
Abstract
Background
The influence of distance traveled for treatment on short- and long-term cancer outcomes is unclear.
Methods
Patients with colon, esophageal, liver, and pancreas cancer from 2003 to 2006 were identified from the National Cancer Data Base (NCDB). Distance traveled for surgical treatment was estimated using zip code centroids. Propensity scores were generated for probability of traveling farther for treatment. Mixed effects logistic regression for 90-day mortality and Cox regression for 5-year mortality were compared between patients treated regionally and those traveling from farther away.
Results
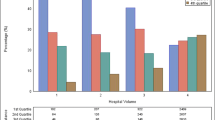
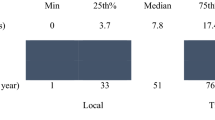
The mean distance traveled for all patients for surgical resection was 30.0 ± 227 miles, with a median distance of 7.5 (interquartile range 14.4) miles. Patients who were aged ≥80 years, on Medicaid, or African American were less likely to be in the fourth quartile of distance (Q4) traveled for surgery. Patients who were in Q4 had a lower risk-adjusted 90-day mortality compared to Q1 for colon [odds ratio (OR) 0.89, 95 % confidence interval (CI) 0.82–0.96], liver (OR 0.49, 95 % CI 0.3–0.78), and pancreatic (OR 0.74, 95 % CI 0.56–0.98) cancer. Similarly, patients in Q4 for all tumor types had a lower risk-adjusted 5-year mortality compared to patients in Q1; colon (hazard ratio (HR) 0.96, 95 % CI 0.93–0.99), esophagus (HR 0.84, 95 % CI 0.75–0.94), liver (HR 0.75, 95 % CI 0.62–0.89), and pancreas (HR 0.87, 95 % CI 0.80–0.95).
Conclusions
Greater travel distance for surgical resection of gastrointestinal cancers is associated with lower 90-day and 5-year mortality outcomes. This distance bias has implications for regionalization and reporting of cancer outcomes.

Similar content being viewed by others

References
Ballard DJ, Bryant SC, O’Brien PC, et al. Referral selection bias in the Medicare hospital mortality prediction model: are centers of referral for Medicare beneficiaries necessarily centers of excellence?. Health Serv Res. 1994;28:771–84.
Etzioni DA, Fowl RJ, Wasif N, et al. Distance bias and surgical outcomes. Med Care. 2013;51:238–44.
Lamont EB, Hayreh D, Pickett KE, et al. Is patient travel distance associated with survival on phase II clinical trials in oncology?. J Natl Cancer Inst. 2003;95:1370–5.
Lenhard RE Jr, Enterline JP, Crowley J, et al. The effects of distance from primary treatment centers on survival among patients with multiple myeloma. J Clin Oncol. 1987;5:1640–5.
Swanson RS, Pezzi CM, Mallin K, et al. The 90-day mortality after pancreatectomy for cancer is double the 30-day mortality: more than 20,000 resections from the National Cancer Data Base. Ann Surg Oncol. 2014;21:4059–67.
Byrne BE, Mamidanna R, Vincent CA, et al. Population-based cohort study comparing 30- and 90-day institutional mortality rates after colorectal surgery. Br J Surg. 2013;100:1810–7.
Onega T, Duell EJ, Shi X, et al. Geographic access to cancer care in the US. Cancer. 2008;112:909–18.
Charlson M, Szatrowski TP, Peterson J, et al. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47:1245–51.
Dehejia RH. Propensity score-matching methods for nonexperimental causal studies. Rev Econ Stat. 2002;84:151–61.
Imbens G. The role of the propensity score in estimating dose–response functions. Biometrika. 2000;87:706–10.
Etzioni DA, Wasif N, Dueck AC, et al. Association of hospital participation in a surgical outcomes monitoring program with inpatient complications and mortality. JAMA. 2015;313:505–11.
Patlak M, Nass SJ. The role of obesity in cancer survival and recurrence: workshop summary. Washington, DC: National Academies Press; 2012.
Esnaola NF, Ford ME. Racial differences and disparities in cancer care and outcomes: where’s the rub? Surg Oncol Clin North Am. 2012;21:417–37.
Fortney J RK, Warren J. Comparing alternative methods of measuring geographic access to health services. Health Serv Outcomes Res Methodol. 2000;1:173–84.
Acknowledgment
The data used in this study are derived from a deidentified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed or for the conclusions drawn from these data by the investigators.
Disclosure
No financial disclosures or conflicts of interest for any of the authors and no specific source of funding.
Author information
Authors and Affiliations
Corresponding author
Additional information
The data used in this study are derived from a de-identified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigators.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Wasif, N., Chang, YH., Pockaj, B.A. et al. Association of Distance Traveled for Surgery with Short- and Long-Term Cancer Outcomes. Ann Surg Oncol 23, 3444–3452 (2016). https://doi.org/10.1245/s10434-016-5242-z
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-016-5242-z