
Abstract
Background
The standard treatment for cervical radiculopathy is anterior discectomy and fusion. The authors describe a minimally invasive anterior cervical foraminotomy as a surgical option for direct nerve root decompression in cervical radiculopathy.
Method
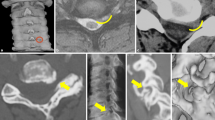
Through a modified Smith-Robinson approach, the prevertebral fascia is mobilized laterally, displacing the sympathetic chain with it. A thumbnail size portion of the longus colli muscle is removed. A tubular retractor is placed, centered over the index uncovertebral joint. The lateral part of the joint is progressively drilled towards the foramen. After exposure of the intervertebral foramen, the perivascular ligamentous tissue is opened. Removal of disc fragments and osteophytes allows direct visualization and direct decompression of the nerve root.
Conclusion
Anterior cervical foraminotomy is a safe “motion preserving” procedure for direct nerve decompression in selected patients with cervical radiculopathy that does not require cervical fusion.






Similar content being viewed by others


References
Hacker RJ, Miller CG (2003) Failed anterior cervical foraminotomy. J Neurosurg 98:126–130
Hartman J (2014) Anatomy and clinical significance of the uncinate process and uncovertebral joint: a comprehensive review. Clin Anat 27:431–440. https://doi.org/10.1002/ca.22317
Jho HD (1996) Microsurgical anterior cervical foraminotomy for radiculopathy: a new approach to cervical disc herniation. J Neurosurg 84:155–160. https://doi.org/10.3171/jns.1996.84.2.0155
Jho HD (2003) Failed anterior cervical foraminotomy. J Neurosurg 98:121–125 discussion 125
Jho HD, Kim WK, Kim MH (2002) Anterior microforaminotomy for treatment of cervical radiculopathy: part 1--disc-preserving “functional cervical disc surgery”. Neurosurgery 51:S46–S53
Nguyen J, Chu B, Kuo CC, Leasure JM, Ames C, Kondrashov D (2017) Changes in foraminal area with anterior decompression versus keyhole foraminotomy in the cervical spine: a biomechanical investigation. J Neurosurg Spine 27:620–626. https://doi.org/10.3171/2017.2.SPINE141237
Pait TG, Killefer JA, Arnautovic KI (1996) Surgical anatomy of the anterior cervical spine: the disc space, vertebral artery, and associated bony structures. Neurosurgery 39:769–776. https://doi.org/10.1097/00006123-199610000-00026
Park YK, Moon HJ, Kwon TH, Kim JH (2013) Long-term outcomes following anterior foraminotomy for one- or two-level cervical radiculopathy. Eur Spine J 22:1489–1496. https://doi.org/10.1007/s00586-013-2712-x
Yilmazlar S, Kocaeli H, Uz A, Tekdemir I (2003) Clinical importance of ligamentous and osseous structures in the cervical uncovertebral foraminal region. Clin Anat 16:404–410. https://doi.org/10.1002/ca.10158
Zou S, Gao J, Xu B, Lu X, Han Y, Meng H (2017) Anterior cervical discectomy and fusion (ACDF) versus cervical disc arthroplasty (CDA) for two contiguous levels cervical disc degenerative disease: a meta-analysis of randomized controlled trials. Eur Spine J 26:985–997. https://doi.org/10.1007/s00586-016-4655-5
Acknowledgments
We heartily thank Pr. Selcuk Yilmazlar, Department of Neurosurgery, Uludag University (Bursa, Turkey), for permitting the reproduction of Fig. 1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors
Additional information
Key Points
1) Single-level cervical radiculopathy may be treated with ACF.
2) Careful preoperative neurological and radiological investigations are mandatory.
3) The course of VA needs to be studied on preoperative imaging.
4) The use and careful placement of tubular retractors may help preventing VA injury and excessive bone removal by guiding drilling trajectory.
5) Identification of bony landmarks intraoperatively is crucial.
6) Anterior foraminotomy permits a direct “tailored” foraminal decompression.
7) The UP is removed only on its posterior half.
8) “Tailored” bone removal prevents iatrogenic instability.
9) Removal of disc fragments and osteophytes decompresses the nerve root.
10) Postoperative follow-up is mandatory.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Spine degenerative
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Maduri, R., Bobinski, L. & Duff, J.M. Minimally invasive anterior foraminotomy for cervical radiculopathy: how I do it. Acta Neurochir 162, 679–683 (2020). https://doi.org/10.1007/s00701-019-04201-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-019-04201-y