
Abstract
Introduction and hypothesis
Opioid use, addiction, and overdose are a growing epidemic in the USA. Our objective was to determine whether the amount of opioid medication prescribed following gynecologic and pelvic reconstructive surgery is insufficient, adequate, or in excess. We hypothesized that we were overprescribing postoperative opioids.
Methods
Participants who were at least 18 years old and underwent gynecologic and/or pelvic reconstructive surgery from April through August 2016 were eligible to participate. Routine practice for pain management is to prescribe 30 tablets of opioids for major procedures and ten to 15 tablets for minor procedures. At the 2-week postoperative visit, participants completed a questionnaire regarding the number of tablets prescribed and used, postoperative pain control, and relevant medical history. Fisher’s exact test was used to compare data.
Results
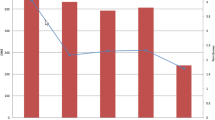
Sixty-five participants completed questionnaires. Half (49.1%) reported being prescribed more opioids than needed, while two (3.5%) felt the amount was less than needed. Though not significant, participants who underwent major surgeries were more likely to report being prescribed more than needed (53.5%) compared with participants who underwent minor surgeries (35.7%; p = 0.47). Though not significant, participants with anxiety were less likely to report being prescribed more tablets than needed compared with participants without anxiety (44.4% vs. 57.1%; p = 0.38). This was also true of participants with depression compared with those without (37.5% vs. 58.3%; p = 0.17), and those with chronic pain compared with those without (33.3% vs. 60.0%; p = 0.10).
Conclusions
Our current opioid prescription practice for postoperative pain management may exceed what patients need.
Similar content being viewed by others


References
Warner M, Chen LH, Makuc DM, Anderson RN, Miniño AM. Drug poisoning deaths in the United States, 1980–2008. NCHS data brief, no 81. Hyattsville: National Center for Health Statistics. p. 2011.
Center for Disease Control and Prevention. Addressing Prescription Drug Abuse in the United States. 2013:1–36. http://www.cdc.gov/HomeandRecreationalSafety/pdf/HHS_Prescription_Drug_Abuse_Report_09.2013.pdf.
García MC, Dodek AB, Kowalski T, et al. Declines in Opioid prescribing after a private insurer policy change — Massachusetts, 2011–2015. MMWR Morb Mortal Wkly Rep. 2016;65:1125–31.
Kennedy-Hendricks A, Andrea G, McDonald E, McGinty EE, Shields W, Barry CL. Medication sharing, storage, and disposal practices for Opioid medications among US adults. JAMA Intern Med. 2016;176(7):1027–8.
Bates C, Laciak R, Southwick A, Bishoff J. Overprescription of postoperative narcotics: a look at postoperative pain medication delivery, consumption and disposal in urological practice. J Urol. 2011;185(2):551–5.
United States Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. Center for Behavioral Health Statistics and Quality. National Survey on Drug Use and Health, 2013. ICPSR35509-v3. Ann Arbor, MI: Inter-university Consortium for Political and Social Research [distributor], 2015–11-23.
Centers for Disease Control and PreventionPublic Health Service U S Department of Healath and Human Services. Guideline for prescribing Opioids for chronic pain. J Palliat Care Parmacothera. 2016;30(2):138–40.
Swenson CW, Kelley AS, Fenner DE, Berger MB. Outpatient narcotic use after minimally invasive Urogynecologic surgery. Female Pelvic Med Reconstr Surg. 22(5):377–81.
Bartels K, Mayes LM, Dingmann C, Bullard KJ, Hopfer CJ, BinswangerI A. Opioid use and storage patterns by patients after hospital discharge following surgery. PLoS One. 2016;11(1):e0147972.
Taenzer P, Melzack R, Jeans ME. Influence of psychological factors on postoperative pain, mood and analgesic requirements. Pain. 1986;24(3):331–42.
Hylan TR, Von Korff M, Saunders K, et al. Automated prediction of risk for problem opioid use in a primary care setting. J Pain. 2015;16(4):380–7.
Javier A, Briana C, Yueqin H, Krista J, Krista H. Evaluation of how depression and anxiety mediate the relationship between pain catastrophizing and prescription opioid misuse in a chronic pain population. Pain Med. 2016;17(2):295–303.
Wilsey BL, Fishman SM, Tsodikov A, Ogden C, Symreng I, Ernst A. Psychological comorbidities predicting prescription opioid abuse among patients in chronic pain presenting to the emergency department. Pain Med. 2008;9(8):1107–17.
Funding
This work was conducted with support from Harvard Catalyst | The Harvard Clinical and Translational Science Center (National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health Award UL1 TR001102) and financial contributions from Harvard University and its affiliated academic healthcare centers.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest.
Additional information
Presentation
2017 Society of Gynecologic Surgeons Annual Scientific Meeting, San Antonio, TX, USA, 27 March 2017.
Rights and permissions
About this article

Cite this article
Hota, L.S., Warda, H.A., Haviland, M.J. et al. Opioid use following gynecologic and pelvic reconstructive surgery. Int Urogynecol J 29, 1441–1445 (2018). https://doi.org/10.1007/s00192-017-3474-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-017-3474-5