disease is defined as a spontaneous, massive, and nonfamilial idiopathic osteolysis. The diagnosis is based essentially on radiological and histological findings. Biopsy reviews always reveal excessive intraosseous nonmalignant proliferation of small vessels, which results in bone resorption and may extend to adjacent bones and soft tissues. These lesions are progressively replaced by extensive fibrosis. Since its first description in 1955, there is still controversy about its prognosis, etiology, and treatment. A case of Gorham-Stout disease, located on the right pelvis, is reported with 50 years of clinical and radiographic follow-up, in a man who has never been treated. To date, this is the longest documented case report of the disease and its rare natural history. It demonstrates that after a variable time of evolution, the massive osteolysis is able to undergo spontaneous arrest and that the lesions may remain stable during several decades. Besides, no reossification was observed, even after 37 years of disease quiescence. Based on a large review of the literature, the authors then discuss the prognosis, etiopathology, and different therapeutic options available to halt the progression of the osteolysis.






Similar content being viewed by others


References
Jackson JBS (1838) A boneless arm. Boston Med Surg J 18:368–369
Hardegger F, Simpson LA, Segmueller G (1985) The syndrome of idiopathic osteolysis. Classification, review, and case report. J Bone Joint Surg Br 67:88–93
Gorham LW, Stout AP (1955) Massive osteolysis (acute spontaneous absorption of bone, phantom bone, disappearing bone). J Bone Joint Surg Am 37:985–1004
Milner S, Baker SL (1958) Disappearing bones. J Bone Joint Surg Br 40:502–513
Green HD, Mollica AJ, Karuza AS (1995) Gorham’s disease: a literature review and case reports. J Foot Ankle Surg 34:431–441
Chong Ng L, Sell P (2003) Gorham disease of the cervical spine-a case report and review of the literature. Spine 28:E355–E358
Christ F, Siemes HD, Stiens R (1984) Pelvic bone angiomas. Rofo 140:79–83
Florchinger A, Bottger E, Claass-Bottger F, Georgi M, Harms J (1998) Gorham–Stout syndrome of the spine. Case report and review of the literature. Rofo 168:68–76
Klein M, Metelmann HR, Gross U (1996) Massive osteolysis (Gorham–Stout syndrome) in the maxillofacial region: an unusual manifestation. Int J Oral Maxillofac Surg 25:376–378
Stöve J, Reichelt A (1995) Massive osteolysis of the pelvis, femur and sacral bone with a Gorham–Stout syndrome. Arch Orthop Trauma Surg 114:207–210
Kulenkampff HA, Richter GM, Hasse WE, Adler CP (1990) Massive pelvic osteolysis in the Gorham–Stout syndrome. Int Orthop 14:361–366
Moller G, Priemel M, Amling M, Werner M, Kuhlmey AS, Delling G (1999) The Gorham–Stout syndrome (Gorham’s massive osteolysis). A report of six cases with histopathological findings. J Bone Joint Surg Br 81:501–506
Bode-Lesniewska B, von Hochstetter A, Exner GU, Hodler J (2002) Gorham–Stout disease of the shoulder girdle and cervico-thoracic spine: fatal course in a 65-year-old woman. Skeletal Radiol 31:724–729
Cannon SR (1986) Massive osteolysis. J Bone Joint Surg Br 68:24–28
Dunbar SF, Rosenberg A, Mankin H, Rosenthal D, Suit HD (1993) Gorham’s massive osteolysis: the role of radiation therapy and a review of the literature. Int J Radiat Oncol Biol Phys 26:491–497
Mochizuki K, Koyama S, Ishii Y (2000) Seventeen-year follow-up of massive osteolysis of the scapula. J Orthop Sci 5:618–621
Turra S, Gigante C, Scapinelli R (1990) A twenty-year follow-up study of a case of surgically treated massive osteolysis. Clin Orthop 250:297–302
Campbell J, Almond HG, Johnson R (1975) Massive osteolysis of the humerus with spontaneous recovery. J Bone Joint Surg Br 57:238–240
Rauh G, Gross M (1997) Disappearing bone disease (Gorham–Stout disease): report of a case with a follow-up of 48 years. Eur J Med Res 2:425–427
Kery L, Wouters HW (1970) Massive osteolysis. Report of two cases. J Bone Joint Surg Br 52:452–459
Hagberg H, Lamberg K, Åström G (1997) Alpha-2b interferon and oral clodronate for Gorham’s disease. Lancet 350:1822–1823
Tie ML, Poland GA, Rosenow EC 3rd (1994) Pleural effusion: a complication of Gorham’s disease. Pediatr Radiol 24:542
Choma ND, Biscotti CV, Bauer T, Mehta AC, Licata AA (1987) Gorham’s syndrome: a case report and review of the literature. Am J Med 83:1151–1156
Knoch HG (1963) Die Gorhamsche Krankheit aus klinisher Sicht. Zentralbl Chir 18:674–683
Mundy GR, Varani J, Orr W, Gondek MD, Ward PA (1978) Resorbing bone is chemotactic for monocytes. Nature 275:132–135
Heyden G, Kindblom LG, Nielsen JM (1977) Disappearing bone disease: a clinical and histological study. J Bone Joint Surg Am 59:57–61
Devlin RD, Bone Hg, Roodman GD (1996) Interleukin-6: a potential mediator of the massive osteolysis in patients with Gorham–Stout disease. J Clin Endocrinol Metab 81:1893–1897
Patrick JH (1976) Massive osteolysis complicated by chylothorax successfully treated by pleurodesis. J Bone Joint Surg Br 58:347–349
Plontke S, Koitschev A, Ernemann U, Pressler H, Zimmermann R, Plasswilm L (2002) Massive Gorham–Stout osteolysis of the temporal bone and the craniocervical transition. HNO 50:354–357
Mathias K, Hoffmann J, Martin K (1986) Gorham–Stout syndrome of the mandible. Radiology 26:439–441
Meydam K, Hering KG, Jaspers U, Machtens E (1985) Gorham–Stout syndrome-progressive osteolysis with viscerocranial involvement. Strahlentherapie 161:625–627
Sage MR, Allen PW (1974) Massive osteolysis. Report of a case. J Bone Joint Surg Br 56:130–135
Anavi Y, Sabes WR, Mintz S (1989) Gorham’s disease affecting the maxillofacial skeleton. Head Neck 11:550–557
Woodward HR, Chan DP, Lee J (1981) Massive osteolysis of the cervical spine. A case report of bone graft failure. Spine 6:545–549
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Boyer, P., Bourgeois, P., Boyer, O. et al. Massive Gorham-Stout syndrome of the pelvis. Clin Rheumatol 24, 551–555 (2005). https://doi.org/10.1007/s10067-005-1088-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-005-1088-7