
Abstract
Objective
Solitary fibrous tumor is a rare, spindle-cell benign mesenchymal neoplasm and has a high recurrence rate. In this study, we reviewed our experience in the diagnosis and treatment of 24 patients with central nervous system solitary fibrous tumors.
Methods
Clinical data were retrieved from the medical records. Prognosis was assessed by clinic service and telephone interview. The specimens were stained with hematoxylin and eosin. Immunohistochemistry for CD34, CD99, EMA, HMB-45, Bcl-2, vimentin, GFAP, S-100, MBP, CK and MIB-1 was performed in all cases. Distributions of time to progression and recurrence were estimated using the KaplanMeier method and compared using the log-rank test.
Results
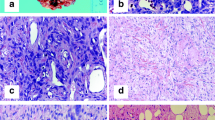
The 24 patients included 13 men and 11 women with a median age of 49.0 years. The most frequent initial symptoms were headache, dizziness, unstable walk and hearing loss. The most common location was cerebellar pontine angle (n = 6). Surgery reached gross total removal for 18 patients but subtotal removal for six patients on initial operation. Histopathologic examination showed spindle to oval cells were disposed in wavy fascicles between prominent, eosinophilic bands of collagen. Dense bands of collagen appeared in cross section as minute nodules that separated individual tumor cells. Cellular areas with a partial hemangiopericytoma pattern were noted in six cases. Atypical presentations were shown on initial operation in three cases. CD34, CD99 and vimentin were 100% positive; but EMA, CK, MBP, HBM-45 and GRAP were 100% negative. The positive in Bcl-2, RF and S-100 was 89%, 85% and 26%, respectively. Follow-up information was available for 23 patients. The median follow-up period was 36.0 months. Nine patients recurred and one patient died from the progression. Incomplete surgical resection was significantly associated with recurrence (p = 0.010). MIB-1 labeling index in recurrence was higher than in no recurrence (6.0% versus 3.4%, p = 0.029). All treated with subtotal removal only had subsequent tumor recurrence or progression; however, the two patients who were administered adjuvant radiosurgery after subtotal removal did not recur or progress. Adjuvant radiosurgery seemed to improve the prognosis (p = 0.028).
Conclusions
Solitary fibrous tumor is a rare mesenchymal tumor with a propensity to recur. The most affected area is the cerebellopontine angle. Immunohistochemistry should be used to differentiate solitary fibrous tumor from other tumors. The extent of resection, MIB-1 labeling index and some anaplastic features might be predictive for recurrence. Postoperative radiosurgery might be an option in incompletely resected solitary fibrous tumor. Regular and long-term follow-up remains mandatory to monitor recurrence.





Similar content being viewed by others


References
Carneiro SS, Scheithauer BW, Nascimento AG, Hirose T, Davis DH (1996) Solitary fibrous tumor of the meninges: a lesion distinct from fibrous meningioma. A clinicopathologic and immunohistochemical study. Am J Clin Pathol 106:217–224
Caroli E, Salvati M, Orlando ER, Lenzi J, Santoro A, Giangaspero F (2004) Solitary fibrous tumors of the meninges: report of four cases and literature review. Neurosurg Rev 27:246–251
Choi CY, Han SR, Yee GT, Joo M (2011) An intracranial malignant solitary fibrous tumor. Neuropathology 31:177–182
Cummings TJ, Burchette JL, McLendon RE (2001) CD34 and dural fibroblasts: the relationship to solitary fibrous tumor and meningioma. Acta Neuropathol 102:349–354
England DM, Hochholzer L, McCarthy MJ (1989) Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol 13:640–658
Hayashi Y, Uchiyama N, Nakada M, Iwato M, Kita D, Higashi R, Hirota Y, Kai Y, Kuratsu J, Hamada J (2009) A reevaluation of the primary diagnosis of hemangiopericytoma and the clinical importance of differential diagnosis from solitary fibrous tumor of the central nervous system. Clin Neurol Neurosurg 111:34–38
Jalali R, Srinivas C, Nadkarni TD, Rajasekharan P (2008) Suprasellar haemangiopericytoma—challenges in diagnosis and treatment. Acta Neurochir (Wien) 150:67–71
Kim KA, Gonzalez I, McComb JG, Giannotta SL (2004) Unusual presentations of cerebral solitary fibrous tumors: report of four cases. Neurosurgery 54:1004–1009
Kinfe TM, Tschan CA, Stan AC, Krauss JK (2008) Solitary fibrous tumor of the foramen of Monro. Clin Neurol Neurosurg 110:404–407
Klemperer P, Rabin CB (1931) Primary neoplasms of the pleura: a report of five cases. Arch Pathol 11:385–412
Lawlor MW, Nielsen GP, Louis DN (2008) Malignant solitary fibrous tumour of the meninges with marked amianthoid fibre deposition. Neuropathol Appl Neurobiol 34:569–572
Louis DN, Ohgaki H, Wiestler OD, Cavenee WK (eds) (2007) WHO ClassiWcation of tumours of the central nervous system. IARC, Lyon
Macfarlane RG, Galloway M, Plowman PN, Thomas DG (2005) A highly vascular intracranial solitary fibrous tumor treated with radiotherapy and toremifene: case report. Neurosurgery 56:E1378
Mekni A, Kourda J, Hammouda KB, Tangour M, Kchir N, Zitouna M, Haouet S (2009) Solitary fibrous tumour of the central nervous system: pathological study of eight cases and review of the literature. Pathology 41:649–654
Metellus P, Bouvier C, Guyotat J, Fuentes S, Jouvet A, Vasiljevic A, Giorgi R, Dufour H, Grisoli F, Figarella-Branger D (2007) Solitary fibrous tumors of the central nervous system: clinicopathological and therapeutic considerations of 18 cases. Neurosurgery 60:715–722
Nakahara K, Yamada M, Shimizu S, Fujii K (2006) Stereotactic radiosurgery as adjuvant treatment for residual solitary fibrous tumor. Case report J Neurosurg 105:775–776
Nawashiro H, Nagakawa S, Osada H, Katoh H, Ohnuki A, Tsuzuki N, Miyazawa T, Shima K, Ogata S, Aida S (2000) Solitary fibrous tumor of the meninges in the posterior cranial fossa: magnetic resonance imaging and histological correlation—case report. Neurol Med Chir (Tokyo) 40:432–434
Ogawa K, Tada T, Takahashi S, Sugiyama N, Inaguma S, Takahashi SS, Shirai T (2004) Malignant solitary fibrous tumor of the meninges. Virchows Arch 444:459–464
Pizem J, Matos B, Popovic M (2004) Malignant intracranial solitary fibrous tumour with four recurrences over a 30-year period. Neuropathol Appl Neurobiol 30:696–701
Suzuki SO, Fukui M, Nishio S, Iwaki T (2000) Clinicopathological features of solitary fibrous tumor of the meninges: An immunohistochemical reappraisal of cases previously diagnosed to be fibrous meningioma or hemangiopericytoma. Pathol Int 50:808–817
Tihan T, Viglione M, Rosenblum MK, Olivi A, Burger PC (2003) Solitary fibrous tumors in the central nervous system. A clinicopathologic review of 18 cases and comparison to meningeal hemangiopericytomas. Arch Pathol Lab Med 127:432–439
Vassal F, Manet R, Forest F, Camdessanche JP, Peoc’h M, Nuti C (2011) Solitary fibrous tumors of the central nervous system: report of five cases with unusual clinicopathological and outcome patterns. Acta Neurochir (Wien) 153:377–384
Weon YC, Kim EY, Kim HJ, Byun HS, Park K, Kim JH (2007) Intracranial solitary fibrous tumors: imaging findings in 6 consecutive patients. AJNR Am J Neuroradiol 28(8):1466–1469
Yilmaz C, Kabatas S, Ozen OI, Gulsen S, Caner H, Altinors N (2009) Solitary fibrous tumor. J Clin Neurosci 16:1578–1581
Yin W, Ma C, Wu J, Cai B, You C (2010) A primary atypical solitary fibrous tumor of the sella mimicking nonfunctional pituitary adenoma: a case report. Acta Neurochir (Wien) 152:519–522
Zhang J, Cheng H, Qiao Q, Zhang JS, Wang YM, Fu X, Li Q (2010) Malignant solitary fibrous tumor arising from the pineal region: case study and literature review. Neuropathology 30:294–298
Zorludemir S, Scheithauer BW, Hirose T, Van Houten C, Miller G, Meyer FB (1995) Clear cell meningioma. A clinicopathologic study of a potentially aggressive variant of meningioma. Am J Surg Pathol 19:493–505
Acknowledgments
We thank Professor Liang-Fu Zhou, Professor Ying Mao, Professor Feng-Ping Huang, Professor Xiao-Ming Che, Professor Ye Gong, Professor Rong Zhang, Professor Wei Zhu and Professor Zhi-Yong Qin for providing patients’ information. We thank Professor Timir Banerjee of Louisville, KY, USA for reading the manuscript and editing it. We also thank Professor Jian-Kang Shen for expert opinions during the development of this manuscript. This work is supported by grants from China Postdoctoral Science Foundation (No. 20100480568)
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Comment
Neurosurgery at Huashan Hospital, Shanghai, is at its own level of magnitude [1]. In 9 years (2002–10), they operated on 6,700 meningiomas, 183 hemangiopericytomas (rare) and 28 solitary fibrous tumors (very rare) of the CNS. Their 28 solitary fibrous tumours make obviously the largest published series to date - but that is only secondary here. The most important point is the change of times. China and its megacities allow the creation of huge neurosurgical units compared with our European ones, and such units (1) may produce series of patients five- to ten-times larger than published from Europe, (2) may allow subspecialization with tens of neurosurgeons and dedicated instrumentation into a much deeper level that in standard European units, and (3) may at best represent the frontline of neurosurgical decidation and innovation.
Young neurosurgeons, look East!
Juha E Jääskeläinen
Kuopio Finland
1. Mao Y, Shi ZF, Zhou LF, Zhao Y (2011) Huashan Hospital affiliated to Fudan University: spanning a century of history. World Neurosurg 75(3–4):369–376
Hong Chen and Xian-Wei Zeng contributed equally to this study
Rights and permissions
About this article
Cite this article
Chen, H., Zeng, XW., Wu, JS. et al. Solitary fibrous tumor of the central nervous system: a clinicopathologic study of 24 cases. Acta Neurochir 154, 237–248 (2012). https://doi.org/10.1007/s00701-011-1160-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00701-011-1160-9