
Abstract
We present a two-phase model for a staff planning problem in a surgical department. We consider the setting where staff, in particular nurse circulators and surgical scrub technicians, are assigned to one of different service lines, and while they can be ‘pooled’ and temporally assigned to other service line if needed, these re-assignments should belimited. In Phase I, we decide on the number of staff hours to budget for each service line, considering policies limiting staff pooling and overtime, and different demand scenarios. In Phase II, we determine how these budgeted staff hours should be allocated across potential work days and shifts, given estimated staff requirements and shift-related scheduling restrictions. We propose a heuristic to speed the model’s Phase II solution time. We implement the model using a hospital’s surgical data and compare the model’s results with the hospital’s current practices. Using a simulation model for the surgical operations, we find that our two-phase model reduces the delays caused by staff unavailability as well as staff pooling, without increasing the workforce size. Finally, we briefly describe a decision-support tool we developed with the objective of fine-tuning staff planning decisions.











Similar content being viewed by others

References
Agnihothri S, Taylor P (1991) Staffing a centralized appointment scheduling department in lourdes hospital. Interfaces 21:1–11
Alfares HK (1998) An efficient two-phase algorithm for cyclic days-off scheduling. Comput Oper Res 25(11):913–923
Alfares HK (2004) Survey, categorization, and comparison of recent tour scheduling literature. Ann Oper Res 127(1-4):145– 175
Baker K (1974) Scheduling a full-time workforce to meet cyclic staffing requirements. Manag Sci 20:1561–1568
Baker K (1977) Workforce scheduling with cyclic demands and day-off. Manag Sci 24:161–167
Bard JF (2004) Staff scheduling in high volume service facilities with downgrading. IIE Trans 36(10):985–997
Bard JF (2010) Nurse scheduling models. Wiley Encyclopedia of Operations Research and Management Science, pp 3617– 3627
Bard JF, Binici C, desilva AH (2003) Staff scheduling at the united states postal service. Comput Oper Res 30(5):745–771
Bard JF, Morton DP, Wang YM (2007) Workforce planning at usps mail processing and distribution centers using stochastic optimization. Ann Oper Res 155:51–78
Bard JF, Purnomo HW (2005) A column generation-based approach to solve the preference scheduling problem for nurses with downgrading. Socio Econ Plan Sci 39(3):193–213
Bard JF, Wan L (2005) Weekly scheduling in the service industry: an application to mail processing and distribution centers. IIE Trans 37(5):379–396
Beaumont N (1997) Scheduling staff using mixed integer programming. Eur J Oper Res 98(3):473–484
van den Bergh J, Belin J, Bruecker PD, Demeulemeester E, Boeck LD (2013) Invited review: Personnel scheduling: A literature review. Eur J Oper Res
Brunner JO, Edenharter GM (2011) Long term staff scheduling of physicians with different experience levels in hospitals using column generation. Health Care Manag Sci 14(2):189– 202
Brusco M, Jacobs L (2001) Starting-time decisions in labor tour scheduling: An experimental analysis and case study. Eur J Oper Res 131:459–475
Burns R, Carter M (1985) Work force size and single shift schedules with variable demands. Manag Sci 31(5):599–607
Camm JD, Magazine MJ, Polak GG, Zaric GS (2008) Scheduling parallel assembly workstations to minimize a shared pool of labor. IIE Trans 40(8):749–758
Cardoen B, Demeulemeester E, Belien J (2010) Operating room planning and scheduling: a literature review. Eur J Oper Res 201:921–932
Cezik T, Gunluk O, Luss H (2001) An integer programming model for the weekly tour scheduling problem. Nav Res Logist 48
Chung J, White K (2008) Cross-trained versus specialized agents in an inbound call centre: a simulation-based methodology for trade-off analysis. J Simul 2(3):162–169
Cochran J, Chu D, Chu M (2001) Optimal staffing for cyclically scheduled processes. Int J Prod Res 35:3393–3403
Dexter F (2013) Operating room staffing and allocation. http://www.franklindexter.net/Lectures/ORStaffingTalk.pdf
Dexter F, Epstein RH (2003) Optimizing second shift or staffing. AORN J 77(4):825–830
Dexter F, Epstein RH (2006) Holiday and weekend operating room on-call staffing requirements. Anesth Analg 103(6):1494–1498
Dexter F, Epstein RH, Marcon E, Ledolter J (2005) Estimating the incidence of prolonged turnover times and delays by time of day. Anesth 102(6):1242–1248
Dexter F, Epstein RH, Traub RD, Xiao Y (2004) Making management decisions on the day of surgery based on operating room efficiency and patient waiting times. Anesth 101:1444–1453
Dexter F, Macario A (1996) Applications of information systems to operating room scheduling. Anesth 85(6):1232–1234
Dexter F, Macario A, Epstein RH, Ledolter J (2005) Validity and usefulness of a method to monitor surgical services average bias in scheduled case durations. Can J Anesth 52(9):935–939
Dexter F, Macario A, ONeill L (2000) Scheduling surgical cases into overflow block timecomputer simulation of the effects of scheduling strategies on operating room labor costs. Anesth Analg 90(4):980–988
Dexter F, Macario A, Qian F, Traub RD (1999) Forecasting surgical groups total hours of elective cases for allocation of block time: application of time series analysis to operating room management. Anesth 91(5):1501
Dexter F, O’Neill L (2001) Weekend operating room on call staffing requirements. AORN J 74(5):664–671
Dexter F, Traub RD (2000) The lack of systematic month-to-month variation over one-year periods in ambulatory surgery caseloadapplication to anesthesia staffing. Anesth Analg 91(6):1426–1430
Di Gaspero L, Gartner J, Kortsarz G, Musliu N, Schaerf A, Slany W (2007) The minimum shift design problem. Ann Oper Res 155(1):79–105
Easton FF (2011) Cross-training performance in flexible labor scheduling environments. IIE Trans 43(8):589–603
Ernst A, Jiang H, Krishnamoorthy M, Owens B, Sier D (2004) An annotated bibliography of personnel scheduling and rostering. Ann Oper Res 127:21–144
Ernst AT, Jiang H, Krishnamoorthy M, Sier D (2004) Staff scheduling and rostering: a review of applications, methods and models. Eur J Oper Res 153(1):3–27
Fry MJ, Magazine MJ, Rao US (2006) Firefighter staffing including temporary absences and wastage. Oper Res 54 (2):353–365
Gupta D (2007) Surgical suites’ operations management. Prod Oper Manag 16(6):689–700
Ingolfsson A, Haque A, Umnikov A et al (2002) Accounting for time-varying queueing effects in workforce scheduling. Eur J Oper Res 139(3):585–597
Jordan WC, Inman RR, Blumenfeld DE (2004) Chained cross-training of workers for robust performance. IIE Trans 36(10):953–967
Li LLX, King BE (1999) A healthcare staff decision model considering the effects of staff cross-training. Health Care Manag Sci 2(1):53–61
Maenhout B, Vanhoucke M (2013) An integrated nurse staffing and scheduling analysis for longer-term nursing staff allocation problems. Omega 41(2):485–499
Masursky D, Dexter F, OLeary CE, Applegeet C, Nussmeier NA (2008) Long-term forecasting of anesthesia workload in operating rooms from changes in a hospitals local population can be inaccurate. Anesth Analg 106(4):1223–1231
McIntosh C, Dexter F, Epstein RH (2006) The impact of service-specific staffing, case scheduling, turnovers, and first-case starts on anesthesia group and operating room productivity: a tutorial using data from an australian hospital. Anesth Analg 103(6):1499–1516
Moore IC, Strum DP, Vargas LG, Thomson DJ (2008) Observations on surgical demand time series: detection and resolution of holiday variance. Anesth 109(3):408–416
Morris JG, Showalter MJ (1983) Simple approaches to shift, days-off and tour scheduling problems. Manag Sci 29(8):942–950
van Oostrum JM, Bredenhoff E, Hans EW (2010) Suitability and managerial implications of a master surgical scheduling approach. Ann Oper Res 178:91–104
van Oostrum JM, Van Houdenhoven M, Vrielink MM, Klein J, Hans EW, Klimek M, Wullink G, Steyerberg EW, Kazemier G (2008) A simulation model for determining the optimal size of emergency teams on call in the operating room at night. Anesth Analg 107(5):1655–1662
Sayın S, Karabatı S (2007) Assigning cross-trained workers to departments: a two-stage optimization model to maximize utility and skill improvement. Eur J Oper Res 176(3):1643–1658
Shapiro A, Homem-de Mello T (2000) On the rate of convergence of optimal solutions of monte carlo approximations of stochastic programs. SIAM J Optim 11(1):70–86
Sinreich D, Jabali O (2007) Staggered work shifts: a way to downsize and restructure an emergency department workforce yet maintain current operational performance. Health Care Manag Sci 10(3):293–308
Viapiano J, Ward DS (2000) Operating room utilization: the need for data. Int Anesthesiol Clin 38(4):127–140
Vohra RV (1987) The cost of consecutivity in the (5, 7) cyclic staffing problem. IIE Trans 19(3):296–299
Walters E (2009) Two sample kolmogorov-smirnov test of the underyling distributions code. http://www.minitab.com/
Wang J, Quan S, Li J, Hollis AM (2012) Modeling and analysis of work flow and staffing level in a computed tomography division of university of wisconsin medical foundation. Health Care Manag Sci 15(2):108–120
Acknowledgments
This research was supported in part by a gift from University Hospital in Augusta, GA. We also thank Stanley Bartlett, Marilyn Bowcutt, Lisa Jackson, Christine Martin, Susan McMillan and Jonathan Turner from the University Hospital.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix A: Phase II formulation when a staff member can be assigned to different shift lengths
In the Phase II original formulation (Section 3.2), we assume that a full-time staff member should be assigned to only one type of shift length l, each week. If we only assume that full-time staff should work an average number of hours per week, say H r, we can drop the index l in Z s,l and introduce the following parameters and variables:
-
Average number of regular time hours per week per staff member
-
Number of full-time staff assigned to service line s
We replace constraints (17), (18), and (19) with constraints (35), (36), (37).
Constraints (35) are necessary conditions for full-time staff not be scheduled more than H r hours per week on average, during regular time. This means no more than \(\frac {H^{r}}{8}\) shifts per week, per full-time staff member, since full-time shifts are at least 8 hours long.
Appendix B: Other model parameters for the two-phase ORs staffing model
We define the remaining of the parameters for the two-phase ORs staffing model based on the hospital’s current processes and practices. These parameters include:
Phase I
-
The standard number of hours per FTE per week is H std = 40, and the effective number of hours is H e = 37.5.
-
Staff hours in excess of 40 hours per FTE per week are paid at an overtime rate. Overtime is paid at a 1.5 rate with respect of regular time, i.e., \(C^{o}_{s}= 1.5C^{r}_{s}\).
-
The costs to hire and to fire are \(C^{h}_{s}=0\) and \(C^{f}_{s}=0\). The initial workforce size is assumed to be zero \((X^{0}_{s}=0)\).
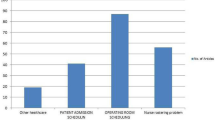
Since we do not have a value for the hospital’s maximum fractions of overtime and pooling, we define these parameters so that the resulting permanent FTEs (X s ) would be similar to those implemented by the hospital for the same planning horizon, with the goal of making results more comparable. The baseline for the number of permanent FTEs for both circulators and scrub techs is obtained from the hospital’s staffing in December 2012. The staffing budget and structure do not change much throughout a year, so we believe that this is a reasonable approximation of the original staff planning decisions for 2012. Even if this was not the case, Phase I makes decisions by considering about the same or less information (i.e., historical data available prior to July 2011) compared to that available to the hospital’s OR manager when the initial staffing decisions are made. In December 2012, the number of FTEs for scrub techs and circulators were 23.8 and 20.7, respectively. We test different maximum pooling and overtime settings to match these numbers of FTEs. Using CPLEX, we run Phase I for circulators with 30 demand scenarios for a 48-weeks planning horizon in 2012 assuming that no pooling or overtime is allowed. We arrive to approximately the same number of permanent FTEs as the hospital, so we keep the zero pooling and no overtime assumption. Similarly, we run Phase I for scrub techs and look for pooling and overtime settings that would give similar results to those implemented by the hospital. In Fig. 12 we see that 23.8 FTEs (the hospital’s budget) result from a maximum average overtime \((\bar {\alpha }^{o}_{s} \cdot 100~\%)\) of 0.7 % and a maximum average pooling \((\bar {\alpha }^{p}_{s} \cdot 100~\%)\) of 0.0 %, or 0.2 % and 10 % respectively. We select the latter setting, when overtime is lower.

Number of FTEs obtained from Phase I, under different settings for the maximum average percentage of pooling and overtime
-
Shifts can start every 30 minutes from 6:00 AM to 2:30 PM, every day of the week. There are five shift lengths: {5, 8, 9, 10, 12}.
-
There is a pre-fixed night shift from 7:00 PM to 6:30 AM with a minimum staffing requirement of one circulator and two scrub techs. Including this night shift, there are 91 potential shifts (N J = 91).
-
The less-than-full-time hours fraction \((\alpha ^{lf}_{s})\) is limited to 0.04 of effective permanent FTEs hours for scrub techs and zero for circulators.
-
The part-time hours fraction \((\alpha ^{pt}_{s})\) is limited to 0.22 of effective permanent FTEs hours for circulators and scrub techs.
-
We use the staffing levels from week 28 in 2010 to week 27 in 2011 as an estimate for the staffing levels during the first 48 weeks of 2012 (the planning horizon).
-
The penalty for unmet staffing level by service line is constant for all time buckets and all service lines (Π s,t = 1).
-
An additional 0.5 penalty \(({\Pi }^{\prime }_{t}=0.5)\) is incurred for overall unmet staffing levels.
Appendix C: OR simulation
We build the simulation model using Arena. Figure 13 shows a snapshot of the Arena model, with the identification of the main parts:
-
Read staff schedule: This module reads a file with the number of available staff at any time for each service line, based on the staffing structure under consideration.
-
Read cases information: This module reads a file with the surgical cases information and times.
-
Patient arrival and paperwork: This module generates patient arrivals according to the arrival time distributions. After a patient’s arrival, paperwork is completed at reception. The patient is prepared for surgery when the estimated procedure start time is closer (<2 hours).
-
Blood drawn and assessment: Blood may be drawn, and the patient is assessed by a nurse.
-
Waiting for scheduled time and OR: The patient waits for the scheduled procedure start time if it is the first case for the OR, the anesthesiologist, or the surgeon; otherwise, the patient waits for the OR to be ready.
-
Seize anesthesia and OR staff: The case patient seizes the required anesthesia and OR staff. OR staff assigned to the case’s service line is chosen first if available, if not, OR staff form other service lines can be pooled and used.
-
Procedure: The patient is taken to the OR and the surgical procedure starts. The patient is taken out of the room after the procedure is completed.
-
Room turnover: The OR is cleaned and prepared for the next case by the patient care assistants and the OR staff.
-
Write output: This module writes the surgical case time stamps in a file for analysis.

Arena simulation snapshot
To obtain the time distribution for the patient’s arrival relative to the case scheduled start time, the percentage of cases with blood being drawn, and the patient assessment and preparation time distributions, we use a 16-days time study done in November 2010 that includes the time stamps of the more than 280 OR patients from their arrival to the end of their preparation for the surgical procedure. We link these time stamps with data provided by the surgical information system, including the type of patient and procedure, the scheduled start and end times for the case, and the patient’s wheels-in and -out times. The cases assigned OR, sequence, and actual duration are taken directly from the surgical data. All the time distribution fittings are done using Expert Fit. If there is not a distribution with a good fit, an empirical distribution based on the available data is used. We use empirical time distributions for outpatients and inpatients paperwork, blood work and nurse assessment, and for outpatients arrival time; and we fit a Normal distribution (AD p-value > 0.25) for inpatients arrival time. We use the surgical data from 2009 and 2010 to calculate the turnover time distributions by case type. We assume that the turnover for a case starts at the wheels-out of the previous patient in the room and ends with the wheels-in of the new patient. Only the turnover for cases with some delay are considered, so that the case waiting time for its scheduled start time is not included in the calculation. Table 12 shows the best fitted distributions for each case type. AD p-values > 0.25 and KS p-values > 0.15, for all case types (except for Colon-Rectal, with a KS p-value > 0.10).
1.1 C.1 OR Simulation Validation
To validate the simulation, we analyze the simulation results given the hospital’s CP staffing structure and compare them with the actual surgical data for the planning horizon, i.e, the first 48 weeks of 2012. In particular, we look at the percentage of delayed cases and an OR last wheels-out time of the day, since these statistics reflect the surgical schedule characteristics and the resource availability dynamics.
According to surgical data, the percentage of delayed cases (those cases for which the wheels-in occurs 10 minutes or later after the scheduled time) is 42.4 %, whereas according to the simulation this percentage is 41.6 %, a non-statistically significant difference of 0.8 % (Fisher’s exact test p-value > 0.31). The average OR last wheels-out time in a day (for those days with more than 5 ORs open) is 3:37PM according to surgical data and 3:30PM according to the simulation, a non-statistically significant difference of 7 minutes (two-sample t-test with p-vale > 0.65). The average OR last wheels-out time distributions for the actual surgical data and the simulation results are shown in Fig. 14. We perform a KS 2-sample test under the null hypothesis that these distributions are not different. According to this test there is not sufficient evidence to reject this hypothesis at a 95 % confidence.

Simulated and actual average OR last wheels-out empirical distribution functions
Appendix D: A decision-support tool
We developed a decision-support tool with the objective of helping the OR manager to make adjustments to the staff budget and the staffing structure by: reassigning staff to another service line, changing the number of people assigned to a shift, adding a new shift, etc. The tool was implemented using Microsoft Excel, and it was automated for ease of use.
Tool Input
-
Historical surgical data (from automatic reports from the surgical information system).
-
Current staffing structure.
-
Classification of surgical services to one of the three service lines.
-
OR staff requirements per case type.
-
User can select: time baseline, staff type, one or a group of ORs.
Tool Output
-
Budget by service line and staff type.
-
Weekly volume trends by service line, compared with the budget. See Fig. 15.
-
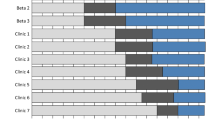
Current staffing levels vs. observed demand patterns, overall and by service line. See Fig. 16.

Weekly volume trends by service line in OR staff hours

Staffing levels of circulators compared with the demand patterns for all service lines
Although this tool does not make automated staff planning decisions (it is not integrated with Phase I and Phase II yet), it gives useful statistics and graphs based on easily available surgical data, which are helpful to analyze and fine-tune previous decisions. For example, if the OR manager observes that the demand of a particular service line exhibits a decreasing trend, and the demand of another service line increases, he/she can reassign staff. Similarly, if the aggregated demand trend is increasing, the manager can request an increase in the total FTEs budget. Also, if the demand patterns suggest that a service line may be overstaffed on one day and understaffed on another, the OR manager can restructure shifts.
Rights and permissions
About this article

Cite this article
Villarreal, M.C., Keskinocak, P. Staff planning for operating rooms with different surgical services lines. Health Care Manag Sci 19, 144–169 (2016). https://doi.org/10.1007/s10729-014-9307-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10729-014-9307-x