
Abstract
Background
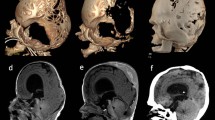
The authors described their surgical technique for scaphocephaly in relatively older infants who are 5 months old or over. The technique is a kind of hybrid of distraction osteogenesis utilizing skull expanders and a traditional cranial reconstruction procedure.
Surgery
The surgery usually consists of four procedures. The first is to make strip craniotomy over the superior sagittal sinus (SSS) from the major fontanelle to the minor one. The second is the occipital craniotomy for the occipital bossing. The occipital bone flap undergoes barrel stave osteotomy and is repositioned later. The third is placement of skull expander for distraction osteogenesis. Bidirectional small strip craniotomy is made along the coronal and lambdoid sutures, then transverse cutting is added to make a hinge point near the base of the parietal bone. Two to three skull expanders are placed crossing the SSS. The last procedure is radial-oriented osteotomy on the dorsal end of frontal bone to meet the elevated, expanded parietal bone. Skull expansion starts within a week with 5 mm/week base up to 20 to 30 mm. Exposed shafts of the expander are cut at the end of skull expansion.
Discussion
Process of osteogenesis is followed at an outpatient clinic, and the expanders are removed 4 to 6 months later after confirming the sufficient ossification. An advantage of our procedure is that maximum skull expansion is possible with minimum regression after distraction osteogenesis in the long term. Limited craniotomy enables limited blood loss. The skin trouble caused by stretching can be avoided. No postoperative helmet is required. A disadvantage is that the procedure leaves a foreign body on the skull for several months and requires additional surgery for removal.
Access this article
We’re sorry, something doesn't seem to be working properly.
Please try refreshing the page. If that doesn't work, please contact support so we can address the problem.






Similar content being viewed by others


References
Hirabayashi S, Sugawara Y, Sakurai A, Harii K, Par S (1998) Frontoorbital advancement by gradual distraction. Technical note. J Neurosurg 89:1058–1061
Ilizarov GA (1989) The tension-stress effect on the genesis and growth of tissues. Part 1. The influence of stability of fixation and soft-tissue preservation. Clin Orthop 238:249–281
McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH (1992) Lengthening the human mandible by gradual distraction. Plast Reconstr Surg 89:1–8
Imai K, Komune H, Toda C, Nomachi T, Enoki E, Sakamoto H, Kitano S, Hatoko M, Fujimoto T (2002) Cranial remodeling to treat craniosynostosis by gradual distraction using a new device. J Neurosurg 96:654–659
Komuro Y, Yanai A, Hayashi A, Nakanishi H, Miyajima M, Arai H (2005) Cranial reshaping employing distraction and contraction in the treatment of sagittal synostosis. Br J Plast Surg 58:196–201
Takagi T, Morota N, Ihara S, Kaneko T (2011) Anthropometric outcome of sagittal craniosynostosis following surgery. Shoni No No Shinkei 36:20–25
Chieffo D, Tamburrini G, Massimi L, Di Giovanni S, Giansanti C, Caldarelli M, Di Rocco C (2010) Long-term neuropsychological development in single-suture craniosynostosis treated early. J Neurosurg Pediatrics 5:232–237
Bellew M, Liddington M, Chumas P, Russell J (2011) Preoperative and postoperative developmental attainment in patients with sagittal synostosis: 5-year follow-up. J Neurosurg Pediatris 7:121–126
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morota, N., Ogiwara, H. & Kaneko, T. Hybrid surgery for scaphocephaly with distraction osteogenesis using skull expanders: technical note. Childs Nerv Syst 28, 1353–1358 (2012). https://doi.org/10.1007/s00381-012-1810-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-012-1810-0