
Abstract
This paper addresses play for the elderly, and how playware can act as a play force that pushes people into a play dynamics. Play is a free and voluntary activity that we do for no other purpose than the play and enjoyment. Nevertheless, we may observe collateral effects of play amongst the elderly, e.g. in terms of health effects. The paper presents both qualitative and quantitative studies of the effect of play amongst elderly. For instance, it is shown how playful training on modular interactive tiles show statistical significant effects on all the test measures of elderly functional abilities (e.g. balancing, strength, mobility, agility, endurance) after merely 13 group training sessions during which each elderly play (exercise) for just 12–13 min. Hence, the statistical significant effects are obtained after just 2–3 h of total playing time with such playful technology. In play, the elderly seem to forget about time and place (e.g. forget about their possible fear of falling and physical limitations), and thereby achieve the remarkable collateral effect on their health.
You have full access to this open access chapter, Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Play is a free and voluntary activity that we do for no other purpose than play itself. We do not play to achieve a certain outcome or product, but we play for the pleasure and enjoyment that we feel while playing. Nevertheless, under various circumstances, we may observe certain effects of play. For the one who plays, these effects are not the primary reason to engage in play. Therefore, we term such effects the collateral effects of play. The collateral effects of play can be educational achievements, motor skill enhancement, cognitive and physical rehabilitation, etc. These collateral effects of play can be significant and important, but it is essential to understand that play is a self-sustaining phenomenon which carries its purpose in itself. Compared to other human activities, in its pure form, play does not lead to anything; it neither creates nor produces anything, except for play:
-
Play is a free, voluntary activity indulged for its own sake, and although creative, play is unproductive and non-utilitarian. Play has boundaries of space and time, and takes place temporarily outside ‘regular life,’ with its own course and meaning [1].
Likewise the French play theoretician Roger Caillois emphasizes the unproductive and voluntary nature of play:
-
Play is characterized as free (not obligatory); separate (isolated in space and time); uncertain (indeterminable); unproductive (without material production); governed by rules (contingent conventions); and make-believe (suspension of disbelief) [2].
Huizinga describes play as a separate life sphere, which existence cannot and shall not be legitimized with outer purposes. The notion of play as a separate life sphere is summarized by Gadamer: When human beings engage themselves in playing, an “ontological shift” occurs where we, so to speak, move to another stage of being. This particular stage of being is characterized by the fact that the player as subject is incorporated in the act of playing as the object of the act. Therefore, in the end play is not dependent on the subject who plays but of the subject submitting itself to something which involves the subject as if it was an object. Rephrased, it is “play that plays the player”, and we are thus attracted to play by a basic force. Gadamer describes this force as the fundamental “motion” of the universe as such ([3]:103–04). By submitting oneself to play, the player goes through a separation from ones status as a rational being and instead becomes a part of what Gadamer calls the “natural” uncertain and purposeless motion which influences the universe. This philosophical description in reality shows, in spite of the level of abstraction, a phenomenon which we are able to recognize as a common experience with play activities in which we experience that the play takes over when we actively engage in it – and however possesses the necessary skills. We forget about time and place when in play.
Though society has often viewed play as a childish and frivolous activity, we all engage in play over our entire lifespan, and engage in such play activities in which we forget about time and place just for the enjoyment and pleasure of play itself. Sport, sex, games, art, and scientific research activities can in many cases be described as playful activities in which the subject performs an ontological shift forgetting about time and place, and in which the activity has its own course and meaning. The play activity provides life fulfilling enjoyment and meaning to the player. The player can be of all ages. It appears limiting and exclusive to define such life fulfilling enjoyment as an activity for children and youth alone. Play is, for everybody, a fundamental activity submitted to free will. In the act of playing, we manage our lives at our own choice, as we create the special form of lived life outside the “regular” life where (lust for) life and happiness as the essence of play rules. When we play we become, in the words of the philosopher Friedrich Schiller, “a whole and complete human being”:
-
For, to speak out once for all, man only plays when in the full meaning of the word he is a man, and he is only completely a man when he plays. […] I promise you that the whole edifice of aesthetic art and the still more difficult art of life will be supported by this principle [4].
In the following, we will examine play amongst older adults. Especially, we will examine how the design and development of playful technology in the form of playware mediates playful interaction, and results in significant collateral effects of play in the health of the older adults.
2 Designing Play and Playware for Older Adults
We use countless methods to achieve the moods of play, and knowledge of those methods and competencies in using them are indispensable if one wants to play. As the American psychologist Michael J. Apter expresses it: One of the most interesting things about play is the tremendous variety of devices, stratagems and techniques which people can use to obtain the pleasures of play ([5], p. 18). And it could be added that it is similarly interesting which great economic investments people are willing to make to obtain playful experiences.
Some of the methods to achieve play we know, for example, as games, which we either learn, for instance from parents, peers etc., or buy as with computer games. Other methods are embedded in play equipment like the swing or the roller coaster. Both play equipment and games can be described as instruments or “tools” that are specialized in creating play, and when someone is using these tools, they assist in creating and regulating those physical and mental states of tension that we define as play.
If one wishes to design and develop play facilities or if one wishes to create play products, it is important to have an understanding of which games and play products will function and why some function and others do not. This understanding can be gained by studying what we call the play-dynamics which are activated through games and play-facilities. We define play-dynamics as follows, as we take our point of departure in concepts from the description of dynamic forces in the world of physics:
-
A play-dynamic is the dynamic effect of the play-force which affects the player by placing this person in a state of playing.
The play-force can for example be a motion, a competition, a danger or a joke which initiates a dynamic in which the player raise from the rational reality to a state of playing. The play-force is the influence and the effect becomes a dynamic play condition. Games and other tools function exactly by manifesting a force of play which can initiate a play-dynamic.
We can design play technology, called playware, which act as a play force bringing the user into a play-dynamic. Playware has been defined as intelligent hardware and software that creates play and playful experiences for users of all ages [6, 7]. Playware-tools are tools with a “behaviour” that initiates play force (e.g. a motion, in the case of sensorimotor play) via interaction. This is the basis for the play dynamic to emerge through which the users are brought into a state of playing. R&D in playware has led to numerous applications in various areas such as rehabilitation [8], playgrounds [7], education [9], art [10], and sport [11]. In all such cases, users interact with the playware as a free and voluntary activity that they engage in for the pleasure of play, even if the activity may be shown to have collateral effects e.g. in terms of health and skills. Modular playware has been proposed as of particular interest to develop solutions for such varied areas of application, since modularity may facilitate easy assembly and adaptation of the playware to different interaction modalities [12].
We can outline several guidelines for the design and development of modular playware [12], which should help in the designing playware that acts as a play force to bring the user into play dynamics. Important features of this design approach are modularity, flexibility, and construction, tangible interaction and immediate feedback to stimulate engagement, activity design by end-users, and creative exploration of play activities. These features permit the use of such modular playware by many users, including older adults who often could be prevented from using and taking benefits from modern technologies. The objective is to get anybody moving, exchanging, experimenting and having fun, regardless of their cognitive/physical ability levels.
3 Designing Modular Playware for Dementia Treatment
As an example of design of modular playware following these guidelines, together with P. Marti’s group at University of Siena, we designed and developed novel tools for dementia treatment based on activity analyses together with therapists and elderly in an Italian home care [13, 14]. We developed modular playware tools to become part of a “multi-sensory room”, i.e. a space augmented by innovative technologies, that can be configured for different therapeutic activities and needs and that provide sensory stimulation. The modular playware design features allow for space re-configurability and adaptivity, which should support customized therapeutic interventions, and involve dementia affected users in the interaction with the solutions. The objective of such environment is to obtain an optimal level of stimulation of dementia affected patients through their playful engagement, active participation and intrinsic motivation in the therapeutic activity, and favouring the emergence of personal meanings (memories, interpretations, narratives) eased by the dynamic configurations of the environment.
The modular playware we designed each has a physical expression (Light and Sound Cylinders and RollingPins). Each module can process and communicate with its surrounding environment (to neighbouring modules and/or through sensing or actuation). The overall behaviour emerges from the user’s coordination of a number of modules. The Light and Sound Cylinders and RollingPins developed for the non-pharmacological therapeutic treatment were designed as modular playware in order to allow very easy and understandable physical operation by dementia affected patients and therapists.
In particular, the RollingPins are semi-transparent plastic tubes capable of measuring their orientation and the speed of their rotation. They provide feedback in the form of RGB light, sound and vibration. The RollingPins are able to communicate with each other or with other devices equipped with the same radio communication technology. The RollingPins are usually used in pairs, as the local feedback of a RollingPin can be set depending not only on its own speed and orientation, but also on the speed and the orientation of the peer RollingPin. The system is used as a facilitator and mediator of social dynamics during the normal therapy to counteract social isolation that can result in dementia through the loss of social skills.
The RollingPins embody by design a dialogic component supporting non-verbal communication between therapist and patient. They can be manipulated (e.g. grasped, rolled and shaken), and each of these actions can produce feedback (visual, audio, tactile, smell as a local or environmental output in the multi-sensory room). The RollingPins communicate with each other, and by doing this they influence each other. Each time a RollingPin is manipulated, it produces an output (visual, auditory or tactile) both locally and remotely on the peer device, influencing its behaviour.
The therapeutic interventions in the multi-sensory room include the presence of a therapist. The therapist coordinates the session by defining the protocol, the setting, the most appropriate level of stimuli according to patients’ needs, and also supports the patient in remaining involved in the activity. In order to assess if non-verbal and gesture-based exchange can engage the dementia patient and sustain effective communication and coordination between therapist and patient, an experiment was designed to compare the use of the RollingPins in two conditions:
Individual Modality: with the RollingPins used as independent devices, interactive but not communicating with each other.
Dialogic Modality: with the RollingPins communicating with each other.
It was found in interventions with elderly dementia patients [13, 14] that using the RollingPins, the patients participated in the activity, coordinating their behaviour with the therapist and imitating the same interaction patterns generated by the therapist. Figure 1 shows physical engagement with the RollingPins in individual modality and dialogic modality, with statistical significant differences between the two modalities. Marti et al. [14] concluded that the use of simple units, easy to manipulate without explicit instruction, puts the subjects at ease and provides them with minimal but clear stimuli to both have a pleasurable experience and perform the tasks that better suit their problem. Furthermore, a dynamic, flexible and configurable system has proved to be a key factor for obtaining an optimal stimulation tailored to the specific needs of each patient.

The RollingPins used in individual modality and dialogic modality. The diagram shows mean values in seconds of behavioral indicators (None, Random, Tuning) of the dementia patients actions with the RollingPins in dialogical and individual modality tests.
Further, regarding the intervention with dementia patients, it was concluded that “The results of the experiment demonstrate the positive effects of the use of the RollingPins on engagement, coordination and motivation in regards to therapy in the dialogic condition. In particular, we observed that, differently from the patients working in the individual modality, the patients working in the dialogic modality established with the therapist a non-verbal dialogue based on sensory-motor imitation of the pattern generated by the therapist” [14].
To test for the modular playware mediating play thereby triggering intrinsic motivation in the patients, at the end of the session, the patients were asked to answer a standard version of the Intrinsic Motivation Inventory (IMI). The means of the Interest/Enjoyment and Perceived Competence scores were found to be higher in the dialogic condition than in the individual one. The Interest/Enjoyment means difference was significant (t = 1.95, p = 0.041), which is a critical scale in assessing the emergence of the intrinsic motivation. This indicates that the modular playware designed as the RollingPins indeed mediates playful interaction, which the patients engage in for their own enjoyment.
4 Designing Modular Playware for Functional Ability Enhancement of Older Adults
As another example of the design of modular playware following the design guidelines, we designed and developed modular interactive tiles for enhancing functional abilities – in particular balancing skills – of older adults. There are many functional abilities which are of high importance for elderly to retain and possibly improve in order to perform activities of daily living and in order lower health risks, e.g. related to illness and falls. These functional abilities include mobility, agility, balancing, strength and endurance. Due to the importance of such functional abilities for the health and daily activities of people, a number of training methods are used to address the prevention of loss of these abilities and to address the rehabilitation of these abilities. We hypothesize that if the training methods and training equipment is designed in the form of modular playware for retention and rehabilitation of functional abilities of elderly, it may motivate elderly to perform training which after just few training sessions can provide significant effects on the broad range of functional abilities necessary for elderly health and for elderly to perform their daily activities.
In order to verify this hypothesis, effect studies of such collateral effects of play among elderly is needed. Therefore, we will outline the design of a modular playware technology aimed at improving functional abilities among elderly and related studies of effect of playful modular interactive tiles training amongst community-dwelling elderly.
4.1 Material - Modular Interactive Tiles
The modular interactive tiles [8] are a distributed system of electronic tiles which like building blocks can be attached to one another to form the overall system (Fig. 2). Each tile is self-sufficient of processing power (an ATmega1280) and each one has a battery that lasts approximately 30 h in use. This makes the usage of the tiles very flexible because the tiles do not need a computer, a computer monitor or external power source. When connected to one another to form a playfield, the modular tiles communicate to their neighbors through four infra-red (IR) transceivers located on the sides. One tile has an XBee radio communication chip, with which it can communicate to other devices that have an XBee chip, for example a game selector box (or a PC that has an USB XBee dongle connected).

The modular interactive tiles can be assembled in different configurations for different playful exercises and levels.
When playing on the tiles, the subject provides the tiles with an input in the form of pressure measured by a force sensitive resistor which is located in the center of each tile. The tile can then react by turning on 8 RGB LEDs which are mounted with equal spacing between each other in a circle inside the tile. In the present intervention, the tiles were placed on the floor (though there is also an option to place them on a wall with magnets on the back of the tiles).
Therapists may use the interactive modular tiles to provide playful treatment for a large number of patients who receive hospital, municipality or home care, although the tiles can as well be used for prevention with elderly or for fitness with normal people. Nielsen and Lund [15] described the use of the modular tiles with cardiac patients, smoker’s lung (COLD) patients and stroke patients in hospitals and in the private homes of patients and elderly. Through a qualitative research methodology of the new practice with the tiles, it was found that therapists are using the modular aspect of the tiles for personalized training of a vast variety of elderly patients modulating exercises and difficulty levels, that in physical games there are individual differences in patient interaction capabilities and styles, and that modularity allows the therapist to adapt exercises to the individual patient’s capabilities [15]. The aspect of adaptivity was further explored by Lund and Thorsteinsson [16].
4.2 Interventions and Results
We have performed several tests for the effect on functional abilities of elderly from playful training with the modular interactive tiles over a short period of time, e.g. [17]. In one study, 16 community-dwelling elderly aged 63–95 years (mean 83.2 years of age) participated in 13 group training sessions on the modular interactive tiles over a period of 16 weeks in two senior activity centers in Gentofte (Copenhagen), Denmark. The training with the modular interactive tiles were set up to be an activity which like any other activities in the senior activity centers, the elderly could sign up to. Each individual elderly performed training on the modular interactive tiles 12–13 min during each session. The elderly participants were tested with the Senior Fitness Test [18, 19] (Chair-to-stand (CS), 8 ft Timed Up and Go (TUG), 6 Minute Walking Test (6MWT)) and an extra balancing test (Line Walk (LW)) before and after the intervention (pre-tests and post-tests after 13 sessions). The pre- and posttests were performed by Sundhedsdoktor, an independent third-party not involved with the training, and post-test was performed blinded from the pre-test results.
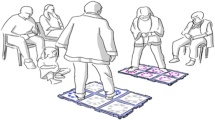
A research assistant would guide the training of the group on the modular interactive tiles, using 10–12 tiles for each session. In the group sessions, the elderly rotated between playing on the modular interactive tiles for a few minutes, and resting until it was their turn on the modular interactive tiles again.
During some of the sessions, the tiles would be split into two smaller platforms (with 6 tiles each) to allow parallel interaction of two elderly on two different platforms. Other part of the session would be on a larger platform of tiles, on which elderly would interact individually. The individual platforms where formed as squares of 9 tiles or as a horseshoe with the elderly player standing in the middle.
The games used for the training were Colour Race, Final Countdown, Reach, Island Game, Concentration Game Colour, and Simon Says. The last two games are memory games that may potentially challenge both physical and mental skills, whereas the first four games are also challenging mobility, balancing, endurance, and reaction. Indeed, most games are designed to challenge several physical and cognitive abilities simultaneously while playing the games.
The protocol for the sessions were that the elderly participants started out with playing Colour Race of 2 × 4 round with each round lasting for 30 s, given a two minute workout at a time followed by a break while the rest of the eldery were training. Afterwards, the game Final Countdown was applied in a slow version in order for the elderly participants to feel success with their playing. Again the training was 2 × 2 min, in a pace that the elders could set themselves. In the informal sessions, Reach, Island and Simon Says were used depending on the wishes and mood of the eldery while maintaining a two minute play, though Island has a fixed length of 1.5 min. The Concentration Game Color game was put on as a finale game, not least because this game seemed to entertain the eldery a lot, and thus motivated them to play for longer. In general each eldery got at least 12 min of training, but due to the nature of playing, some elders forgot time and in the informal sessions were allowed to continue to play games as Concentration Game Colour for longer time without breaks.
The sessions were preformed in small rooms with the tiles in the middle, surrounded by small mattress and the eldery placed on chairs along the edge. The setup had the advantage that the elders could engage with each other while playing, thus also motivate and making sure all participated.
The games required variations in the both movements of the players, such as the length of steps, moving forward and backwards, turning around, and in the speed, because of the elements of competition that is central for the games. These were important elements, due to the motivation of the elderly participants, as they lost track of time, and gave into playing the games.
Table 1 shows the results of the pre- and posttests of the elderly participants. All tests showed a statistical significant improvement of performance between pre-test and post-test at level P < 0.001 (Wilcoxon Signed Rank Test). The average improvement was 24 % on CS, 21 % on 8-ft TUG, 29 % on 6MWT, and 66 % on LW. Further, several subjects improved so that they transferred from one health risk level to another health risk level (according to the Rikli and Jones’ criterion reference points [19]) increasing at least one level. In total, 63 % of the subjects improved their health risk level according to at least one of the three tests of the Senior Fitness Test.
As confirmed by the quantitative data, also qualitative observations found the subjects to be much more mobile at post-test, and it was found that three subjects who performed the pre-tests with orthopedic aids (rollator, walker and cane), would perform the post-test without these aids or using these much less.
In another study, 12 community-dwelling elderly (average age: 79 (66–88)) with smaller balancing problems participated in a small randomized controlled study to test for dynamic balancing using the Dynamic Gait Index (DGI) test. The intervention was performed at the Lyngby-Taarbaek municipality (Copenhagen, Denmark) physiotherapy training unit. A therapist blinded to the intervention perform random lottery to assign the elderly to either the control group (6 persons) or the intervention group (6 persons). The control group continued to perform their daily activities during the experimental period of 2 months, whereas the intervention group performed playful training on the modular interactive tiles of average 12.5 group sessions during the 2 months. DGI tests were performed as pre-tests and post-tests for both control group and intervention group.
The test score for control group and intervention group is presented in Table 2. The score in the control group and the tiles training group did not differ at baseline (DGI mean score: 18.3 vs. 19.0), but there was significant difference in change of DGI score after the 2-months period with the control group decreasing DGI score by 9.3 % and tiles training group increasing DGI score by 12.3 %. A two way repeated measures ANOVA (Student Newman-Keuls method) resulted in no statistical significant differences at baseline and in control group performance over time, whereas there is statistical significant increase in performance of tiles training group over time (p < 0.05) and statistical significant difference between control group and tiles training group after intervention (p < 0.05). DGI mean score after intervention was 16.6 for the control group compared with 21.33 for the tiles training group, i.e. −9.3 % vs. +12.3 %.
The community dwelling elderly with balancing problems seemed to be at high risk of falling if not subject to any training, whereas those who performed training increased their dynamic balancing abilities. A DGI score of < 19 is associated with impairment of gait and fall risk [20, 21], so the statistical significant difference between DGI score of 16.6 of the control group and DGI score of 21.33 of the tiles training group is important.
5 Discussion and Conclusion
The effect studies show important collateral effects of play. Qualitative observations indicate that the elderly participants are having fun and that they meet to play for their own enjoyment and pleasure. They enter into play as a free and voluntary activity with no other purpose that the play itself, and for the life fulfilling enjoyment and meaning that it provides to the elderly participants. The observations indicate that the ontological shift happens for the participants. They enter into a new status when they are playing, forgetting about time and place, and thereby most importantly for obtaining the documented collateral health effects of play, they forget about the fear of falling, fear of getting out of balance, their normal physical limitations, etc. We observe that often, when the elderly citizens are on the modular interactive tiles, they jump around much more freely and fast than when they move around normally.
Hence, the tiles’ light pattern and performance seem to act as a play force which pushes the elderly user into a play dynamics. The tiles light up in the pattern needed to be performed by the user, and the tiles are providing immediate feedback to the user. As found by Nielsen and Lund in a study of playful training on tiles with elderly stroke patients: “the features of the modular interactive tiles allow for a combination of physical and cognitive training of elderly” [15]. The features based upon the modular playware design seem to be among those which results in the tiles acting as a play force. They distinguish the modular interactive tiles from other exergaming systems and other training methods, and may be among the reasons that may explain the success of the modular interactive tiles for improving the functional abilities of the community-dwelling elderly.
Compared with other training methods, it is extraordinary that the playful training on modular interactive tiles show statistical significant effects on all the test measures of elderly functional abilities after merely 13 group training sessions during which each elderly exercise for just 12–13 min. Hence, the statistical significant effects are obtained after just 2–3 h of total training time on the modular interactive tiles. This can be compared to other training methods and interventions typically reporting 13–25 h of training for showing statistical significant effects [22].
Further, even when such other training methods show statistical significant effects after the longer period of, for instance, 25 training sessions, the effects are often on only one or two of the functional abilities that are included in the tests in the present work. Contrary, the tests with modular interactive tiles training show comprehensive statistical significant effect on all test measures which test for dynamic balancing, strength, mobility, agility, and endurance.
The design, development and testing of modular playware (e.g. as RollingPins and modular interactive tiles) has shown that such tools may act as play forces to push the users into play dynamics. The users engage in play with such playware as a free and voluntary activity with no other purpose than play itself, but simply for the pleasure and enjoyment. For instance, in the case of the modular interactive tiles, it seems to be the case that the elderly participants forget about their possible fear of falling and physical limitations when playing, and thereby achieve the remarkable collateral effect on their health in terms of balancing skills, endurance, strength, etc. Hence, as has been shown in this paper, playing may lead to important collateral effects. These collateral effects of play are shown to be significant and important, especially in the area of health. At the same time, it is important to remember that play is a self-sustaining phenomenon which carries its purpose in itself.
References
Huizinga, J.: Homo Ludens (1938). Beacon Press, Boston (1971)
Caillois, R.: Man, Play and Games (1958). University of Illinois Press, Champaign (2001)
Gadamer, H.-G.: Truth and Method. Crossroad, New York (1989)
Schiller, F.: Letters Upon The Aesthetic Education of Man. Courier Corporation, Chelmsford (1795)
Apter, M.J.: A structural phenomenology of play. In: Kerr, J.K., Apter, M.J. (eds.) Adult Play. Routledge, New York (1991)
Lund, H.H., Jessen, C.: Playware - Intelligent technology for children’s play. Technical report TR-2005-1, June, Maersk Institute, University of Southern Denmark (2005)
Lund, H.H., Klitbo, T., Jessen, C.: Playware technology for physically activating play. Artif. Life Robot. J. 9(4), 165–174 (2005)
Lund, H.H.: Modular robotics for playful physiotherapy. In: Proceedings of IEEE International Conference on Rehabilitation Robotics, pp. 571–575. IEEE Press (2009)
Lund, H.H., Marti, P.: Physical and conceptual constructions in advanced learning environments. Interact. Stud. 5(2), 269–299 (2004)
Lund, H.H., Ottesen, M.: RoboMusic – a behavior-based approach. Artif. Life Robot. J. 12(1–2), 18–23 (2008)
Lund, H.H., Thorsteinsson, T.: Social playware for mediating teleplay interaction over distance. Int. J. Artif. Life Robot. 16(4), 435–440 (2012)
Lund, H.H., Marti, P.: Designing modular robotic playware. In: Proceedings of 18th IEEE International Symposium on Robot and Human Interactive Communication (Ro-Man 2009), pp.115–121. IEEE Press (2009)
Marti, P., Lund, H.H., Bacigalupo, M., Giusti, L., Mennecozzi, C.: A multi-sensory environment for the treatment of dementia affected subjects. J. Gerontechnol. 6(1), 33–41 (2007)
Marti, P., Giusti, L., Lund, H.H.: The role of modular robotics in mediating nonverbal social exchanges. IEEE Trans. Rob. 25(3), 602–613 (2009)
Nielsen, C.B., Lund, H.H.: Adapting playware to rehabilitation practices. Int. J. Comput. Sci. Sport 11, 1 (2012)
Lund, H.H., Thorsteinsson, T.: Adaptive playware in physical games. In: Proceedings of the 6th International Conference on Foundations of Digital Games 2011. ACM (2011)
Lund, H.H., Jessen, J.D.: Effects of short-term training of community-dwelling elderly with modular interactive tiles. Games For Health: Res. Dev. Clin. Appl. 3(5), 277–283 (2014)
Rikli, R.E., Jones, C.J.: Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Act. 7(2), 129–161 (1999)
Rikli, R.E., Jones, C.J.: Senior Fitness Test Manual. Human Kinetics, Champaign (2001)
Shumway-Cook, A., Woollacott, M.: Motor Control: Theory and Applications. Wilkins & Wilkins, Baltimore (1995)
Shumway-Cook, A., Baldwin, M., Polissar, N.L., Gruber, W.: Predicting the probability for falls in community-dwelling older adults. Phys. Ther. 77, 812–819 (1997)
Sherrington, C., Whitney, J.C., Lord, S.R., Herbert, R.D., Cumming, R.G., Close, J.C.T.: Effective exercise for the prevention of falls: a systematic review and meta-analysis. J. Am. Geriatr. Soc. 56(12), 2234–2243 (2008)
Acknowledgement
The author would like to thank Prof.ssa Patrizia Marti, University of Siena and her group, staff and elderly at Casa Protetta Albesani, staff and elderly at the senior activity centers Tvaerbommen and Vennerslund, children from the kindergarten, Sundhedsdoktor, Gentofte municipality, Lyngby-Taarbaek municipality, physiotherapists of Lyngby-Taarbaek municipality, Kirsten Skyhøj, volunteers from Ældre Sagen in Lyngby, and especially J. Jessen who assisted several interventions.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer International Publishing Switzerland
About this paper
Cite this paper
Lund, H.H. (2015). Play for the Elderly - Effect Studies of Playful Technology. In: Zhou, J., Salvendy, G. (eds) Human Aspects of IT for the Aged Population. Design for Everyday Life. ITAP 2015. Lecture Notes in Computer Science(), vol 9194. Springer, Cham. https://doi.org/10.1007/978-3-319-20913-5_46
Download citation
DOI: https://doi.org/10.1007/978-3-319-20913-5_46
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-319-20912-8
Online ISBN: 978-3-319-20913-5
eBook Packages: Computer ScienceComputer Science (R0)