
Abstract
The distal airways are covered with a heterogeneous layer of cells known as the alveolar epithelium. Alveolar epithelial cells provide the major barrier between the airspace and fluid filled tissue compartments. As such, regulation of the alveolar epithelium is critical to maintain a healthy lung and for optimal gas exchange. In this chapter, we discuss functional roles for alveolar epithelial cells with particular emphasis on intercellular junctions and communication. As a thin layer of cells directly exposed to atmospheric oxygen, alveoli are particularly sensitive to oxidant insults. Alcohol significantly diminishes the normal antioxidant reserves of the alveolar epithelium, thereby rendering it sensitized for an exaggerated damage response to acute and chronic injuries. The effects of alcohol on alveolar epithelia are discussed along with open questions and potential therapeutic targets to prevent the pathophysiology of alcoholic lung disease.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
- Pneumocyte
- Alveolus
- Claudin
- Connexin
- Tight junction
- Gap junction
- Ethanol
- Barrier function
- Pulmonary edema
- Fluid clearance
Introduction
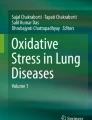
Gas exchange occurs in the terminal airspaces of the lung, known as alveoli. The alveolar epithelium consists of two distinct cell populations where >90 % consists of Type I cells and the remainder are Type II cells (Fig. 8.1). Type I cells are exceptionally thin squamous cells that allow efficient gas permeability between the airspace and bloodstream. Type II cells are cuboidal epithelia that serve several functions including the production and secretion of pulmonary surfactant that maintains alveolar surface tension and promotes innate immunity. Type II cells produce cytokines that are critical for regulation of the alveolar barrier and in the regulation of alveolar immune cells. Type II cells also respond to injury and have the ability to proliferate and differentiate into Type I cells to repair damaged alveoli.

Morphology and distribution of alveolar epithelial cells. The en face representation of alveolar epithelium shows the relative size and number of type I and type II cells [115]. The monolayer is heterogeneous and predominantly contains two classes of cell–cell interfaces: type I–type I cell junctions and type I–type II cell junctions. Adapted from [26]
Critically, Type I and Type II cells function in a cohesive manner in order to regulate alveolar fluid balance. This depends on functional interactions between these cells, which are regulated in large part by intercellular junctions at sites where cells are in direct contact. Paracrine signaling by cytokines and extracellular ATP also integrate alveolar epithelial cell function.
The alcoholic lung presents a unique pre-disease state that renders the tissue susceptible to damage when presented with a significant inflammatory insult. This is in large part because the ability of the lung to maintain a proper air/liquid interface is compromised due to a deficit in alveolar epithelial barrier function. Here we focus on how alcohol impairs alveolar epithelial physiology, with particular emphasis on that critical barrier function.
Effects of Alcohol on Alveolar Glutathione
Lung airspaces are directly exposed to environmental oxygen, which makes them vulnerable to oxidant stress. In patients requiring oxygen supplementation, there is even greater oxidant stress. As a major component of antioxidant defense, lungs use the tri-peptide thiol antioxidant glutathione [1]. Levels of glutathione in the alveoli are among the highest in the human body and are present at concentrations of 400 μM or more in the alveolar fluid. Type II cells also contain high levels of intracellular mitochondrial and cytosolic glutathione pools that enable them to resist oxidant stress.
In contrast to the unstressed lung, chronic alcohol ingestion increases oxidative damage by depleting glutathione [2, 3]. Type II cells from alcohol-fed rats contain 20 times less total glutathione than controls and airspace glutathione is depleted [2, 4]. Glutathione levels are further decreased during endotoxemia where whole lung glutathione was reduced by 25 % in alcohol-fed septic rats as compared to control-fed septic rats, consistent with an additive effect of sepsis as a second hit on oxidative stress when it occurs in alcoholics [5, 6].
Metabolsim of dietary alcohol (ethanol) to acetaldehyde directly depletes glutathione, causing oxidant stress [6, 7]. Alcohol also induces cell-signaling pathways that contribute to oxidant stress, including increasing the production of Transforming Growth Factor β (TGF-β), which appears to play a critical role in mediating the alcoholic lung phenotype [5, 8]. TGF-β decreases lung glutathione by inhibiting γ-glutamylcysteine synthetase expression [9, 10] and further increases oxidant stress by increasing Nox expression [11, 12] and H2O2 production [13]. Consistent with this effect on oxidant stress, TGF-β accelerates the progression of acute lung injury [14, 15].
The effects of alcohol on the total cell glutathione pool suggest the potential of antioxidant therapies as a means to reduce the severity of acute lung injury. Consistent with this, supplementing the diets of alcohol-fed rats with the glutathione precursor procysteine reduces oxidant stress and reverses many of the pathophysiological effects of alcohol on the lung [16–18]. Antioxidant therapies have not yet been proven to be effective in decreasing mortality in critically ill patients since they have never been directly tested in individuals with alcohol use disorders. However, antioxidants can prevent the severity and duration of acute lung injury [19, 20]. Therefore, bolstering the antioxidant reserves of the lung are likely to be best used as an adjunct to other therapeutic approaches.
Alveolar Epithelial Barrier Function and Fluid Balance
The alveolar epithelium controls fluid balance through a combination of processes. First, the alveolus provides a permeability barrier which prevents fluid efflux from the bloodstream, lymphatic system, and tissue into the airspaces. Second, the alveolus actively promotes fluid efflux from the airspaces through a system of ion channels where water osmotically accompanies ion transport. To some extent, barrier function and ion transport can compensate for each other; however, the extent of compensation is not unlimited.
Most progress on defining the mechanistic basis for the effects of alcohol on alveolar barrier function have been through studies of rodents fed the isocaloric Lieber DeCarli alcohol diet that carefully controls for nutrition and thereby can “isolate” the independent effects of alcohol ingestion [21]. Studies in the intact animal have demonstrated that rats on a chronic alcohol diet have enhanced permeability to small molecules (e.g., inulin) as well as to proteins as large as serum albumin [22]. Moreover, their ability to resist a saline challenge is impaired. Understanding this at a molecular level has benefited from the observation that the “alcoholic lung” phenotype of alveolar epithelial cells isolated from alcohol-fed rats persists in culture. In other words, alveolar epithelial cells isolated from alcohol-fed rats and grown in monolayers in culture remain leakier than comparably isolated and cultured cells from control-fed rats [22]. The basis for this is not fully understood, but it is likely that alveolar epithelial cells differentiate in response to chronic stress in the alcoholic lung and that this results in epigenetic modification to genomic DNA that modifies the behavior of these cells [23]. Epigenetics is a nascent field in alcohol research and is only beginning to be explored [24, 25]. Given the persistence of the alcoholic lung phenotype, alveolar epithelial cells from alcohol-fed rats provide a valuable model system to study their pathophysiology.
Tight Junctions and Alveolar Barrier Function
The bulk of the alveolar barrier consists of the cells themselves. The remaining barrier function is due to a series of structures at cell–cell interfaces called tight junctions. Tight junctions serve as a sealing point between polarized epithelial cells and denote the boundary between the apical and basolateral plasma membrane domains (Fig. 8.2). This segregation and sealing function formed by the tight junctions provide two important physiological functions of the epithelium: (1) a physical barrier to small molecules and (2) a series of paracellular ion channels that enable ion diffusion between cells [26].

Core tight junction protein complex. Shown are the major functional components of tight junctions known to directly interact. These include transmembrane proteins (claudins, occludin), scaffold proteins (ZO-1, ZO-2), and the actin cytoskeleton. Head-to-head interactions between claudins on adjacent cells form the basis for paracellular channels which restrict permeability. Homotypic interactions (between the same type of claudin) and heterotypic interactions (between different types of claudins) are depicted. The likely presence of additional scaffold proteins is represented by the orange circle. Not shown are immunoglobulin-fold transmembrane proteins, which associate with tight junctions and also regulate claudin expression and tight junction permeability, such as Junction Adhesion Molecule A (JAM-A) [116]. Adapted from [26]
Tight junctions are formed by a complex that includes transmembrane proteins, cytosolic scaffold proteins, and cytoskeletal proteins. Tight junction permeability is primarily mediated by proteins known as claudins that span the membrane bilayer four times and have both the N- and C-terminal domains oriented inside towards the cytosol. The C terminus of claudins interacts with cytosolic scaffold proteins, most notably zonula occludens-1 (ZO-1) and ZO-2 [27]. ZO-1 and ZO-2 in turn link claudins to the actin cytoskeleton. While almost all claudins interact with ZO-1 and ZO-2, they differ in the extent of actin association, which correlates with incorporation into functional tight junctions. Other transmembrane proteins also regulate tight junction assembly and stability, particularly occludin and tricellulin [28]. Roles for these proteins in the alveolar epithelium are continuing to be elucidated. However, occludin and ZO-1 expression are both down-regulated by the alveolar epithelium in response to alcohol, consistent with the concept that an early and primary defect in the alcoholic lung is impaired alveolar epithelial barrier function [29, 30].
There are over a dozen claudin isoforms expressed by the alveolus; the nine most prevalent are summarized in Table 8.1. Of these, 97 % of claudin mRNA in both type I and type II cells encodes for claudin-3, claudin-4, and claudin-18 [31]. However, type II cells express significantly more claudin-3 than is expressed by type I cells. This difference has functional ramifications, since claudin-3 expression increases alveolar tight junction permeability whereas claudin-4 makes tight junctions less permeable (Fig. 8.3) [32]. One consequence of this difference is that type II–type I cell interfaces are enriched for claudin-3 and are therefore likely to be more permeable than type I–type I cell interfaces. Functionally, the unique permeability of type II–type I cell junctions might provide a paracellular pathway for ion and fluid diffusion that counterbalances ion flux due to channel activity (see below).

Differential effect of increasing cldn-3 or cldn-4 on alveolar epithelial cell barrier function. Model type I alveolar epithelial cells transduced with YFP-cldn-3 (filled square), YFP-cldn-4 (filled diamond), YFP-control virus (filled circle), or untransfected controls (filled triangle) were assessed for the effect of altering claudin expression on barrier function, as determined using transepithelial resistance (TER; Ohm × cm2) (Y-axis). The expression ratio cldn-4/cldn-3 was determined by immunoblot (X-axis) demonstrating that there was a linear relationship between cldn-4/cldn-3 ratio and TER (r 2 = 0.93). Cells expressing increased cldn-3 had significantly lower TER than either control cells or cells expressing increased cldn-4 (p <0.05). Increasing cldn-4 also significantly increased barrier function (p < 0.05). Adapted from [37]
Critically, claudin-4 is up-regulated during ventilator-induced lung injury. Since claudin-4 expression correlates well with human lung fluid clearance and is inversely related to the severity of the Acute Respiratory Distress Syndrome (ARDS), this underscores a protective effect of claudin-4 in lung function [33, 34]. Claudin-18 has a longer C-terminal domain and is more tightly associated with the cytoskeleton than claudin-3 or claudin-4, most likely due to increased interactions with tight junction scaffold proteins [32]. Claudin-18 is decreased in response to inflammation [35], consistent with impaired barrier function in ARDS.
As mentioned above, alcohol impairs alveolar barrier function by increasing tight junction permeability. In part this is due to decreases in claudin expression [36]. Perhaps more critically, the decrease in alveolar barrier function due to alcohol is accompanied by a significant shift in tight junction morphology as determined by immunofluorescence microscopy (Fig. 8.4). In normal cells, claudins are predominantly localized to cell–cell contact sites. By contrast, cells impaired by alcohol show significant morphological disruption of claudin localization, including strand breaks and increased intracellular labeling. Intriguingly, this correlates with an increase in expression of claudin-5, which is normally expressed at low levels in the alveolus [36, 37]. These effects of alcohol on claudin-5 and epithelial barrier function are consistent with the observations that increased claudin-5 correlates with impaired lung epithelial barrier function in cells treated with methanandamide or in cells directly transfected with claudin-5 [38, 39]. However, whether there is a direct mechanistic link between claudin-5 and disruption of tight junction assembly and function in alveolar epithelium remains to be determined.

Alcohol impairs assembly of claudins into tight junctions. Model type I alveolar epithelial monolayers were derived from primary cells isolated from either control (a) or alcohol-fed (b) rats which were cultured for 6 days and then immunolabeled for cldn-7. In contrast with control alveolar epithelial cells, where cldn-7 prominently localized to sites of cell–cell contact (a), cells isolated from alcohol-fed rats had impaired claudin assembly (b) which correlated with impaired barrier function. Bar—10 μm. Adapted from [37]
Ion Channels and Alveolar Fluid Clearance
The primary mode of fluid efflux from airspaces is promoted by ion flux through alveolar epithelial cells that sets up an electrochemical gradient that drives water from airspaces into tissues. The majority of ion flux is due to sodium transport. On the apical surface, sodium transport into cells is mediated by epithelial sodium channels (ENaC), which are the rate-limiting step in alveolar sodium transport [40]. Transport out of cells on the basolateral surface is by Na,K-ATPases that actively pump sodium out of the cell and thereby provide the gradient that promotes transcellular passage of sodium from the alveolar space into the interstitium. Both type I and type II cells express sodium channels, as well as other ion transporters, that contribute to maintenance of lung fluid balance.
In contrast to the effect of alcohol on barrier function, alcohol increases net flux of sodium by having a direct effect on both parts of the sodium transport pathway. This was confirmed by examining the expression of lung Na,K-ATPase in rats fed the Lieber-DeCarli diet [41]. Na,K-ATPase is composed of several subunits, all of which were up-regulated in the alcoholic lung. When treated with the Na,K-ATPase inhibitor ouabain, lungs from alcohol-fed rats developed more edema than control lungs, indicating that increased Na,K-ATPase compensates for other deficits in maintenance of lung fluid balance induced by alcohol.
In parallel to this increase in Na,K-ATPase expression, ENaC is also up-regulated in the alcoholic lung [42]. Critically, ENaC activity was also increased by direct oxidation mediated through NADPH oxidase activity. This is in line with other studies demonstrating that reactive oxygen species have the capacity to increase ENaC and lung fluid clearance [43, 44]. Together, increased ENaC and Na,K-ATPase in the alcoholic lung provide a pathway for up-regulated fluid clearance that can compensate for deficits in barrier function induced by dietary alcohol. Studies to date have focused on sodium transport; chloride transport must also increase in order to retain electronic neutrality across the alveolar epithelium. Whether this occurs via up-regulation of chloride channels or by chloride transport via the paracellular route remains an open question [40]. Taken together, these observations explained an initial paradox when the phenotype of the alcoholic lung was first being examined experimentally. Specifically, if chronic alcohol ingestion causes such significant defects in alveolar epithelial permeability, why don’t alcoholics have pulmonary edema at baseline? The marked up-regulation of active fluid transport mechanisms in the alcoholic lung appear to compensate for the increased paracellular permeability and maintain a relatively “dry” airspace. However, this new equilibrium is far more susceptible to the stresses imposed by acute inflammation such as pneumonia or sepsis, and the alcoholic lung is far more prone to alveolar flooding with proteins and fluids during critical illness.
Therefore, in the otherwise healthy alcoholic, barrier function and fluid efflux are counterbalanced to maintain a non-edematous lung. However, if alveolar barrier function is further impaired due to a second hit, e.g., sepsis or barotrauma, the lung requires an additional increase in sodium transporters in order to prevent alveolar edema. ENaC in the alcoholic lung does have some additional capacity for further up-regulation (e.g., in acute response to endotoxin [42]). However, it is clear that lungs of injured alcohol-fed animals are more susceptible to endotoxin and sepsis induced lung edema than non-alcohol-fed controls [2, 18]. This suggests that in the alcoholic lung, fluid clearance saturates at a level insufficient to compensate for barrier dysfunction which, in turn, exacerbates the severity of ARDS. Therefore, any treatment modality designed to prevent alcohol-associated ARDS must address alveolar tight junctions, since it is not likely to be possible to increase fluid clearance enough to prevent alveolar flooding.
Intercellular Communication
Gap Junctions
Gap junctions provide a means for intracellular communication by forming channels that connect the cytosols of adjacent cells in a tissue (Fig. 8.5). This connection enables the direct diffusion of small cytoplasmic molecules, ions, and water. Metabolites including adenosine triphosphate (ATP) and glutathione also can move through gap junction channels. Several functions have been ascribed to gap junctions including metabolite sharing, electrical coupling, cell growth control, and regulation of cell migration.

Intercellular communication pathways between alveolar epithelial cells which control surfactant secretion. Gap junctional transmission (1) of either calcium or inositol trisphosphate (IP3) generates increased cytosolic calcium in type II cells, which, in turn, could stimulate surfactant secretion either through protein kinase C activation or through a direct effect of calcium on lamellar body fusion. Increased cytosolic calcium can also be mediated through secretion of ATP through P2X7 receptor-mediated pannexin channels (2) acting on P2Y2 purinergic receptors. Protein kinase A activation through stimulation of A2 purinergic receptors by ATP can also occur (3). Adapted from [46]
The proteins that form gap junctions are known as connexins. In the alveoli, connexin-43 (Cx43) is the major connexin demonstrated to have functional roles [45–49]. Other connexins expressed by the alveolar epithelium include Cx26, Cx32, Cx30.3, Cx40, and Cx46. Specific roles for these other connexins in the alveolar epithelium have not been elucidated. Among these, Cx32 is restricted to type II cells and is absent from type I cells [50, 51]. Moreover, type I cells cannot form functional gap junctions with cells expressing only Cx32; however, type II cells readily communicate through Cx32 gap junction channels [51]. Although type I cells can form functional heterocellular gap junctions with type II cells via Cx43, roles for Cx32 in regulating alveolar signaling remain unknown at present. One possibility is that Cx32 provides a “priority channel” where type II cells can specifically communicate with each other, but this has yet to be determined.
Alcohol treatment of cells in vitro inhibits gap junctional communication [52–55]. Specifically, alcohol significantly inhibits expression of the major lung connexin, Cx43 [52, 53], but has less effect on other connexins [52, 54]. A direct mechanism for the effect of alcohol on gap junctions is by partitioning into membranes and changing the connexin microenvironment [56]. Hormones induced by chronic alcohol ingestion can also have deleterious effects on alveolar gap junctions. Most notably, TGF-β inhibits alveolar Cx43 expression [55]. Moreover, glutathione depletion and increased oxidant stress induced by chronic alcohol exposure also decrease gap junctional communication [57, 58]. Although a reduction in gap junctions in response to oxidant stress reduces intercellular signaling, it can be beneficial since it decreases the transfer of toxic agents and thus minimizes tissue damage [59, 60]. However, this is at the expense of promoting the transfer of protective agents including glutathione.
Recently, a novel mode of Cx43-dependent interaction in the alveolus was demonstrated by showing that bone-marrow-derived stromal cells (BMSCs) instilled into injured lungs formed functional gap junctions with type II cells in vivo [61]. This interaction was particularly critical for preventing cell injury due to insufficient mitochondrial function. In part, this could be due to direct transfer of metabolites from healthy BMSCs to damaged type II cells. More provocatively, evidence was provided showing direct mitochondrial transfer from the BMSCs to the type II cells, which also appeared to require functional gap junctions. Gap junction permeability is too limited to enable direct movement of mitochondria through channels themselves. Instead, mitochondrial transfer was due to microvesicles that were taken up by type II cells. It is plausible that this gap junction plaque endocytosis could enable mitochondrial transfer since, during this process, the plasma membrane and a small amount of cytosol are taken up by the neighboring cell [62]. Regardless of the specific mechanism, if a mitochondrial transfer pathway is critical for ameliorating lung injury then it is likely to be adversely affected by alcohol, which impairs both gap junctional communication (see above) and mitochondrial function [63].
Gap junctions play an important role in regulating the secretion of pulmonary surfactant produced by type II alveolar epithelial cells. Mechanical distension of type I cells in the alveolus occurs during a physical stretch, for example a deep breath or assisted ventilation, which then initiates a transient increase in cytosolic calcium through stretch-activated channels. The calcium is then transmitted through gap junctions from type I cells to type II cells where it stimulates fusion of lamellar bodies with the plasma membranes to release surfactant [64–66].
Paracrine Signaling
In addition to gap junctional communication, intercellular calcium transients can also be generated by extracellular ATP release and paracrine stimulation of purinergic receptors that can also promote surfactant secretion (Fig. 8.5) [67–70]. This provides a system where multiple pathways can promote intercellular signaling and surfactant release. In type II cells, P2Y2 receptors are the primary targets for paracrine ATP signaling that induce calcium transients through a G-protein-coupled mechanism [71]. Alveolar epithelial cells also express P2X-type purinergic receptors and L-type voltage-gated calcium channels that can initiate calcium transients involved in surfactant secretion [72, 73].
By contrast, type I cells express high levels of P2X7 purinergic receptors [74, 75]. P2X7 receptors differ from other classes of purinergic receptors in that they are linked to a high conductance pore composed of proteins known as pannexins [76]. Thus, ATP stimulation of P2X7 receptors induces additional ATP release, acting as a feed-forward loop to further amplify purinergic signaling. Consistent with this, cocultures of type I and type II cells are more sensitive to stretch-induced surfactant lipid secretion than type II cells in monoculture [67]. The enhanced lipid secretion by cocultures was due to the sensitivity of type I cells to mechanical stimulation. In response to ~20 % stretch, type I cells released fourfold more ATP than type II cells. This supports the hypothesis that type I cells are mechanosensors and that paracrine stimulation of type II cells by extracellular ATP regulates surfactant secretion.
Pulmonary Surfactant
Pulmonary surfactant is a mixture of proteins and lipids synthesized by type II cells that lines the alveolar airspace. Surfactant prevents atelectasis by reducing airspace surface tension that would otherwise cause lung collapse due to the pressure of fluid filled tissues. The major proteins found in pulmonary surfactant are SP-A, SP-B, SP-C, and SP-D.
Two of these, SP-B and SP-C, are hydrophobic and interact with surfactant lipid components to create a surface active mixture [77, 78]. By contrast, SP-A and SP-D are members of the collectin protein family and serve as part of the innate immune system by opsonizing bacteria, viruses, and other foreign agents [79–82]. Both SP-A and SP-D have carbohydrate recognition domains that bind to polysaccharides, while the collagenous stalk region of the proteins is recognized by phagocytes in the airspaces. However, SP-A and SP-D also play key roles in regulating pulmonary surfactant as well. SP-A promotes surfactant lipid turnover by mediating surfactant uptake by type II cells [83]. SP-D also helps regulate surfactant degradation by macrophages and type II cells, as evidenced by the observation that this function is impaired in SP-D-deficient mice [84, 85].
The majority of surfactant lipid is phosphatidylcholine, with phosphatidylglycerol and phosphatidylethanolamine as the other major phospholipids present [86]. Moreover, most surfactant lipid contains saturated fatty acids, the bulk of which is dipalmitoyl-phosphatidylcholine. Saturated fatty acids are fairly unreactive as opposed to unsaturated lipids present in surfactant and cell membranes that are readily oxidized [87, 88]. Oxidant damage to type II cells alters their ability to synthesize surfactant lipids, which further compromises its surface activity [89, 90].
Given the negative impact of oxidant stress on surfactant function it is not surprising that surfactant production is impaired in the alcoholic lung. Surfactant lipid synthesis, secretion, and function are all impaired by chronic alcohol ingestion in rats as a result of glutathione depletion [17, 18]. Procysteine administered as a redox protective strategy restored the ability of type II cells to produce functional surfactant. Interestingly, N-acetyl cysteine was ineffective, since it can only compensate for cytosolic glutathione, whereas procysteine can also replenish mitochondrial glutathione [17]. Exposure to alcohol in utero also has a negative impact on production of several surfactant lipids, indicating that oxidant stress can occur in the absence of atmospheric oxygen [91]. This is significant, since it suggests that pulmonary complications are a likely complication of fetal alcohol exposure, particularly in preterm infants [92].
Alveolar Wound Repair and Extracellular Matrix
Lung epithelia are susceptible to environmental insults and are in varying states of repair ranging from baseline turnover to recovery from acute injury. Acute and chronic alcohol consumption has been shown to alter the repair of damaged epithelial tissues. Much of what has been learned about wound repair is from studies of patient recovery from skin trauma [93]. Of particular relevance to alveolar epithelium is that the state and remodeling of the extracellular matrix are impaired as a result of alcohol ingestion.
Cells interact with the extracellular matrix as a means of regulating homeostasis and cell proliferation. Normal alveolar cells interact with an extracellular matrix containing several proteins, including laminin and type IV collagen [94, 95]. When the alveolus is injured, the matrix is destroyed and replaced with a provisional matrix of fibronectin and type I collagen that stimulates cell migration and wound healing [96–100]. Interestingly, fibronectin also stimulates alveolar epithelial cells to more rapidly form a high resistance barrier as opposed to cells on a matrix with basal composition [101, 102]. This is due to enhanced spreading of the cells on a fibronectin-enriched matrix. Although initially beneficial to the lung, barriers formed by alveolar epithelial cells on fibronectin over the long term have lower resistance than barriers formed by cells on laminin or collagen [102].
Therefore, healthy alveolar repair requires that the extracellular matrix is remodeled back to a state rich in laminin and type IV collagen. If this does not occur, then persistent fibronectin will cause an exaggerated inflammatory response and fibroproliferation that can permanently damage the alveolar epithelium [103, 104]. In response to chronic alcohol exposure, fibronectin expression in the lung is significantly increased [105, 106]. Increased fibronectin, in conjunction with other aspects of the alcoholic lung (e.g., oxidant stress and increased TGF-β), provides an alveolar microenvironment primed for aberrant repair in response to lung injury.
Summary
In order to withstand the environmental stresses of alcohol, the lung has to compensate for several changes that are not present in the normal lung. Chief among these is increased oxidant stress. To some extent, there is overt damage to the alveolar epithelium as a direct result of oxidant exposure. However, the lung epithelium also adapts through subtle changes in phenotype. Hallmarks of the alcoholic lung are similar to changes that occur during lung injury; however they are more limited in scale. Therefore, as previously mentioned the otherwise healthy alcoholic has no clinically detectable evidence of alveolar dysfunction. However, these phenotypic changes predispose the alveolus for an exaggerated response when subjected to the added injury of a “second hit” such as ventilator-induced lung injury or sepsis.
Two key aspects of alveolar function are particularly impaired in response to alcohol exposure and have a significant impact on the severity of acute lung injury, namely impaired surfactant production and barrier dysfunction. Most of the effects of alcohol on pulmonary surfactant diminish the surface active lipid component rather than the protein component. However, when coupled with the added impact of alcohol on host defense, even a small effect on collectin family surfactant proteins is likely to be amplified. Given difficulties in using surfactant augmentation therapy in adult lung injury [107], it seems likely that the best approach is to target improving the immune response or attenuating inflammation rather than directly manipulating the surfactant pool in the adult alcoholic lung.
An impaired alveolar barrier is perhaps the more serious consequence of alcohol and likely has a major impact on the severity of acute lung injury because of the effects of alveolar flooding on gas exchange [108]. As discussed earlier, increased fluid clearance can compensate for some deficiencies in alveolar tight junctions. However, the capacity for up-regulated fluid clearance is not unlimited. Progress in understanding how alcohol affects the expression and assembly of alveolar tight junctions has identified several potential therapeutic targets to improve alveolar barrier function. Given that alveolar tight junctions are remodeled in response to alcohol, this suggests that a successful therapeutic approach targeting the alveolar epithelium may require normalizing tight junction protein composition. Alternatively, given the profound effects of alcohol that diminish tight junction stability, pharmacologic approaches to stabilize incorporation of claudins into tight junctions may prove to be a useful approach to minimize alveolar flooding due to barotrauma.
References
Jean JC, Liu Y, Brown LA, Marc RE, Klings E, Joyce-Brady M. Gamma-glutamyl transferase deficiency results in lung oxidant stress in normoxia. Am J Physiol. 2002;283(4): L766–76.
Holguin F, Moss I, Brown LA, Guidot DM. Chronic ethanol ingestion impairs alveolar type II cell glutathione homeostasis and function and predisposes to endotoxin-mediated acute edematous lung injury in rats. J Clin Invest. 1998;101(4):761–8.
Moss M, Guidot DM, Wong-Lambertina M, Ten Hoor T, Perez RL, Brown LA. The effects of chronic alcohol abuse on pulmonary glutathione homeostasis. Am J Respir Crit Care Med. 2000;161(2 Pt 1):414–9.
Lois M, Brown LA, Moss IM, Roman J, Guidot DM. Ethanol ingestion increases activation of matrix metalloproteinases in rat lungs during acute endotoxemia. Am J Respir Crit Care Med. 1999;160(4):1354–60.
Joshi PC, Guidot DM. The alcoholic lung: epidemiology, pathophysiology, and potential therapies. Am J Physiol. 2007;292(4):L813–23.
Moss M, Parsons PE, Steinberg KP, Hudson LD, Guidot DM, Burnham EL, et al. Chronic alcohol abuse is associated with an increased incidence of acute respiratory distress syndrome and severity of multiple organ dysfunction in patients with septic shock. Crit Care Med. 2003;31(3):869–77.
Brown LA, Harris FL, Ping XD, Gauthier TW. Chronic ethanol ingestion and the risk of acute lung injury: a role for glutathione availability? Alcohol (Fayetteville, NY). 2004;33(3): 191–7.
Bechara RI, Pelaez A, Palacio A, Joshi PC, Hart CM, Brown LA, et al. Angiotensin II mediates glutathione depletion, transforming growth factor-beta1 expression, and epithelial barrier dysfunction in the alcoholic rat lung. Am J Physiol. 2005;289(3):L363–70.
Jardine H, MacNee W, Donaldson K, Rahman I. Molecular mechanism of transforming growth factor (TGF)-beta1-induced glutathione depletion in alveolar epithelial cells. Involvement of AP-1/ARE and Fra-1. J Biol Chem. 2002;277(24):21158–66.
Arsalane K, Dubois CM, Muanza T, Begin R, Boudreau F, Asselin C, et al. Transforming growth factor-beta1 is a potent inhibitor of glutathione synthesis in the lung epithelial cell line A549: transcriptional effect on the GSH rate-limiting enzyme gamma-glutamylcysteine synthetase. Am J Respir Cell Mol Biol. 1997;17(5):599–607.
Hsu YC, Wang LF, Chien YW. Nitric oxide in the pathogenesis of diffuse pulmonary fibrosis. Free Radic Biol Med. 2007;42(5):599–607.
Sturrock A, Cahill B, Norman K, Huecksteadt TP, Hill K, Sanders K, et al. Transforming growth factor-beta1 induces Nox4 NAD(P)H oxidase and reactive oxygen species-dependent proliferation in human pulmonary artery smooth muscle cells. Am J Physiol. 2006;290(4): L661–73.
Waghray M, Cui Z, Horowitz JC, Subramanian IM, Martinez FJ, Toews GB, et al. Hydrogen peroxide is a diffusible paracrine signal for the induction of epithelial cell death by activated myofibroblasts. Faseb J. 2005;19(7):854–6.
Munger JS, Huang X, Kawakatsu H, Griffiths MJ, Dalton SL, Wu J, et al. The integrin alpha v beta 6 binds and activates latent TGF beta 1: a mechanism for regulating pulmonary inflammation and fibrosis. Cell. 1999;96(3):319–28.
Pittet JF, Griffiths MJ, Geiser T, Kaminski N, Dalton SL, Huang X, et al. TGF-beta is a critical mediator of acute lung injury. J Clin Invest. 2001;107(12):1537–44.
Brown LA, Harris FL, Guidot DM. Chronic ethanol ingestion potentiates TNF-alpha-mediated oxidative stress and apoptosis in rat type II cells. Am J Physiol. 2001;281(2): L377–86.
Guidot DM, Brown LA. Mitochondrial glutathione replacement restores surfactant synthesis and secretion in alveolar epithelial cells of ethanol-fed rats. Alcohol Clin Exp Res. 2000; 24(7):1070–6.
Velasquez A, Bechara RI, Lewis JF, Malloy J, McCaig L, Brown LA, et al. Glutathione replacement preserves the functional surfactant phospholipid pool size and decreases sepsis-mediated lung dysfunction in ethanol-fed rats. Alcohol Clin Exp Res. 2002;26(8):1245–51.
Bernard GR, Wheeler AP, Arons MM, Morris PE, Paz HL, Russell JA, et al. A trial of antioxidants N-acetylcysteine and procysteine in ARDS. The Antioxidant in ARDS Study Group. Chest. 1997;112(1):164–72.
Adhikari N, Burns KE, Meade MO. Pharmacologic treatments for acute respiratory distress syndrome and acute lung injury: systematic review and meta-analysis. Treat Respir Med. 2004;3(5):307–28. Epub 2004/12/21.
DeCarli LM, Lieber CS. Fatty liver in the rat after prolonged intake of ethanol with a nutritionally adequate new liquid diet. J Nutr. 1967;91(3):331–6. Epub 1967/03/01.
Guidot DM, Modelska K, Lois M, Jain L, Moss IM, Pittet JF, et al. Ethanol ingestion via glutathione depletion impairs alveolar epithelial barrier function in rats. Am J Physiol. 2000;279(1):L127–35.
Garcia O, Buckley S, Navarro S, Driscoll B, Warburton D. Modulating the alveolar milieu to enhance resolution of fibrotic lung injury. Proc Am Thorac Soc. 2012;9(3):117–9. Epub 2012/07/18.
Liu Y, Balaraman Y, Wang G, Nephew KP, Zhou FC. Alcohol exposure alters DNA methylation profiles in mouse embryos at early neurulation. Epigenetics. 2009;4(7):500–11. Epub 2009/12/17.
Zahs A, Curtis BJ, Waldschmidt TJ, Brown LA, Gauthier TW, Choudhry MA, et al. Alcohol and epigenetic changes: summary of the 2011 Alcohol and Immunology Research Interest Group (AIRIG) meeting. Alcohol (Fayetteville, NY). 2012;46(8):783–7.
Koval M. Claudin heterogeneity and control of lung tight junctions. Annu Rev Physiol. 2012;75:551–67. Epub 2012/10/18.
Umeda K, Ikenouchi J, Katahira-Tayama S, Furuse K, Sasaki H, Nakayama M, et al. ZO-1 and ZO-2 independently determine where claudins are polymerized in tight-junction strand formation. Cell. 2006;126(4):741–54.
Raleigh DR, Marchiando AM, Zhang Y, Shen L, Sasaki H, Wang Y, et al. Tight junction-associated MARVEL proteins marveld3, tricellulin, and occludin have distinct but overlapping functions. Mol Biol Cell. 2010;21(7):1200–13. Epub 2010/02/19.
Fan X, Joshi PC, Koval M, Guidot DM. Chronic alcohol ingestion exacerbates lung epithelial barrier dysfunction in HIV-1 transgenic rats. Alcohol Clin Exp Res. 2011;35(10):1866–75. Epub 2011/05/17.
Joshi PC, Mehta A, Jabber WS, Fan X, Guidot DM. Zinc deficiency mediates alcohol-induced alveolar epithelial and macrophage dysfunction in rats. Am J Respir Cell Mol Biol. 2009;41(2):207–16. Epub 2008/12/26.
Lafemina MJ, Rokkam D, Chandrasena A, Pan J, Bajaj A, Johnson M, et al. Keratinocyte growth factor enhances barrier function without altering claudin expression in primary alveolar epithelial cells. Am J Physiol. 2010;299(6):L724–34.
Mitchell LA, Overgaard CE, Ward C, Margulies SS, Koval M. Differential effects of claudin-3 and claudin-4 on alveolar epithelial barrier function. Am J Physiol. 2011;301(1):L40–9.
Rokkam D, Lafemina MJ, Lee JW, Matthay MA, Frank JA. Claudin-4 levels are associated with intact alveolar fluid clearance in human lungs. Am J Pathol. 2011;179(3):1081–7. Epub 2011/07/12.
Wray C, Mao Y, Pan J, Chandrasena A, Piasta F, Frank JA. Claudin 4 augments alveolar epithelial barrier function and is induced in acute lung injury. Am J Physiol. 2009;297(2): L219–27.
Fang X, Neyrinck AP, Matthay MA, Lee JW. Allogeneic human mesenchymal stem cells restore epithelial protein permeability in cultured human alveolar type II cells by secretion of angiopoietin-1. J Biol Chem. 2010;285(34):26211–22.
Fernandez AL, Koval M, Fan X, Guidot DM. Chronic alcohol ingestion alters claudin expression in the alveolar epithelium of rats. Alcohol (Fayetteville, NY). 2007;41(5):371–9.
Overgaard CE, Mitchell LA, Koval M. Roles for claudins in alveolar epithelial barrier function. Ann N Y Acad Sci. 2012;1257:167–74.
Coyne CB, Gambling TM, Boucher RC, Carson JL, Johnson LG. Role of claudin interactions in airway tight junctional permeability. Am J Physiol. 2003;285(5):L1166–78.
Wang F, Daugherty B, Keise LL, Wei Z, Foley JP, Savani RC, et al. Heterogeneity of claudin expression by alveolar epithelial cells. Am J Respir Cell Mol Biol. 2003;29(1):62–70.
Eaton DC, Helms MN, Koval M, Bao HF, Jain L. The contribution of epithelial sodium channels to alveolar function in health and disease. Annu Rev Physiol. 2009;71:403–23.
Otis JS, Mitchell PO, Kershaw CD, Joshi PC, Guidot DM. Na, K-ATPase expression is increased in the lungs of alcohol-fed rats. Alcohol Clin Exp Res. 2008;32(4):699–705.
Downs CA, Trac DQ, Kreiner LH, Eaton AF, Johnson NM, Brown LA, et al. Ethanol alters alveolar fluid balance via nadph oxidase (NOX) signaling to epithelial sodium channels (ENaC) in the lung. PLoS One. 2013;8(1):e54750. Epub 2013/02/06.
Goodson P, Kumar A, Jain L, Kundu K, Murthy N, Koval M, et al. NADPH oxidase regulates alveolar epithelial sodium channel activity and lung fluid balance in vivo via O(−)(2) signaling. Am J Physiol. 2012;302(4):L410–9. Epub 2011/12/14.
Takemura Y, Goodson P, Bao HF, Jain L, Helms MN. Rac1-mediated NADPH oxidase release of O2- regulates epithelial sodium channel activity in the alveolar epithelium. Am J Physiol. 2010;298(4):L509–20. Epub 2010/01/26.
Chatterjee S, Baeter S, Bhattacharya J. Endothelial and epithelial signaling in the lung. Am J Physiol. 2007;293(3):L517–9.
Koval M. Sharing signals: connecting lung epithelial cells with gap junction channels. Am J Physiol. 2002;283(5):L875–93.
Koval M. Connexins, tissue expression. In: Laurent GJ, Shapiro SD, editors. Encyclopedia of respiratory medicine. Oxford: Elsevier; 2006. p. 558–60.
Alford AI, Rannels DE. Extracellular matrix fibronectin alters connexin43 expression by alveolar epithelial cells. Am J Physiol. 2001;280(4):L680–8.
Andreeva AV, Kutuzov MA, Voyno-Yasenetskaya TA. Regulation of surfactant secretion in alveolar type II cells. Am J Physiol. 2007;293(2):L259–71.
Abraham V, Chou ML, DeBolt KM, Koval M. Phenotypic control of gap junctional communication by cultured alveolar epithelial cells. Am J Physiol. 1999;276(5 Pt 1):L825–34.
Abraham V, Chou ML, George P, Pooler P, Zaman A, Savani RC, et al. Heterocellular gap junctional communication between alveolar epithelial cells. Am J Physiol. 2001;280(6): L1085–93.
Wentlandt K, Kushnir M, Naus CC, Carlen PL. Ethanol inhibits gap-junctional coupling between P19 cells. Alcohol Clin Exp Res. 2004;28(9):1284–90.
Bokkala S, Reis HM, Rubin E, Joseph SK. Effect of angiotensin II and ethanol on the expression of connexin 43 in WB rat liver epithelial cells. Biochem J. 2001;357(Pt 3):769–77.
Abou Hashieh I, Mathieu S, Besson F, Gerolami A. Inhibition of gap junction intercellular communications of cultured rat hepatocytes by ethanol: role of ethanol metabolism. J Hepatol. 1996;24(3):360–7.
Johnson LN, Koval M. Cross-talk between pulmonary injury, oxidant stress, and gap junctional communication. Antioxid Redox Signal. 2009;11(2):355–67.
Johnston MF, Simon SA, Ramon F. Interaction of anaesthetics with electrical synapses. Nature. 1980;286(5772):498–500.
Todt I, Ngezahayo A, Ernst A, Kolb HA. Hydrogen peroxide inhibits gap junctional coupling and modulates intracellular free calcium in cochlear Hensen cells. J Membr Biol. 2001; 181(2):107–14.
Upham BL, Kang KS, Cho HY, Trosko JE. Hydrogen peroxide inhibits gap junctional intercellular communication in glutathione sufficient but not glutathione deficient cells. Carcinogenesis. 1997;18(1):37–42.
Azzam EI, de Toledo SM, Little JB. Direct evidence for the participation of gap junction-mediated intercellular communication in the transmission of damage signals from alpha-particle irradiated to nonirradiated cells. Proc Natl Acad Sci U S A. 2001;98(2):473–8.
Elshami AA, Saavedra A, Zhang H, Kucharczuk JC, Spray DC, Fishman GI, et al. Gap junctions play a role in the ‘bystander effect’ of the herpes simplex virus thymidine kinase/ganciclovir system in vitro. Gene Ther. 1996;3(1):85–92.
Islam MN, Das SR, Emin MT, Wei M, Sun L, Westphalen K, et al. Mitochondrial transfer from bone-marrow-derived stromal cells to pulmonary alveoli protects against acute lung injury. Nat Med. 2012;18(5):759–65. Epub 2012/04/17.
Laird DW. Life cycle of connexins in health and disease. Biochem J. 2006;394(Pt 3): 527–43.
Brown LA, Harris FL, Bechara R, Guidot DM. Effect of chronic ethanol ingestion on alveolar type II cell: glutathione and inflammatory mediator-induced apoptosis. Alcohol Clin Exp Res. 2001;25(7):1078–85. Epub 2001/08/16.
Kuebler WM, Parthasarathi K, Lindert J, Bhattacharya J. Real-time lung microscopy. J Appl Physiol. 2007;102(3):1255–64.
Ashino Y, Ying X, Dobbs LG, Bhattacharya J. [Ca2+]i oscillations regulate type II cell exocytosis in the pulmonary alveolus. Am J Physiol. 2000;279(1):L5–13.
Wang PM, Fujita E, Bhattacharya J. Vascular regulation of type II cell exocytosis. Am J Physiol. 2002;282(5):L912–6.
Patel AS, Reigada D, Mitchell CH, Bates SR, Margulies SS, Koval M. Paracrine stimulation of surfactant secretion by extracellular ATP in response to mechanical deformation. Am J Physiol. 2005;289(3):L489–96.
Isakson BE, Seedorf GJ, Lubman RL, Evans WH, Boitano S. Cell-cell communication in heterocellular cultures of alveolar epithelial cells. Am J Respir Cell Mol Biol. 2003;29(5): 552–61.
Isakson BE, Evans WH, Boitano S. Intercellular Ca2+ signaling in alveolar epithelial cells through gap junctions and by extracellular ATP. Am J Physiol. 2001;280(2):L221–8.
Rooney SA. Regulation of surfactant secretion. Comp Biochem Physiol A Mol Integr Physiol. 2001;129(1):233–43.
Yang C, Su L, Wang Y, Liu L. UTP regulation of ion transport in alveolar epithelial cells involves distinct mechanisms. Am J Physiol. 2009;297(3):L439–54. Epub 2009/06/23.
Dietl P, Haller T, Wirleitner B, Volkl H, Friedrich F, Striessnig J. Activation of L-type Ca2+ channels after purinoceptor stimulation by ATP in an alveolar epithelial cell (L2). Am J Physiol. 1995;269(6 Pt 1):L873–83. Epub 1995/12/01.
Sen N, Grunstein MM, Chander A. Stimulation of lung surfactant secretion by endothelin-1 from rat alveolar type II cells. Am J Physiol. 1994;266(3 Pt 1):L255–62. Epub 1994/03/01.
Chen Z, Jin N, Narasaraju T, Chen J, McFarland LR, Scott M, et al. Identification of two novel markers for alveolar epithelial type I and II cells. Biochem Biophys Res Commun. 2004;319(3):774–80.
Mishra A, Chintagari NR, Guo Y, Weng T, Su L, Liu L. Purinergic P2X7 receptor regulates lung surfactant secretion in a paracrine manner. J Cell Sci. 2011;124(Pt 4):657–68.
Penuela S, Gehi R, Laird DW. The biochemistry and function of pannexin channels. Biochim Biophys Acta. 2013;1828(1):15–22. Epub 2012/02/07.
Beers MF, Mulugeta S. Surfactant protein C biosynthesis and its emerging role in conformational lung disease. Annu Rev Physiol. 2005;67:663–96.
Whitsett JA, Weaver TE. Hydrophobic surfactant proteins in lung function and disease. N Engl J Med. 2002;347(26):2141–8.
Giannoni E, Sawa T, Allen L, Wiener-Kronish J, Hawgood S. Surfactant proteins A and D enhance pulmonary clearance of Pseudomonas aeruginosa. Am J Respir Cell Mol Biol. 2006;34(6):704–10.
Wright JR. Immunoregulatory functions of surfactant proteins. Nat Rev Immunol. 2005; 5(1): 58–68.
Hartshorn KL, White MR, Voelker DR, Coburn J, Zaner K, Crouch EC. Mechanism of binding of surfactant protein D to influenza A viruses: importance of binding to haemagglutinin to antiviral activity. Biochem J. 2000;351(Pt 2):449–58.
LeVine AM, Elliott J, Whitsett JA, Srikiatkhachorn A, Crouch E, DeSilva N, et al. Surfactant protein-d enhances phagocytosis and pulmonary clearance of respiratory syncytial virus. Am J Respir Cell Mol Biol. 2004;31(2):193–9.
Bates SR, Dodia C, Tao JQ, Fisher AB. Surfactant protein-A plays an important role in lung surfactant clearance: evidence using the surfactant protein-A gene-targeted mouse. Am J Physiol. 2008;294(2):L325–33. Epub 2007/12/18.
Botas C, Poulain F, Akiyama J, Brown C, Allen L, Goerke J, et al. Altered surfactant homeostasis and alveolar type II cell morphology in mice lacking surfactant protein D. Proc Natl Acad Sci U S A. 1998;95(20):11869–74. Epub 1998/09/30.
King BA, Kingma PS. Surfactant protein D deficiency increases lung injury during endotoxemia. Am J Respir Cell Mol Biol. 2011;44(5):709–15. Epub 2010/07/20.
Veldhuizen R, Nag K, Orgeig S, Possmayer F. The role of lipids in pulmonary surfactant. Biochim Biophys Acta. 1998;1408(2–3):90–108.
Sosenko IR, Innis SM, Frank L. Polyunsaturated fatty acids and protection of newborn rats from oxygen toxicity. J Pediatr. 1988;112(4):630–7.
Putman E, Liese W, Voorhout WF, van Bree L, van Golde LM, Haagsman HP. Short-term ozone exposure affects the surface activity of pulmonary surfactant. Toxicol Appl Pharmacol. 1997;142(2):288–96.
Crim C, Longmore WJ. Sublethal hydrogen peroxide inhibits alveolar type II cell surfactant phospholipid biosynthetic enzymes. Am J Physiol. 1995;268(1 Pt 1):L129–35.
Minoo P, King RJ, Coalson JJ. Surfactant proteins and lipids are regulated independently during hyperoxia. Am J Physiol. 1992;263(2 Pt 1):L291–8.
Sozo F, Vela M, Stokes V, Kenna K, Meikle PJ, De Matteo R, et al. Effects of prenatal ethanol exposure on the lungs of postnatal lambs. Am J Physiol. 2011;300(1):L139–47.
Giliberti D, Mohan SS, Brown LA, Gauthier TW. Perinatal exposure to alcohol: implications for lung development and disease. Paediatr Respir Rev. 2013;14(1):17–21.
Radek KA, Ranzer MJ, Dipietro LA. Brewing complications: the effect of acute ethanol exposure on wound healing. J Leukoc Biol. 2009;86(5):1125–34.
Crouch EC, Martin GR, Brody JS, Laurie GW. Basement Membranes. In: Crystal RG, West JB, Weibel ER, Barnes PJ, editors. The lung: scientific foundations. Philadelphia, PA: Lippincott-Raven; 1997. p. 769–91.
Pelosi P, Rocco PR. Effects of mechanical ventilation on the extracellular matrix. Intensive Care Med. 2008;34(4):631–9.
Chapman HA. Disorders of lung matrix remodeling. J Clin Invest. 2004;113(2):148–57.
Roman J. Extracellular matrix and lung inflammation. Immunol Res. 1996;15(2):163–78.
Kim HJ, Henke CA, Savik SK, Ingbar DH. Integrin mediation of alveolar epithelial cell migration on fibronectin and type I collagen. Am J Physiol. 1997;273(1 Pt 1):L134–41.
Rickard KA, Taylor J, Rennard SI, Spurzem JR. Migration of bovine bronchial epithelial cells to extracellular matrix components. Am J Respir Cell Mol Biol. 1993;8(1):63–8.
Garat C, Kheradmand F, Albertine KH, Folkesson HG, Matthay MA. Soluble and insoluble fibronectin increases alveolar epithelial wound healing in vitro. Am J Physiol. 1996;271(5 Pt 1):L844–53.
Sugahara K, Kiyota T, Clark RA, Mason RJ. The effect of fibronectin on cytoskeleton structure and transepithelial resistance of alveolar type II cells in primary culture. Virchows Arch. 1993;64(2):115–22.
Koval M, Ward C, Findley MK, Roser-Page S, Helms MN, Roman J. Extracellular matrix influences alveolar epithelial claudin expression and barrier function. Am J Respir Cell Mol Biol. 2010;42(2):172–80.
Hernnas J, Nettelbladt O, Bjermer L, Sarnstrand B, Malmstrom A, Hallgren R. Alveolar accumulation of fibronectin and hyaluronan precedes bleomycin-induced pulmonary fibrosis in the rat. Eur Respir J. 1992;5(4):404–10.
Roman J, Ritzenthaler JD, Bechara R, Brown LA, Guidot D. Ethanol stimulates the expression of fibronectin in lung fibroblasts via kinase-dependent signals that activate CREB. Am J Physiol. 2005;288(5):L975–87.
Brown LA, Ritzenthaler JD, Guidot DM, Roman J. Alveolar type II cells from ethanol-fed rats produce a fibronectin-enriched extracellular matrix that promotes monocyte activation. Alcohol (Fayetteville, NY). 2007;41(5):317–24.
Burnham EL, Moss M, Ritzenthaler JD, Roman J. Increased fibronectin expression in lung in the setting of chronic alcohol abuse. Alcohol Clin Exp Res. 2007;31(4):675–83.
Lewis JF, Jobe AH. Surfactant and the adult respiratory distress syndrome. Am Rev Respir Dis. 1993;147(1):218–33.
Ware LB, Matthay MA. Alveolar fluid clearance is impaired in the majority of patients with acute lung injury and the acute respiratory distress syndrome. Am J Respir Crit Care Med. 2001;163(6):1376–83.
Daugherty BL, Mateescu M, Patel AS, Wade K, Kimura S, Gonzales LW, et al. Developmental regulation of claudin localization by fetal alveolar epithelial cells. Am J Physiol. 2004; 287(6):L1266–73.
Kaarteenaho R, Merikallio H, Lehtonen S, Harju T, Soini Y. Divergent expression of claudin −1, -3, -4, -5 and −7 in developing human lung. Respir Res. 2010;11:59. Epub 2010/05/19.
Kaarteenaho-Wiik R, Soini Y. Claudin-1, -2, -3, -4, -5, and −7 in usual interstitial pneumonia and sarcoidosis. J Histochem Cytochem. 2009;57(3):187–95.
Chen SP, Zhou B, Willis BC, Sandoval AJ, Liebler JM, Kim KJ, et al. Effects of transdifferentiation and EGF on claudin isoform expression in alveolar epithelial cells. J Appl Physiol. 2005;98(1):322–8.
Mazzon E, Cuzzocrea S. Role of TNF-alpha in lung tight junction alteration in mouse model of acute lung inflammation. Respir Res. 2007;8:75.
Ohta H, Chiba S, Ebina M, Furuse M, Nukiwa T. Altered expression of tight junction molecules in alveolar septa in lung injury and fibrosis. Am J Physiol. 2012;302(2):L193–205. Epub 2011/10/18.
Crapo JD, Barry BE, Gehr P, Bachofen M, Weibel ER. Cell number and cell characteristics of the normal human lung. Am Rev Respir Dis. 1982;126(2):332–7.
Laukoetter MG, Nava P, Lee WY, Severson EA, Capaldo CT, Babbin BA, et al. JAM-A regulates permeability and inflammation in the intestine in vivo. J Exp Med. 2007;204(13): 3067–76.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Molina, S.A., Koval, M. (2014). Alcohol and the Alveolar Epithelium. In: Guidot, D., Mehta, A. (eds) Alcohol Use Disorders and the Lung. Respiratory Medicine, vol 14. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4614-8833-0_8
Download citation
DOI: https://doi.org/10.1007/978-1-4614-8833-0_8
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4614-8832-3
Online ISBN: 978-1-4614-8833-0
eBook Packages: MedicineMedicine (R0)