
Abstract
Summary
Bone health status of the radius in individuals with chronic stroke was evaluated using peripheral quantitative computed tomography. Bone mineral density and cortical thickness on the affected side were compromised when compared with the unaffected side. Muscle weakness, spasticity, and disuse were identified as contributing factors to such changes.
Introduction
Following a stroke, demineralization and geometric changes occur in bone as a result of disuse and residual impairments, and these can contribute to an increased risk of fragility fractures.
Methods
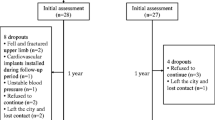
This study used peripheral quantitative computed tomography (pQCT) to evaluate volumetric bone mineral density and geometry at the midshaft radius in people living with chronic stroke. Older individuals with chronic stroke were recruited. Each subject underwent a pQCT scan of the midshaft radius at the 30% site on both upper limbs. Muscle strength, motor function, spasticity, and chronic disuse were also evaluated. Data from 47 subjects (19 women) were assessed.
Results
A significant difference was found between the two limbs for cortical bone mineral content, cortical bone mineral density, cortical thickness, and polar stress-strain index. There was no significant side-to-side difference in total bone area. Percent side-to-side difference in muscle strength, spasticity, and chronic disuse were significant determinants of percent side-to-side difference in cortical bone mineral content and cortical thickness.
Conclusions
The findings suggest that following chronic stroke, endosteal resorption of the midshaft radius occurred with a preservation of total bone area. Muscle weakness, spasticity, chronic disuse significantly contributed to demineralization and geometric changes in the radius following chronic stroke.
Similar content being viewed by others

References
Wolf SL, Lecraw DE, Barton LA et al (1989) Forced use of hemiplegic upper extremities to reverse the effect of learned nonuse among chronic stroke and head-injured patients. Exp Neurology 104:125–132
Hamdy RC, Krishnaswamy G, Cancellaro V et al (1993) Changes in bone mineral content and density after stroke. Am J Phys Med Rehabil 72:188–191
Prince RL, Price RI, Ho S (1988) Forearm bone loss in hemiplegia: a model for the study of immobilization osteoporosis. J Bone Miner Res 3:305–310
Liu M, Tsuji T, Higuchi Y et al (1999) Osteoporosis in hemiplegic stroke patients as studied with dual-energy X-ray absorptiometry. Arch Phys Med Rehabil 80:1219–1226
Ramnemark A, Nyberg L, Lorentzon R et al (1999) Progressive hemiosteoporosis on the paretic side and increased bone mineral density in the nonparetic arm the first year after severe stroke. Osteoporos Int 9:269–275
Kanis J, Oden A, Johnell O (2001) Acute and long-term increase in fracture risk after hospitalization for stroke. Stroke 32:702–706
Ramnemark A, Nyberg L, Borssen B et al (1998) Fractures after stroke. Osteoporos Int 8:92–95
Dennis MS, Lo KM, McDowall M et al (2002) Fractures after stroke. Frequency, types and associations. Stroke 33:728–734
Garrett NA, Brasure M, Schmitz KH et al (2004) Physical inactivity. Direct cost to a Health Plan. Am J Prev Med 27:304–309
Jorgensen L, Jacobsen BK (2001) Functional status of the paretic arm affects the loss of bone mineral in the proximal humerus after stroke: a 1-year prospective study. Calcif Tissue Int 68:11–15
Pang MYC, Eng JJ (2005) Muscle strength is a determinant of bone mineral content in the hemiparetic upper extremity: implications for stroke rehabilitation. Bone 37:103–111
Iwamoto J, Takeda T, Ichimura S (2001) Relationships between physical activity and metacarpal cortical bone mass and bone resorption in hemiplegic patients. J Orthop Sci 6:227–233
Sahin L, Ozoran K, Gunduz OH et al (2001) Bone mineral density in patients with stroke. Am J Phys Med Rehabil 80:592–596
Sato Y, Fujimatsu Y, Kikuyama M et al (1998) Influence of immobilization on bone mass and bone metabolism in hemiplegic elderly patients with long-standing stroke. J Neurol Sci 156:205–210
Frost HM (2003) Absorptiometry and “osteoporosis”: problems. J Bone Miner Metab 21:255–260
Burr DB, Turner Ch (2003) Biomechanics of bone. In: Favus MJ (ed) Primer on the metabolic bone diseases and disorders of mineral metabolism, 5th edn. American Society for Bone and Mineral Research, Washington DC, pp 58–64
Ashe MC, Fehling P, Eng JJ et al (in press) Bone structural changes to chronic disuse following stroke. J Musculoskelet and Neuron Interact
Riggs LB, Melton LJ, Robb RA et al (2004) A population-based study of age and sex differences in bone volumetric density, size, geometry and structure at different skeletal sites. J Bone Miner Res 19:1945–1954
Pang MYC, Eng JJ, Dawson AS et al (2005) A community-based Fitness and Mobility Exercise program for older adults with chronic stroke: a randomized controlled trial. J Am Geriatr Soc 53:1667–1674
Folstein MF, Folstein, SE, McHugh PR (1975) Mini-mental state: a practical method for grading the state of patients for the clinician. J Psychiat Res 12:189–198
Kelly-Hayes M, Robertson JT, Broderick JP et al (1998) The American Heart Association Stroke Outcome Classification: executive summary. Circulation 97:2474–2478
Liu-Ambrose TY, Khan KM, Eng JJ et al (2004) Both resistance and agility training increase cortical bone density in 75- to 85-year-old women with low bone mass: a 6-month randomized controlled trial. J Clin Densitom 7:390–398
Pang MYC, Ashe MC, Eng JJ et al (2006) A 19-week exercise program for people with chronic stroke enhances bone geometry at the tibia: a peripheral quantitative computed tomography study. Osteoporos Int 17:1615–1625
Fess EE (1992) Grip strength. In: Casanova JS (ed) Clinical assessment recommendations, 2nd edn. American Society of Hand Therapists, Chicago, pp 41–45
McCrea PH, Eng JJ, Hodgson AJ (2003) Time and magnitude of torque generation is impaired in both arms following stroke. Muscle Nerve 28:46–53
Bohannon RW (1997) Measurement and nature of muscle strength in patients with stroke. J Neuro Rehabil 11:115–125
Mathiowetz V (2002) Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occup Ther Int 9:201–209
Wolf SL, Catlin PA, Ellis M et al (2001) Assessing Wolf Motor Function Test as outcome measure for research in patients after stroke. Stroke 32:1635–1639
Morris DM, Uswatte G, Crago JE et al (2001) The reliability of the Wolf Motor Function Test for assessing upper extremity function after stroke. Arch Phys Med Rehabil 82:750–755
Bohannon BW, Smith MB (1987) Interrater reliability of a Modified Ashworth Scale of muscle spasticity. Phys Ther 67:206–207
van der Lee JH, Beckerman H, Knol DL et al (2004) Clinimetric properties of the Motor Activity Log for the assessment of arm use in hemiparetic patients. Stroke 35:1410–1414
Hughes VA, Frontera WR, Dallal GE et al (1995) Muscle strength and body composition: associations with bone density in older subjects. Med Sci Sports Exerc 27:967–974
Di Monaco M, Di Monaco R, Manca M et al (2000) Handgrip strength is an independent predictor of distal radius bone mineral density in postmenopausal women. Clin Rheumatol 19:473–476
Eser P, Schiessl H, Willnecker J (2004) Bone loss and steady state after spinal cord injury: a cross-sectional study using pQCT. J Musculoskel Neuron Interact 4:197–198
Russo CR, Laurentani F, Bandinelli S et al (2003) Aging bone in men and women: beyond changes in bone mineral density. Osteoporos Int 14:531–538
Ahlborg HG, Johnell O, Turner CH et al (2003) Bone loss and bone size after menopause. New Engl J Med 349:327–334
Hangartner TN, Gilsanz V (1996) Evaluation of cortical bone by computed tomography. J Bone Miner Res 11:1518–1525
Adami S, Gatti D, Braga V et al (1999) Site-specific effects of strength training on bone structure and geometry of ultradistal radius in postmenopausal women. J Bone Miner Res 14:120–124
Wilmet E, Ismail AA, Heilporn A et al (1995) Longitudinal study of the bone mineral content and of soft tissue composition after spinal cord section. Paraplegia 33:674–677
Taub E, Miller NE, Novack TA et al (1993) Technique to improve chronic motor deficit after stroke. Arch Phys Med Rehabil 74:347–354
Funding
MYCP was supported by a post-doctoral fellowship from Natural Sciences and Engineering Research Council of Canada. MCA was supported by a post-doctoral fellowship from the Michael Smith Foundation for Health Research. This study was supported by a grant-in-aid from the Heart Stroke Foundation of British Columbia and Yukon (JJE), and from career scientist awards from Canadian Institute of Health Research (JJE) and the Michael Smith Foundation for Health Research (JJE).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pang, M.Y.C., Ashe, M.C. & Eng, J.J. Muscle weakness, spasticity and disuse contribute to demineralization and geometric changes in the radius following chronic stroke. Osteoporos Int 18, 1243–1252 (2007). https://doi.org/10.1007/s00198-007-0372-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-007-0372-6