
Abstract
Children with autism spectrum disorders (ASD) and their unaffected siblings (US) are frequent targets of social bullying, which leads to severe physical, emotional, and social consequences. Understanding the risk factors is essential for developing preventative measures. We suggest that one such risk factor may be a difficulty to discriminate different biological body movements (BBM), a task that requires fast and flexible processing and interpretation of complex visual cues, especially during social interactions. Deficits in cognition of BBM have been reported in ASD. Since US display an autism endophenotype we expect that they will also display deficits in social interpretation of BBM. Methods. Participants: 8 US, 8 matched TD children, age 7–14; Tasks/Measurements: Social Blue Man Task: Narrative interpretation with a Latent Dirichlet Allocation [LDA] analysis; Social Experience Questionnaires with children and parents. Results. The US displayed as compared to TD: (i) low self-awareness of social bullying in contrast to high parental reports; (ii) reduced speed in identifying social cues; (iii) lower quality and repetitious wording in social interaction narratives (LDA). Conclusions. US demonstrate social endophenotype of autism reflected in delayed identification, interpretation and verbalization of social cues; these may constitute a high risk factor for becoming a victim of social bullying.
Sandia National Laboratories is a multi-mission laboratory managed and operated by Sandia Corporation, a wholly owned subsidiary of Lockheed Martin Corporation, for the U.S. Department of Energy’s National Nuclear Security Administration under contract DE-AC04-94AL85000. SAND2017-2189C.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others

Keywords
1 Introduction
Children with autism spectrum disorders (ASD) and their unaffected siblings (US) are more frequently victims of bullying than typically developing (TD) peers from families not affected by ASD (Sumi et al. 2006). We hypothesize that this greater victimization rate may be related to the primary clinical phenomena in autism: the specific deficit in perceiving, categorizing and understanding social interactions. Prior studies have reported the endophenotype of social deficits in US (Ozonoff et al. 2011). Social interactions are sequences of fast and complex visual experiences that require correct perception of visual-spatial directions of biological body movements (BBM), understanding the social intentions of these movements, and the ability to respond fast to each intention which relies on the correct perception and categorization of the earlier movements in the sequence. We investigate the interpretation of social cues as displayed in BBMs by TD children and US of children with autism. We will examine the level of this complex sequence – perceptual, cognitive, and verbal - on which an abnormality may be manifested in US. The narrative cognitive interpretation of social cues in BBM will be related to personal experiences of bullying. To our knowledge, this relationship has not been studied yet. The long-term goal of this investigation is to better understand in US of children with autism the interplay between difficulties in fast cognitive processing and verbalization of social cues, as displayed in BBM and high risk of these children to bullying victimization.
1.1 Social Bullying in ASD and Their Unaffected Siblings
Core clinical symptoms of ASD include anxious insistence on sameness, purposeless ritualistic cognitive and motor acts and severe difficulty to communicate, initiate and maintain social interactions (DSM-V; American Psychiatric Association 2013). Current research shows one in sixty-eight children being diagnosed with ASD (Center for Disease Control 2014). ASD is a heterogeneous and neurodevelopmental disorder with multiple etiological factors including: hereditary (Kabot et al. 2003), metabolic and neurological (Kennedy and Courchesne 2008; Manzi et al. 2008; Minshew and Keller 2010) and neurodevelopmental (Durkin et al. 2008; Nelson et al. 2001; Varcin and Nelson 2016). Currently, special education, behavior modification and an array of pharmacological therapies are used to enhance the individual’s overall functioning, but a targeted treatment or preventive approach has not been developed yet.
Evidence is accumulating about genetic and hereditary risks for developing ASD. Siblings of children with ASD are 5–10 times more likely to experience a pervasive developmental disorder than a child from the general population (Sumi et al. 2006). Siblings not diagnosed clinically with the disorder are also more likely to have an ASD trait endophenotype, that is expressing characteristics in cognition (attention, learning) and brain function similar to ASD to a much higher degree than in typically developing (TD) children in the population at large (Ozonoff et al. 2011). Consistent with the apparent differences between children with ASD and TD in social interaction and communication, children with ASD are reported to experience more peer victimization. Bullying experiences of clinically unaffected siblings have not attracted yet attention of researchers.
Olweus (1993) defines bullying as aggressive, intentional, and repeated behaviors that involve a power imbalance and inflict mental and physical harm. Bullying can occur in physical, verbal, social, or cyber forms (Cappadocia et al. 2012). In the traditional view, the behavior of a child who bullies others have been correlated with drugs and alcohol abuse, school dropout, earlier sexual activity, criminal convictions, and abusiveness (Olweus 1993). The current view of “bully” has been broadened with sophisticated relational manipulations and cyber abuse. Negative consequences for victims of bullying could be severe, and include depression, anxiety, physical and psychological health concerns, decreased academic performance, reduced social involvement, suicidal ideations and in extreme cases the school shootings (Sterzing et al. 2012). Bullying of a child may have a devastating impact on families, and thus becomes a major social problem to be solved. We are focusing here exclusively on perceptual and cognitive characteristics of a child who experiences social victimization or bullying.
Recent research has shown an increase in prevalence of school bullying. For TD school children, the prevalence of peer victimization averages at 30% (Molcho et al. 2009). However, in children with ASD reports show peer victimization between 34–94% (Cappadocia et al. 2012; Carter 2009; Little 2002; Van Roekel et al. 2010). The large range in victimization of children with ASD is in part due to the difference in report styles (i.e. who reports the bullying, length of time considered). The accuracy of self-reports by individuals with ASD has also been questioned due to the perception of social knowledge and interpretation of bullying involvement.
One theoretical framework about communication and social deficits in children with ASD that may be related to their susceptibility to bullying is their deficits in the Theory of Mind (ToM). ToM is the mental ability to attribute beliefs and attitudes to others and has been used to describe social behavior in autism (Baron-Cohen et al. 1985). Van Roekel et al. (2010) conducted a study that considered the ToM and perception of bullying in adolescents with ASD and found a relationship between weaker ToM and greater exposure to victimization. In a comprehensive literature review of the ToM and ASD, Baron-Cohen (2000) suggested that ToM deficits are universal in individuals with ASD therefore those with ASD are more likely to experience peer victimization. Our study will permit characterization of these risk factors and their interplay in bullying, as we will be asking US children to assign intentions and social behavioral aims to stimuli expressing BBM.
Another study examined if certain characteristics might lead to greater victimization in ASD (Sterzing et al. 2012). The results showed that: (1) Individuals with ASD who had less deficits in social skills were less likely to be bullied due to their more socially appropriate responses; (2) Those engaging in conversational interactions, however, were more likely to be bullied, because they exposed the poverty and inappropriateness of verbal expressions to be negatively seen by their peers; (3) Children in general education classrooms were more likely to be bullied because of the unprotected environment; (4) Children who had at least one peer whom they considered a friend were less likely to be victimized, and (5) Children who had comorbid conditions (e.g. attention-deficit/hyperactivity disorder) were more likely to be bullied. The findings were consistent with other studies showing that children attending a public school and diagnosed with Asperger syndrome are at the greatest risk of being a victim of social bullying in the forms of rumor spreading or exclusion (Zablotsky et al. 2014; Cappadocia et al. 2012). The more friends a child has, the less likely they are to experience victimization, which highlights the impact of the social component as a factor for resilience to victimization (Cappadocia et al. 2012). The above evidence suggests that a relationship exists between bullying and social interactions, interpretations, and communication as an explanation for higher victimization rates. These finding form a foundation for our study.
As far as we know, no research has been reported on peer victimization of clinically unaffected siblings. Most investigators consider these US individuals as a typically developing group (Nowell et al. 2014). Nowell et al. (2014) however, made an important observation that children with an ASD diagnosis are more frequently bullied than their siblings without a diagnosis. This study is inspiring in directing our attention to the cognitive risk factors of social bullying in unaffected siblings of children with ASD in comparison to their TD peers. Due to the role of genetics in ASD, we predict that clinically unaffected siblings are more likely to experience the trait endophenotype of difficulties in social communication or interaction that we see in ASD, and, thus, will be more susceptible to social bullying than their TD peers.
1.2 Visual Processing of Biological Body Movements (BBM)
BBM paradigms have been successfully used to test the perception of biological body movement in humans. Studies have shown that the perceptual system is able to accurately and quickly identify the biological body motion and distinguish it from other types of motion patterns (Hubert et al. 2007). Researchers have found that typically developing persons can accurately determine social meanings associated with bodily movements such as the gender of an individual walking or emotions/attitudes (Hubert et al. 2007). However, individuals with ASD have been found to have difficulties when perceiving actions of others’, their subjective states, and emotions as compared to TD (Koldewyn et al. 2001; Lainé et al. 2011; Swettenham et al. 2013). Specifically, children with ASD were impaired when distinguishing expressive/emotional states (e.g. bored, tired, hurt) when compared with TD and peers with other developmental disorders who have intact the interpretation of object motions (Moore et al. 1997). Thus, BBM tasks can be useful when testing perception of social intentions expressed in body motion.
Little research has been conducted on social perception in unaffected siblings. Those reported relate mostly to perception of faces. Dalton et al. (2007) reported that the gaze fixations and brain activation patterns of US during face-processing is similar to children with ASD and largely different than their typically developing group indicating differences in social processing as well as underlying neural circuitry. Further, Kaiser et al. (2010) using fMRI found distinctly different pattern of brain activation to body motion when compared to typically developing children, even though their behavioral responses were similar. These studies showed that US display neural signatures of increased compensatory activity in regions implicated in social perception and cognition, significantly different than those in the TD and ASD subjects. This could indicate protective genetic factors that are vital for understanding treatment and intervention in those with ASD.
1.3 Rationale
Social interactions belong to very complex and multi-stage visual events that require a fast and accurate perception and interpretation of another’s actions. In addition, one must then be able to quickly and adequately evaluate the event and respond in a socially appropriate manner so not to be rejected or penalized. Examining one’s interpretation of social interactions as displayed by BBM could provide an important insight into the risk factors that contribute to the vulnerability of becoming a victim of bullying.
We examine the interpretation of social content of BBM and compare it to both parental reports about the child’s experience with bullying and to the child’s self-reported social interactions questionnaire. The ultimate goal of this study is to contribute to developing a new line of research on prevention of social bullying among healthy children and children with psychopathological disorders. We predict that: (i) In clinically unaffected siblings (US) the self-reports and parental reports will reveal significantly more prevalent social bullying events than in their TD peers; (ii) US Children, compared to their TD peers, will require a significantly longer time for perception and interpretation of social interactions as expressed in BBM, and (iii) In US the quality and quantity of narratives about the social meaning of BBM will be lower than in TD.
2 Methods
2.1 Participants
Sixteen children participated in this study: eight unaffected siblings of children with ASD (US; 5 males, mean age = 11y6m, SD = 2y5m) and eight typically developing controls (TD; mean age = 11y0m, SD = 2y8m) ranging from 7 to 14 years for both groups. TD children were matched to US for age, sex, SES, and the developmental markers of speaking and walking onset (p > .05 for all demographics).
The inclusion criteria for TD involved: age 6–16, both genders and normal academic achievements at school. The exclusion criteria involved: no current Central Nervous System medication, no history of premature birth or TBI, and no history or current DSM diagnosis including substance abuse or ADHD; no first- or second-degree family members diagnosed with ASD, psychotic and bipolar disorders; no neuropsychological scores consistently −2SD below age norms. TD children were recruited by flyers on the UNM Campus and by personal contacts. The inclusion and exclusion criteria for US were identical except that US must have had a first- or second-degree family member diagnosed with ASD: six had a sibling diagnosed, one had a cousin with ASD and another had a second degree cousin with Asperger’s Syndrome and a parent with OCD. All family members who had an ASD diagnosis were males. The US children were recruited from Clinical Centers for Children with ASD, by contact to Pediatric Psychiatrists and by personal contacts.
All participants underwent a telephone or in-person screening interview ensuring they met all inclusion/exclusion requirements before being invited to participate in our study. However, in one US subject we found out only after the data was processed that the child was taking a low dose of cognition enhancing medication (open on shelf) and was diagnosed with ADD. One US participant was removed from our analysis due to the consistently −2SD scores below her age normative scores and more than two standard deviations below normalized scores of other US participants. This child was undergoing a clinical diagnostic process that was revealed to us only after we completed testing.
2.2 Procedures and Measurements
All participants were tested in the Pediatric Neuroscience Laboratory, Psychology Clinical Neuroscience Center, The University of New Mexico. Child participants and their parent were briefed on the components of our study prior to signing the IRB approved consent/assent forms. The assent forms and the parental consent forms were signed before the testing began. The University of New Mexico (UNM) Institutional Review Board Committee for the School of Medicine (North Campus) approved this study. All participants were compensated $30 for their time and travel expenses.
The study constituted of two parts. Part I included two related tasks: first, visual-spatial perception task of the blue cartoon characters (Blue Man Test, BMT, Ciesielski 2003, 2007; based on The Blue Man Group, www.blueman.com/boston) while recording the performance accuracy, time of processing and the brain Event-Related Potentials (ERPs). After completing this task and a short resting break, the second task was administered. This involved table-paper presentation of two different characters from the BMT arranged into a socially meaningful interactions and we record the child’s narrative description of the social interaction between two blue characters expressed by their biological body movements (BBM). Part II of the study involved also the neuropsychological battery of tests for assessing child’s cognitive functions and clinical interviews. For details of the visual-spatial perception task and ERPs methods, see Bouchard et al. (2016; under review) and Newton et al. (2016).
2.2.1 Social Blue Man Task (SBMT): Interpretation of Social Cues in BBM
To investigate how US interpret social interactions as expressed by BBM of two interacting individuals, we present our figures in pairs. We will use the Social Blue Man Test (SBMT; Ciesielski et al. 2015) which is derived from the Blue Man Task (BMT; Ciesielski 2007). The SBMT involves static little blue characters that depict posture of a biological body motion and may be interpreted as expressing different intentions towards the second character in the image (Fig. 1). They are faceless to remain as simple as possible and thus do not require participants to observe both body motions and facial expressions. SBMT provides an opportunity to assess social interactions without an overload on sensory levels in children with ASD - which is a common occurrence in autism. The blue characters can be arranged into social interactions and can represent humans interacting with each other as a snapshot of human BBM.

(SBMT, Ciesielski et al. 2015). (Color figure online)
Example of social scenario represented by a snapshot of BBM in social blue man test
Participants were shown 10 images consisting of 2 blue characters depicting a social interaction. First, the participant had to decide if the blue men’s’ interactions were either good (happy and nice) or bad (mean and angry) and press the button immediately: green if good and black if bad. The stress on the speed of the response was emphasized. Response “I don’t know” was permitted only if encouragements failed. The main task was to “imagine what the blue men are doing and create a story about it, including information such as who they are, where they are right now, and why they are doing all of this.” Responses were recorded with a digital voice recorder and were later transcribed. There was no time limitation but the response time on completion of the task was recorded.
2.2.2 Self- and Parent-Reports on Bullying Experiences
To gain an understanding of each participant’s daily social interactions, we created a questionnaire in the Pediatric Neuroscience Laboratory called the “Social Interactions Questionnaire”. Some questions asked were, “Do you know what bullying is?” “How many friends do you have?”, “Are children nice to you at school or during after-school programs?”, “Have you ever seen someone who was bullied?”, and “Have you experienced any bullying?” The answers to these questions provide information on the participants’ awareness of being a target of bullying and the child’s resilience to bullying, as well as their social adjustment.
Finally, a confidential clinical interview with each participant’s parents were conducted. Detailed information was collected about the child’s prenatal and early postnatal life history, family history of DSM-V disorders, current status of family health, constitution and social-economic status. Additionally, a Traumatic Experiences Questionnaire (Ciesielski et al. 2015, Manual, PNL) was used to obtain parental knowledge about their child’s exposure to peer victimization. Among several other questions the following were posed to the parent: (1) “Has your child experienced any rejection, teasing and/or aggressive behaviors from his/her peers in school or other places? – please describe.” and (2) “Has your child experienced any psychological or physical punishment, aggression by other or isolation from others?”
2.3 Statistical Data Analysis
The data analysis was conducted using three approaches: t-tests for independent samples, Pearson correlations and a Latent Dirichlet Allocation analysis. The independent samples t-test was used to analyze: between-group contrasts in performance accuracy and reaction time during the SBMT and all neuropsychological tests scores. Pearson correlation coefficients were used to find within-group correlations on neuropsychological tests and the results on severity of bullying questionnaires. Latent Dirichlet Allocation (LDA) as a method of text analytics via topic modeling was used to analyze the transcribed stories from the SBMT in an unbiased manner (Blei et al. 2003). Each word in the collection of documents is treated as a finite mixture of an unobservable set of topics so that the LDA provides topic representation in each document. The t-tests and correlations were conducted on SPSS 23 and the LDA was completed with software developed by researchers at Sandia National Laboratories.
3 Results
We examined the association between the quality and quantity of verbal narratives regarding social interactions of BBM with the parent- and self-reports of exposure to bullying (Newton et al. 2016). Details of the ERP data were processed separately (Bouchard et al. 2016). TD children showed no significant neuropsychological deviations, except for significantly prolonged time of recognition of complex visual figures with ambiguous meaning (p > 0.05). There were also no differences found in US in visual-spatial perception of BBM.
While initiating this study, we predicted significantly more frequent social bullying events to be reported by the US children and their parents than in their TD peers. As shown in Fig. 2, parental- and self-reports regarding bullying experiences significantly differed. Parents-reported five times more bullying incidents in US (M = 1.38, SD = .74) than in TD (M = .25, SD = .46; p = .003, d = −1.8) and more bullying than was reported by self-reports by US children (M = 2.21, SD = .32). Self-reports show no significant differences in number of bullying events from those reported by TD children (M = 2.34, SD = .30, p = .42, d = .44). This result may need to be discussed in context of considerable frequency of bullying reported by TD children, but also as a result of poor insight of US children into being a target of bullying.

Percentage of parent- and self- reports that responded “yes” to experiencing peer victimization in both unaffected siblings and typically developing.
US children’s parents reported that 88% of children experienced some form of consistent peer victimization while only 38% of self-reporting US children admitted being bullied. A reverse statistic is observed in TD children: TD parents reported that 25% of their children experienced being bullied while 43% of TD children admitted victimization. Our data provide support to and extend our earlier prediction: US are more frequently bullied when we carefully consider parental reports. This observation of discrepancy between US parental reports and US children’s reports is important as it may suggest low awareness of social victimization in US. Additionally, we found that TD children also report a considerable exposure to bullying.
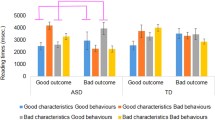
Our second prediction was also supported. Unaffected siblings needed significantly more time to decide if the BBM represent a “good” or “bad” social interaction. The Social Blue Man Task provided participants with images of social interactions and were told to decide as quickly as they could if the image displayed good or bad situations. They were informed that there were no incorrect answers but to respond with how they perceived the image. The response time was measured from the first view of the image and the response of “good” or “bad”. We found that there is a significant delay in response time in US (M = 6.86, SD = 4.26) as compared to TD (M = 2.22, SD = 0.74, p = .01 d = −1.52). Figure 3 shows the relationship of the RT for both tasks in each group. Furthermore, a significant negative correlation of r = − 0.92, p < .001 was found between time delay in decision making about the good/bad social content of the BBM displayed in SBMT stimuli and the lower report rate of bullying by US. This suggests that the slower the US are in their social judgment the less insight they have and therefore report less bullying incidents.

Delayed response time during the SBMT in US.
Finally, we predicted that the quality and quantity of narratives about the social meaning of BBM would be lower in US than in TD and negatively correlated with high frequency of social bullying in US. We conducted the LDA analysis by combining all TD and all US responses into their two separate groups. As seen in Fig. 4, our TD participants weighed heavily on Topic 1 while our unaffected siblings weighed heavily on Topic 0. This unbiased model therefore distinguished differences between our two populations in SBMT responses.

The relationship between weight of each topic and subject group from LDA analysis of transcribed responses to the social blue man task. An inverse relationship exists between each group and the topic they are categorized into according to the unbiased LDA.
The greatest differences between Topic 0 and Topic 1 are the amount of words and the diversity of words chosen, not on their content. By examining word clouds of the transcriptions, we can determine frequency of root words used in each topic. The larger the word in the cloud, the more frequently it is used. Topic 0 has many words that are used frequently and almost all of the words are fairly large in size. This indicates several words were used often by many of our unaffected siblings and that most words were used more than once. However, in Topic 1, only a few words had great frequency while majority of the words were unique. Therefore, Topic 0 is labeled “Uniform” and Topic 1 is labeled “Diverse.” This tells us that our US group provided narratives that were repetitive and lacked quality and flexibility in word choices (Fig. 5).

The word clouds indicate that there was a lack of variation in words used by all unaffected siblings when describing social narratives of the SBMT images.
4 Discussion
We examined the effects of bullying, as measured by both a parent-and self-report, in unaffected siblings of children with ASD. We collected unique information regarding the specific mechanism of underreporting of bullying by US children. We also analyzed the quality of narratives used by US and TD children to describe socially meaningful BBM snapshots to determine if any differences existed between US and TD in perception, interpretation, and reporting of social cues. US displayed significantly delayed interpretations and poorer social narratives. This may be indicative that US struggle to adequately process and interpret social interactions and then report and interpret them, but also that they may be unaware of their difficulties. This is an important insight into creating preventative measures for the US population. Programs that will be able to effectively help US children to increase the processing speed and improve the interpretation and communication of bullying experiences, would likely see more successful outcomes.
Delays in processing visual complex information may vastly interfere with identifying, interpreting, and responding to the fast, continuously changing, and often ambiguous social cues. As a result, unaffected siblings participating in our study might have had difficulty recognizing they were in fact a target of social bullying at school, hence they did not report about it during our testing. Their parental reports unravel a high frequency of victimizing events towards US children, which is consistent with the most recent literature (Nowell et al. 2014). While the parent-reports reveal significantly higher frequency of bullying experiences, the latent Dirichlet allocation showed in US poor verbal flexibility when describing social interactions. This difficulty might have reduced the ability of US to inform accurately, but also could be a foundation of their poor verbalization and poor awareness of bullying incidents. These findings are consistent with the Van Roekel et al. (2010) study, which showed a correlation between weaker ToM in ASD and greater exposure to victimization. To form a ToM with the interacting person one needs time to process the social messages and also verbal tools for understanding them and translating them into a socially-acceptable response. Baron-Cohen (2000) suggested that ToM deficits make individuals more likely to experience peer victimization. ToM may be one of the contributing factors responsible for the slow and partial only interpretation of social meaning of BBM by US children in our study.
The SBMT responses were recorded in relation to social interactions. The children who are typically developing are better able to describe their social surroundings than our US group. US of those with ASD showed a tendency to repeat words and did not use alternative words to describe the various social situations depicted. Since there were no statistically significant group differences on the neuropsychological tasks, with many of our US children outperforming our TD children, we cannot conclude that the results of LDA analysis is due to a lack of verbal abilities as such in the US. Considering the prolonged response times, we conclude that unaffected siblings of children with ASD perform equally well as TD on perception of visual-spatial characteristics of the BBM of the little blue man characters, but show significant deficiencies when they are required to describe the social meaning of the BBM of blue man interactions.
While this study improves our understanding of the mechanism underlying the social bullying in children displaying the endophenotype of ASD, there were some limitations that need to be addressed in future studies. First, our population consists of unaffected siblings of children with ASD- it will be important to examine children diagnosed with ASD with different levels of severity, and how this impacts the perception and interpretation of BBM. In addition, we aim to develop methods of nonverbal measurement of interpretation of BBM that should allow subjects with ASD to participate despite their verbal deficits. Further, our study does not consider causation between interpretation of BBMs and bullying. Thus, future research should attempt to determine causal relationships. In the future, we would like to obtain a more rigorous and holistic perspective of the child’s bullying exposure and impacts to the child’s mental and physical health. Finally, we intend to continue testing children in larger samples.
There is some debate as to whether parent- or self-reports reveal more accurate bullying experiences. The most accepted conclusion is that parents tend to over report their child’s bullying experiences while individuals tend to under report their own bullying experiences. Regardless, that is the case whether children have a disorder or are typically developing. Therefore, to monitor the group differences in parent reports and children self-reports still provide an important insight into the status of bullying experienced in our schools. On the other hand, parents of a child with an ASD may be overly sensitive or even more involved with their children’s social interactions than parents of typically developing children, so they may have better insight to their child’s social interactions than a parent of a child who is TD.
This research provides some insight into the mechanism of bullying experienced by unaffected siblings of children with ASD. Although the cognitive abilities are similar in our TD and US subjects with no evident neuropsychological test deficits, a distinct and specific difference has been identified in the increased parent-report of peer victimization, delayed perception and interpretations on social interactions, and poorer quality of social narratives. The delay in interpretation and low quality of narratives may be characteristics of risk factors for the high exposure to bullying in unaffected siblings. Our findings might give rise to studies on improving the US child’s ability to perceive and absorb complex social cues.
References
American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th edn. Washington, DC (2013)
Baron-Cohen, S.: Theory of mind and autism: a fifteen year review. In: Baron-Cohen, S., Tager-Flusberg, H., Cohen, D.J. (eds.) Understanding Other Minds: Perspectives From Developmental Cognitive Neuroscience, pp. 3–20. Oxford University Press, New York (2000)
Baron-Cohen, S., Leslie, A.M., Frith, U.: Does the autistic child have a ‘theory of mind’? Cognition 21, 37–46 (1985)
Blei, D.M., Ng, A.Y., Jordan, M.I.: Latent Dirichlet allocation. J. Mach. Learn. Res. 3(1), 993–1022 (2003)
Bouchard, C., Solis, I., Seaman, B., Pesko, J.C., Ciesielski, K.R.: Developmental and familial characteristics of top-down inhibitory control networks and performance strategies: ERPs to the blue man stop-response task. Program No. 90.12. 2016 Neuroscience Meeting Planner. Society for Neuroscience, San Diego (2016)
Cappadocia, M.C., Weiss, J.A., Pepler, D.: Bullying experiences among children and youth with autism spectrum disorders. J. Autism Dev. Disord. 42(2), 266–277 (2012). doi:10.1007/s10803-011-1241-x
Carter, S.: Bullying of students with Asperger syndrome. Issues Compr. Pediatr. Nurs. 32, 145–154 (2009). doi:10.1080/01460860903062782
Centers for Disease Control: Autism Spectrum Disorder (ASD) (2014). http://www.cdc.gov/ncbddd/autism/facts.html#ref
Ciesielski, K.T.R.: Blue Man N-Back Test: Visual-Spatial Working Memory Paradigm (MGH/MIT AA Martinos Center for Biomedical Imaging, Radiology, Massachusetts General Hospital). (RN 0008929/2003, 2007) (2007)
Ciesielski, K.T.R., Newton E.V., Solis, I.: Social Blue Man Test. Manual. Pediatric Neuroscience Laboratory, PCNC, Psychology, University of New Mexico, Albuquerque, NM 87131 (2015)
Dalton, K.M., Nacewicz, B.M., Alexander, A.L., Davidson, R.J.: Gaze fixation, brain activation, and amygdala volume in unaffected siblings of individuals with autism. Soc. Biol. Psychiatry 61, 512–520 (2007)
Durkin, M., Maenner, M., Newschaffer, C., Lee, L., Cunniff, C., Daniels, J.L., Schieve, L.A.: Advanced parental age and the risk of autism spectrum disorder. Am. J. Epidemiol. 168(11), 1268–1276 (2008)
Hubert, B., Wicker, B., Moore, D.G., Monfardini, E., Duverger, H., Da Fonséca, D., Deruelle, C.: Brief report: recognition of emotional and non-emotional biological motion in individuals with autistic spectrum disorders. J. Autism Dev. Disord. 37(7), 1386–1392 (2007). doi:10.1007/s10803-006-0275-y
Kabot, S., Masi, W., Segal, M.: Advances in the diagnosis and treatment of autism spectrum disorders. Prof. Psychol. Res. Pract. 34, 26–33 (2003)
Kaiser, M.N., Hudac, C.M., Schultz, S., Lee, S.M., Cheung, C., Berken, A.M., Pelphry, K.A.: Neural signatures of autism. Proc. Nat. Acad. Sci. USA 107(49), 21223–21228 (2010)
Kennedy, D.P., Courchesne, E.: The intrinsic functional organization of the brain is altered in autism. Neuroimage 39(4), 1877–1885 (2008)
Koldewyn, K., Whitney, D., Rivera, S.M.: Neural correlates of coherent and biological motion perception in autism. Dev. Sci. 14(5), 1075–1088 (2001). doi:10.1111/j.1467-7687.2011.01058.x
Lainé, F., Rauzy, S., Tardif, C., Gepner, B.: Slowing down the presentation of facial and body movements enhances imitation performance in children with severe autism. J. Autism Dev. Disord. 41(8), 983–996 (2011). doi:10.1007/s10803-010-1123-7
Little, L.: Middle-class mothers’ perceptions of peer and sibling victimization among children with Asperger’s syndrome and nonverbal learning disorders. Issues Compr. Pediatr. Nurs. 25, 43–57 (2002)
Manzi, B., Loizzo, A., Giana, G., Curatolo, P.: Autism and metabolic diseases. J. Child Neurol. 23(3), 307–314 (2008)
Minshew, N.J., Keller, T.A.: The nature of brain dysfunction in autism: functional brain imaging studies. Cur. Opin. Neurol. 23(2), 124–130 (2010)
Molcho, M., Craig, W., Due, P., Pickett, W., Harel-Fisch, Y., Overpeck, M.: Cross-national time trends in bullying behaviour 1994–2006: findings from Europe and North America. Int. J. Public Health 54, 225–234 (2009)
Moore, D.G., Hobson, R.P., Lee, A.: Components of person perception: an investigation with autistic, nonautistic retarded and typically developing children and adolescents. Br. J. Dev. Psychol. 15, 401–423 (1997)
Nelson, K.B., Greather, J.K., Croen, L.A., Dambrosia, J.M., Dickens, B.F., Jeliffe, L.L.: Neuropeptides and neurotrophins in neonatal blood of children with autism or mental retardation. Ann. Neurol. 49, 597–606 (2001)
Newton, V., Solis, I., Avina, G.E., McClain, J.T., King, C., Bouchard, C., Ciesielski, K.R.: Cognition of biological body movement as a risk factor for social bullying in unaffected siblings of children with autism spectrum disorders. Presentation at Neuroscience 2016, San Diego, California (2016)
Nowell, K.P., Brewton, C.M., Goin-Kochel, R.P.: A multi-rater study on being teased among children/adolescents with autism spectrum disorder (ASD) and their typically developing siblings: associations with ASD symptoms. Focus Autism Other Dev. Disabil. 29(4), 195–205 (2014)
Olweus, D.: Bullying at School: What We Know and What We Can Do. Blackwell, Oxford (1993)
Ozonoff, S., Young, G.S., Carter, A., Messinger, D., Yirmiya, N., Zwaigenbaum, L., Stone, W.L.: Recurrence risk for autism spectrum disorders: a baby siblings research consortium study. Pediatrics 128, e488–e495 (2011)
Sterzing, P.R., Shattuck, P.T., Narendorf, S.C., Wagner, M., Cooper, B.P.: Bullying involvement in autism spectrum disorders: prevalence and correlates of bullying involvement among adolescents with an autism spectrum disorder. Arch. Pediatr. Adolesc. Med. 166(11), 1058–1064 (2012). doi:10.1001/archpediatrics.2012.790
Sumi, S., Taniai, H., Miyachi, T., Tanemura, M.: Sibling risk of pervasive developmental disorder estimated by means of an epidemiologic survey in Nagoya, Japan. J. Hum. Genet. 51, 518–522 (2006)
Swettenham, J., Remington, A., Laing, K., Fletcher, R., Coleman, M., Gomez, J.C.: Perception of pointing from biological motion point-light displays in typically developing children and children with autism spectrum disorder. J. Autism Dev. Disord. 43(6), 1437–1446 (2013). doi:10.1007/s10803-012-1699-1
Varcin, K.J., Nelson, C.A.: A developmental neuroscience approach to the search for biomarkers in autism spectrum disorder. Curr. Opin. Neurol. Apr. 29, 123–129 (2016). doi:10.1097/WCO.0000000000000298
Van Roekel, E., Scholte, H.J., Didden, R.: Bullying among adolescents with autism spectrum disorders: prevalence and perception. J. Autism Dev. Disord. 40, 63–73 (2010). doi:10.1007/s10803-009-0832-2
Zablotsky, B., Bradshaw, C.P., Anderson, C.M., Law, P.: Risk factors for bullying among children with autism spectrum disorders. Autism 18(4), 419–427 (2014). doi:10.1177/1362361313477920
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2017 Springer International Publishing AG
About this paper
Cite this paper
Newton, V., Solis, I., Aviña, G.E., McClain, J.T., King, C., Rewin Ciesielski, K.T. (2017). Analysis of Social Interaction Narratives in Unaffected Siblings of Children with ASD Through Latent Dirichlet Allocation. In: Schmorrow, D., Fidopiastis, C. (eds) Augmented Cognition. Neurocognition and Machine Learning. AC 2017. Lecture Notes in Computer Science(), vol 10284. Springer, Cham. https://doi.org/10.1007/978-3-319-58628-1_28
Download citation
DOI: https://doi.org/10.1007/978-3-319-58628-1_28
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-58627-4
Online ISBN: 978-3-319-58628-1
eBook Packages: Computer ScienceComputer Science (R0)