
Abstract
Background:
Patients with bowel injuries resulting from blunt abdominal trauma show no reliable clinical or radiologic signs on initial examination. The mechanism of injury is the only element of some diagnostic value. Intestinal injury may be evaluated by ultrasonography (US), plain abdominal radiographs, computed tomography (CT), and diagnostic laparoscopy. This paper is a retrospective study of diagnostic procedures used in 45 consecutive patients with bowel injuries who presented at our center between October 1996 and December 2001.
Patients and Methods:
Of 45 patients (mean age 40 years), nine suffered isolated bowel injuries and 36 presented with concomitant injuries. The mechanism of trauma was traffic accident in 30 of 45 patients (in 16 of these 30 patients compression by a seat belt), strong blow to the abdomen in eight, fall from a height in five, and other causes in two patients. US was done in 43 of 45 patients, plain abdominal radiographs in 22, CT in six, peritoneal lavage in one, and diagnostic laparoscopy in one.
Results:
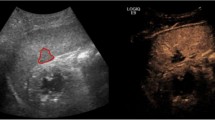
37 of 43 patients were evaluated by US immediately upon arrival; in four patients there was a delay in diagnosis of 1 day, and in two patients a delay of several days. At initial sonography, free intraperitoneal fluid was identified in 32 of the 43 patients; in most of them (n = 15) the amount of free fluid was rather small. Free fluid was absent in eleven of 43 patients; yet seven of these eleven patients demonstrated free fluid upon repeat examination.
In nine of 32 patients, an increased amount of free fluid was identified upon repeat examination. Two of 43 patients, evaluated 3 and 9 days after arrival, respectively, showed dense intraperitoneal fluid, suggestive of peritonitis. US identified intestinal injuries in 14 of 43 patients; in all of them, the diagnosis was established upon repeat examination or delayed initial examination. Radiographs were performed in 22 of 45 patients (18 of them suffering perforation) and verified the pneumoperitoneum in nine of 18 patients with perforation. CT scanning identified intestinal injury in four of six patients. 17 of 45 patients were operated immediately in the Surgical Emergency Unit, 15 patients in the first 24 h, eight patients 2 days after admission, and five patients > 2 days (max. 9 days) after admission. In our series of 45 patients, there were four deaths, and only two (4.4%) were associated with bowel injury.
Conclusion:
In patients presenting with a typical mechanism of trauma and an abdominal bruise, plain radiographs should be taken in addition to initial US to identify the presence of free air. In patients with negative radiologic and US findings and in those demonstrating a small quantity of free fluid, US scanning should be repeated soon after the initial evaluation and, if necessary, a CT scan should be taken. The use of laparoscopy is indicated in unclear cases. According to our experience, a judicious and timely decision for laparotomy can only be based on the combination of the mechanism of injury, clinical picture, and results of properly planned diagnostic tests.
Similar content being viewed by others


Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vidmar, D., Pleskovic, A. & Tonin, M. Diagnosis of Bowel Injuries from Blunt Abdominal Trauma. Eur J Trauma 29, 220–227 (2003). https://doi.org/10.1007/s00068-003-1260-1
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s00068-003-1260-1