
Abstract
Background: Stereotactic core biopsy of mammographically defined breast abnormalities is an alternative to wire localization biopsy. The purpose of this study was to evaluate the extent of lumpectomy in patients diagnosed by stereotactic core versus wire localization biopsy.
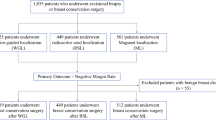
Methods: A total of 67 consecutive patients diagnosed with invasive cancers or ductal carcinoma in situ (DCIS) were retrospectively reviewed. Thirty-four were diagnosed by core biopsy and the remaining 33 by wire localization biopsy.
Results: Approximately 65% of patients subsequently had breast-conserving surgical therapy. Seventy-nine percent of patients undergoing wire localization biopsies had positive surgical margins. Achievement of negative surgical margins for lumpectomies performed after wire localization or stereotactic core biopsies was 100% and 89%, respectively, which was not significantly different. However, the total volume of breast tissue removed for breast conservation in patients undergoing lumpectomy after wire localization versus core biopsies was 183 cm3 and 104 cm3, respectively, which was significantly different (P = .003).
Conclusions: Diagnosis by stereotactic core biopsies resulted in less tissue removal to achieve margin-negative lumpectomies for breast conservation. Stereotactic core biopsy is the method of choice for biopsying nonpalpable, suspicious breast lesions.
Similar content being viewed by others
REFERENCES
Yim JH, Barton P, Weber B, et al. Mammographically detected breast cancer. Benefits of stereotactic core versus wire localization biopsy. Ann Surg 1996;6:688–697.
Osteen RT, Cady B, Chmiel JS, et al. 1991 national survey of carcinoma of the breast by the Commission on Cancer. J Am College of Surg 1994;3:213–219.
Bear HD. Image-guided breast biopsy—how, when, and by whom? (Guest Editorial). J Surg Onc 1997;67:1–5.
Parker SH, Lovin JD, Jube WE, Luethke JM, Hopper KD, Yakes WF, Burke BJ. Stereotactic breast biopsy with a biopsy gun. Radiol 1990;176:741–747.
Doyle AJ, Murray KA, Nelson EW, Bragg DG. Selective use of image-guided large-core needle biopsy of the breast: Accuracy and cost-effectiveness. Am J Radiol 1995;2:281–284.
Berg WA, Krebs TL, Campassi C, Magder LS, Sun CC. Evaluation of 14- and 11-gauge directional, vacuum-assisted biopsy probes and 14-gauge biopsy guns in a breast parenchymal model. Radiol 1997;1:203–208.
Liberman L, LaTrenta LR, Dershaw DD, et al. Impact of core biopsy on the surgical management of the impalpable breast cancer. Am J Radiol 1997;2:495–499.
Parker SH, Burbank F, Jackman RJ, et al. Percutaneous large-core breast biopsy: a multi-institutional study. Radiol 1994;2:359–364.
Nguyen M, McCombs MM, Ghandehari S, et al. An update on core needle biopsy for radiologically detected breast lesions. Cancer 1996;11:2340–2345.
American College of Radiology (ACR). Breast imaging reporting and data system (BI-RADS™). 2nd ed. Reston, VA: American College of Radiology, 1995.
Morrow M. Management of nonpalpable breast lesions. Prin Pract Oncol Updates 1990;4:1–11.
Morrow M, Schmidt R, Cregger B, Hassett C, Cox S. Preoperative evaluation of abnormal mammographic findings to avoid unnecessary breast biopsies. Arch Surg 1994;10:1091–1096.
Sullivan DC. Needle core biopsy of mammographic lesions. Am J Radiol 1994;3:601–608.
Liberman L, Dershaw DD, Rosen PP, Cohen MA, Hann LE, Abramson AF. Stereotaxic core biopsy of impalpable spiculated breast masses. Am J Radiol 1995;3:551–554.
Whitten TM, Wallace TW, Bird RE, Turk PS. Image-guided core biopsy has advantages over needle localization biopsy for the diagnosis of nonpalpable breast cancer. Am Surgeon 1997;12:1072–1077.
Cross MJ, Evans WP, Peters GN, Cheek JH, Jones RC, Krakos P. Stereotactic breast biopsy as an alternative to open excisional biopsy. Ann Surg Onc 1995;3:195–200.
Ngai JH, Zelles GW, Rumore GJ, Sawicki JE, Godfrey RS. Breast biopsy techniques and adequacy of margins. Arch Surg 1991;126:1343–1347.
Cox CE, Ku NN, Reintgen DS, Greenberg HM, Nicosia SV, Wangensteen S. Touch preparation cytology of breast lumpectomy margins with histologic correlation. Arch Surg 1991;126:490–493.
Balch CM. The needle biopsy should replace open excisional biopsy... but will the surgeon’s role in coordinating breast cancer be diminished? (Editorial). Ann Surg Onc 1995;3:191–192.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Al-Sobhi, S.S., Helvie, M.A., Pass, H.A. et al. Extent of Lumpectomy for Breast Cancer After Diagnosis by Stereotactic Core Versus Wire Localization Biopsy. Ann Surg Oncol 6, 330–335 (1999). https://doi.org/10.1007/s10434-999-0330-y
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s10434-999-0330-y