
Abstract
Background
Previous reports on the surgical management of appendix cancer show high recurrence rates among patients initially presenting with localized disease. This study sought to characterize predictors of outcome among patients treated for stages 1–3 appendix cancer at the authors’ institution.
Methods
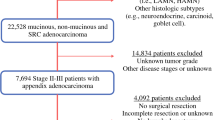
Patients with nonmetastatic appendix cancer undergoing definitive surgery at a single cancer center from 1994 to 2013 were retrospectively reviewed. Patients with appendiceal adenomas, cystadenomas, or classical carcinoids were excluded from the study. The median follow-up period was 5.2 years (interquartile range 2.9–6.7 years).
Results
The study identified 70 patients, 49 % of whom were women. The median age was 52 years (range 20–84 years). All were explored by an expert surgeon who had treated at least 20 appendiceal cancers. The procedures were appendectomy (n = 2), right hemicolectomy (n = 66), and diagnostic laparoscopy and placement of an intraperitoneal port (n = 2). The final pathology showed that transmural (30 T4, 32 T3, 4 T2, 4 T1) and node-negative disease (80 %) were common. Goblet cell carcinoid (GCC) features were identified in 54 % of the tumors. These were smaller and more likely to present as acute appendicitis than appendiceal adenocarcinoma (AA), but were otherwise similar in clinical presentation and outcome. The presence of lymph node (LN) metastasis was associated with a higher risk of recurrence than of stage 2 appendix cancer (78 vs. 4 % at 5 years; p < 0.0001). A total of 12 patients experienced recurrence (5 GCC, 7 AA): 9 in the peritoneum, 2 in mesenteric LNs, and 1 in the surgical incision.
Conclusion
Stages 1–3 invasive AA and GCC behave similarly in terms of clinical presentation and outcome. Perforated appendix and T4 tumor stage were common but not associated with recurrence. Although uncommon, LN metastasis strongly predicted recurrence.

Similar content being viewed by others


References
Nitecki SS, Wolff BG, Schlinkert R, Sarr MG. The natural history of surgically treated primary adenocarcinoma of the appendix. Ann Surg. 1994;219:51–7.
Proulx GM, Willett CG, Daley W, Shellito PC. Appendiceal carcinoma: patterns of failure following surgery and implications for adjuvant therapy. J Surg Oncol. 1997;66:51–3.
Benedix F, Reimer A, Gastinger I, Mroczkowski P, Lippert H, Kube R; Study Group Colon/Rectum Carcinoma Primary Tumor. Primary appendiceal carcinoma-epidemiology, surgery and survival: results of a German multi-center study. Eur J Surg Oncol. 2010;36:763–1.
McGory ML, Maggard MA, Kang H, O’Connell JB, Ko CY. Malignancies of the appendix: beyond case series reports. Dis Colon Rectum. 2005;48:2264–71.
Connor SJ, Hanna GB, Frizelle FA. Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum. 1998;41:75–80.
O’Donnell ME, Badger SA, Beattie GC, Carson J, Garstin WI. Malignant neoplasms of the appendix. Int J Colorectal Dis. 2007;22:1239–48.
Tang LH, Shia J, Soslow RA, et al, Pathologic classification and clinical behavior of the spectrum of goblet cell carcinoid tumors of the appendix. Am J Surg Pathol. 2008;32:1429–43.
Sugarbaker PH. The natural history, gross pathology, and histopathology of appendiceal epithelial neoplasms. Eur J Surg Oncol. 2006;32:644–7.
Acknowledgment
This study was funded in part by the cancer center Core Grant P30 CA008748. The Core Grant provides funding to institutional cores such as biostatistics and pathology, which were used in this study.
Disclosure
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nash, G.M., Smith, J.D., Tang, L. et al. Lymph Node Metastasis Predicts Disease Recurrence in a Single-Center Experience of 70 Stages 1–3 Appendix Cancers: A Retrospective Review. Ann Surg Oncol 22, 3613–3617 (2015). https://doi.org/10.1245/s10434-015-4415-5
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4415-5