
Abstract
Introduction
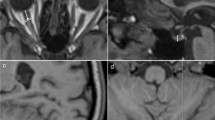
Empty sella in MRI is an important finding associated with idiopathic intracranial hypertension (IIH). This study assesses the sensitivity and reproducibility of several morphological measures of the sella and pituitary gland to indentify the measure that best differentiates IIH from controls. Additionally, the study assesses reversal in gland compression following treatment.
Methods
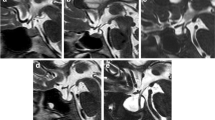
Sagittal 3D-T1W sequence with 1 mm isotropic resolution was obtained from ten newly diagnosed IIH patients and 11 matched healthy controls. Follow-up MRI scans were obtained from eight patients at 1-week post-lumbar puncture and acetazolamide treatment. 1D and 2D measures of absolute and normalized heights and cross-sectional areas of the gland and sella were obtained to identify the measure that best differentiates IIH patients and controls.
Results
Overall area-based measurements had higher sensitivity than length with p < 0.0001 for sella area compared with p = 0.004 for normalized gland height. The gland cross-sectional areas were similar in both cohorts (p = 0.557), while the sella area was significantly larger in IIH, 200 ± 24 versus 124 ± 25 mm2, with the highest sensitivity and specificity, 100 % and 90.9 %, respectively. Absolute gland area was the most sensitive measure for assessing post treatment changes, with 100 % sensitivity and 50 % specificity. Average post-treatment gland area was 18 % larger (p = 0.016). Yet, all eight patients remained within the empty sella range based on a normalized gland area threshold of 0.41.
Conclusions
Sellar area is larger in IIH, and it demonstrated highest sensitivity for differentiating IIH from control subjects, while absolute gland area was more sensitive for detecting post treatment changes.



Similar content being viewed by others

References
Kaufman B (1968) The “empty” sella turcica—a manifestation of the intrasellar subarachnoid space. Radiology 90:931–941
Foley KM, Posner JB (1975) Does pseudotumor cerebri cause the empty sella syndrome? Neurology 25:565–569
Wessel K, Thron A, Linden D, Petersen D, Dichgans J (1987) Pseudotumor cerebri: clinical and neuroradiological findings. Eur Arch Psychiatry Neurol Sci 237:54–60
Berke JP, Buxton LF, Kokmen E (1975) The “empty” sella. Neuroradiology 25:1137–1143
Neelon FA, Goree JA, Lebovitz HE (1973) The primary empty sella: clinical and radiographic characteristics and endocrine function. Med (Baltimore) 52:73–92
Yuh WT, Zhu M, Taoka T et al (2000) MR imaging of pituitary morphology in idiopathic intracranial hypertension. J Magn Reson Imaging 12:808–813
Gibby WA, Cohen MS, Goldberg HI, Sergott RC (1993) Pseudotumor cerebri: CT findings and correlation with vision loss. AJR Am J Roentgenol 160:143–146
Brodsky MC, Vaphiades M (1998) Magnetic resonance imaging in pseudotumor cerebri. Ophthalmology 105:1686–1693
Weisberg LA (1985) Computed tomography in benign intracranial hypertension. Neurology 35:1075–1078
Degnan AJ, Levy LM (2011) Pseudotumor cerebri: brief review of clinical syndrome and imaging findings. AJNR Am J Neuroradiol 32:1986–1993
Sage MR, Blumbergs PC (2000) Primary empty sella turcica: a radiological–anatomical correlation. Australas Radiol 44:341–348
Sage MR, Blumbergs PC, Fowler GW (1982) The diaphragma sellae: its relationship to normal sellar variations in frontal radiographic projections. Radiology 145:699–701
Bergland RM, Ray BS, Torack RM (1968) Anatomical variations in the pituitary gland and adjacent structures in 225 human autopsy cases. J Neurosurg 28:93–99
Quintos JB, Shah A, Castells S (2006) Transient pituitary dysfunction, empty sella, pseudotumor cerebri in a morbidly obese adolescent. Pediatr Endocrinol Rev Suppl 4:576–578
Kim JH, Ko JH, Kim HW, Ha HG, Jung CK (2009) Analysis of empty sella secondary to the brain tumors. J Korean Neurosurg Soc 46:355–359
Takanashi J, Suzuki H, Nagasawa K, Kobayashi K (2001) Empty sella in children as a key for diagnosis. Brain Dev 23:422–423
Francois I, Casteels I, Silberstein J, Casaer P, de Zegher F (1997) Empty sella, growth hormone deficiency and pseudotumor cerebri: effect of initiation, withdrawal, and resumption of growth hormone therapy. Eur J Pediatr 156:69–70
Zagardo MT, Cail WS, Kelman SE, Rothman MI (1996) Reversible empty sella in idiopathic intracranial hypertension: an indicator of successful therapy? AJNR Am J Neuroradiol 17:1953–1956
Friedman DI, Jacobson DM (2002) Diagnostic criteria for idiopathic intracranial hypertension. Neurology 59:1492–1495
McComb JG (1983) Recent research into the nature of cerebrospinal fluid formation and absorption. J Neurosurg 59:369–383
Alperin N, Ranganathan S, Bagci AM et al (2013) MRI evidence of impaired CSF homeostasis in obesity-associated idiopathic intracranial hypertension. AJNR Am J Neuroradiol 34:29–34
Butros SR, Goncalves LF, Thompson D, Agarwal A, Lee HK (2012) Imaging features if idiopathic intracranial hypertension, including a new finding: widening of the foramen ovale. Acta Radiol 53:682–688
Acknowledgments
This study is supported in part by NIH grant R01 NS052122. The authors thank Ms. Lauren S. Meshkov for her participation in the initial phase of the study.
Conflict of interest
NA is a shareholder in Alperin Noninvasive Diagnostics, Inc.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ranganathan, S., Lee, S.H., Checkver, A. et al. Magnetic resonance imaging finding of empty sella in obesity related idiopathic intracranial hypertension is associated with enlarged sella turcica. Neuroradiology 55, 955–961 (2013). https://doi.org/10.1007/s00234-013-1207-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-013-1207-0