
Abstract
Objective
To determine the effect of different mattresses on cardiopulmonary resuscitation performance and establish whether emergency deflation of an inflatable mattress improves the quality of resuscitation.
Design and setting
Randomised controlled cross-over trial performed in a general ICU
Participants
Critical care staff from a general ICU.
Interventions
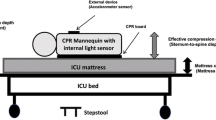
Cardiopulmonary resuscitation on a manikin on the floor or on a bed with a standard foam mattress and inflated and deflated pressure redistributing mattresses. Maximal compression force was measured at different bed heights.
Measurements and results
Compression depth, duty cycle and rate and percentage correct expired air ventilation were recorded on a manikin. Compression depth was significantly lower on the foam (35.2 mm), inflated (37.2 mm) and deflated mattress (39.1 mm) than the floor (44.2 mm). There were no clinically important differences in duty cycle or compression rate. The quality of ventilation was poor on all surfaces. Maximal compression force declined as bed height increased.
Conclusions
Resuscitation performance is adversely affected when performed on a bed (irrespective of mattress type) compared to the floor. There were no differences between the inflated and deflated mattresses, although the deflation process did not adversely affect performance. This study does not support the routine deflation of an inflated mattress during resuscitation and questions the potential benefits from using a backboard. The finding that bed height affects maximal compression forces, challenges the recommendation that cardiopulmonary resuscitation be performed with the bed at middle-thigh level and requires further investigation.


Similar content being viewed by others

Reference
Franklin C, Mathew J (1994) Developing strategies to prevent in hospital cardiac arrest: analyzing responses of physicians and nurses in the hours before the event. Crit Care Med 22:244–247
Keller BPJA, Wille J, Ramshorst B, Werken C (2002) Pressure ulcers in intensive care patients: a review of risks and prevention. Intensive Care Med 28:1379–1388
European Resuscitation Council (2000) Adult basic life support. III. Resuscitation 46:29–71
Wik L, Myklebust H, Auestad BH, Steen PA (2002) Retention of basic life support skills 6 months after training with an automated voice advisory manikin system without instructor involvement. Resuscitation 52:273–279
Resuscitation Council (2000) Guidance for safer handling during resuscitation in hospital. Resuscitation Council, London
Tweed M, Tweed C, Perkins GD (2001) The effect of differing support surfaces on the efficacy of chest compressions using a resuscitation manikin model. Resuscitation 51:179–183
Robertson C, Holmberg S (1992) Compression techniques and blood flow during cardiopulmonary resuscitation. A statement for the Advanced Life Support Working Party of the European Resuscitation Council. Resuscitation 24:123–132
Wik L, Steen PA, Bircher NG (1994) Quality of bystander cardiopulmonary resuscitation influences outcome after prehospital cardiac arrest. Resuscitation 28:195–203
Maier GW, Newton JR Jr, Wolfe JA, Tyson GS Jr, Olsen CO, Glower DD, Spratt JA, Davis JW, Feneley MP, Rankin JS (1986) The influence of manual chest compression rate on hemodynamic support during cardiac arrest: high-impulse cardiopulmonary resuscitation. Circulation 74:IV51–IV59
Babbs CF, Thelander K (1995) Theoretically optimal duty cycles for chest and abdominal compression during external cardiopulmonary resuscitation. Acad Emerg Med 2:698–707
Babbs CF, Voorhees WD, Fitzgerald KR, Holmes HR, Geddes LA (1983) Relationship of blood pressure and flow during CPR to chest compression amplitude: evidence for an effective compression threshold. Ann Emerg Med 12:527–532
Bellamy RF, DeGuzman LR, Pedersen DC (1984) Coronary blood flow during cardiopulmonary resuscitation in swine. Circulation 69:174–180
Wik L, Naess PA, Ilebekk A, Nicolaysen G, Steen PA (1996) Effects of various degrees of compression and active decompression on haemodynamics, end-tidal CO2, and ventilation during cardiopulmonary resuscitation of pigs. Resuscitation 31:45–57
Wolfe JA, Maier GW, Newton JR Jr, Glower DD, Tyson GS Jr, Spratt JA, Rankin JS, Olsen CO (1988) Physiologic determinants of coronary blood flow during external cardiac massage. J Thorac Cardiovasc Surg 95:523–532
Ornato JP, Levine RL, Young DS, Racht EM, Garnett AR, Gonzalez ER (1989) The effect of applied chest compression force on systemic arterial pressure and end-tidal carbon dioxide concentration during CPR in human beings. Ann Emerg Med 18:732–737
Levine RL, Wayne MA, Miller CC (1997) End-tidal carbon dioxide and outcome of out-of-hospital cardiac arrest. N Engl J Med 337:301–306
Boe JM, Babbs CF (1999) Mechanics of cardiopulmonary resuscitation performed with the patient on a soft bed vs a hard surface. Acad Emerg Med 6:754–757
Larsen PD, Perrin K, Galletly DC (2002) Patterns of external chest compression. Resuscitation 53:281–287
Hightower D, Thomas SH, Stone CK, Dunn K, March JA (1995) Decay in quality of closed-chest compressions over time. Ann Emerg Med 26:300–303
Wenzel V, Keller C, Idris AH, Dorges V, Lindner KH, Brimacombe JR (1999) Effects of smaller tidal volumes during basic life support ventilation in patients with respiratory arrest: good ventilation, less risk? Resuscitation 43:25–29
Dorges V, Ocker H, Wenzel V, Sauer C, Schmucker P (2001) Emergency airway management by non-anaesthesia house officers-a comparison of three strategies. Emerg Med J 18:90–94
Clayton TJ, Pittman JA, Gabbott DA (2001) A comparison of two techniques for manual ventilation of the lungs by non-anaesthetists: the bag-valve-facemask and the cuffed oropharyngeal airway (COPA) apparatus. Anaesthesia 56:756–759
Harrison RR, Maull KI, Keenan RL, Boyan CP (1982) Mouth-to-mask ventilation: a superior method of rescue breathing. Ann Emerg Med 11:74–76
Skogvoll E, Wik L (1997) Active compression-decompression cardiopulmonary resuscitation (ACD-CPR) compared with standard CPR in a manikin model-decompression force, compression rate, depth and duration. Resuscitation 34:11–16
Acknowledgements
We thank the Resuscitation Council UK for providing financial support for this study, Huntleigh Healthcare Ltd. for providing the pressure redistributing mattress and the staff at Birmingham Heartlands Hospital for their participation. We also acknowledge the technical advice and support provided by Dr. K.G. Morallee, Laerdal Medical (UK) in relation to the operation of the VAM system.
Author information
Authors and Affiliations
Corresponding author
Additional information
Dr. Robert Benny was tragically killed in a road accident during the Summer of 2003. Dr. Benny was at the very start of a promising career in surgery. Our thoughts go to his family and friends.
G.D.P. and M.T. have received travelling fellowships from Huntleigh Healthcare, and M.T. has previously delivered lectures for Huntleigh Healthcare.
Rights and permissions
About this article
Cite this article
Perkins, G.D., Benny, R., Giles, S. et al. Do different mattresses affect the quality of cardiopulmonary resuscitation?. Intensive Care Med 29, 2330–2335 (2003). https://doi.org/10.1007/s00134-003-2014-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-003-2014-6