
Abstract
Background
The clinical significance of synchronous bilateral papillary thyroid carcinoma (SBiPTC) has not been fully defined, and the prevalence of BRAF V600E mutation in SBiPTC remains unknown. The purpose of this study is to compare the clinical outcomes and BRAF V600E mutation incidence of SBiPTC patients with those of unilateral papillary thyroid carcinoma (UiPTC) patients.
Methods
From 1997 to 2008, a total of 903 patients with papillary thyroid cancer were treated at a single institution. Of 891 studied patients, 177 (19.9%) had SBiPTC and 714 had UiPTC. SBiPTC was defined as cancer diagnosed in both thyroid lobes at the same time or within a period of 3 months. The mean follow-up time was 6 years, ranging from 2.5 to 13.5 years. Rates of disease-free survival (DFS) and overall survival (OS) were calculated and compared. BRAF V600E mutation was determined by polymerase chain reaction (PCR) amplification and DNA sequencing.
Results
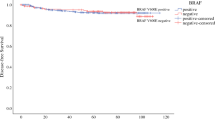
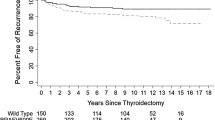
Compared with UiPTC patients, patients with SBiPTC were more likely to have larger tumor size, extrathyroidal invasion, lymph node metastasis, and more advanced stage. The 5-year DFS rate was 86.0% for SBiPTC patients and 94.0% for UiPTC patients (p = 0.013). The prevalence of BRAF V600E mutation in the SBiPTC group was significantly higher than that in the UiPTC group (65.7% vs. 50.4%; p = 0.038).
Conclusions
Patients with SBiPTC present with more advanced tumor stage and have shorter disease-free survival than UiPTC patients. Poorer outcomes of these patients may be at least partially explained by the high incidence of BRAF V600E mutation.


Similar content being viewed by others

References
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300.
Franceschi S, Boyle P, Maisonneuve P, La Vecchia C, Burt AD, Kerr DJ, et al. The epidemiology of thyroid carcinoma. Crit Rev Oncog. 1993;4:25–52.
Elisei R, Molinaro E, Agate L, et al. Are the clinical and pathological features of differentiated thyroid carcinoma really changed over the last 35 years? Study on 4187 patients from a single Italian institution to answer this question. J Clin Endocrinol Metab. 2010;95:1516–27.
Wang W, Wang H, Teng X, et al. Clonal analysis of bilateral, recurrent, and metastatic papillary thyroid carcinomas. Hum Pathol. 2010;41:1299–309.
Elisei R, Ugolini C, Viola D, et al. BRAF (V600E) mutation and outcome of patients with papillary thyroid carcinoma: a 15-year median follow-up study. J Clin Endocrinol Metab. 2008;93:3943–9.
Oler G, Cerutti JM. High prevalence of BRAF mutation in a Brazilian cohort of patients with sporadic papillary thyroid carcinomas: correlation with more aggressive phenotype and decreased expression of iodide-metabolizing genes. Cancer. 2009;115:972–80.
Greene FL, Page DL, Fleming ID, et al. (editors) American Joint Committee on Cancer 2002 AJCC cancer staging manual. 6th ed. New York, Berlin, Heidelberg: Springer-Verlag; 2002.
Carta C, Moretti S, Passeri L, et al. Genotyping of an Italian papillary thyroid carcinoma cohort revealed high prevalence of BRAF mutations, absence of RAS mutations and allowed the detection of a new mutation of BRAF oncoprotein (BRAF(V599lns)). Clin Endocrinol (Oxf). 2006;64:105–9.
Pasieka JL, Thompson NW, McLeod MK, Burney RE, Macha M. The incidence of bilateral well-differentiated thyroid cancer found at completion thyroidectomy. World J Surg. 1992;16: 711–6.
Katoh R, Sasaki J, Kurihara H, Suzuki K, Iida Y, Kawaoi A. Multiple thyroid involvement (intraglandular metastasis) in papillary thyroid carcinoma. A clinicopathologic study of 105 consecutive patients. Cancer. 1992;70:1585–90.
Lin JD, Chao TC, Hsueh C, Kuo SF. High recurrent rate of multicentric papillary thyroid carcinoma. Ann Surg Oncol. 2009;16:2609–16.
Lin YK, Sheng JM, Zhao WH, Wang WB, Yu XF, Teng LS, et al. Multifocal papillary thyroid carcinoma: clinical analysis of 168 cases. Zhonghua Wai Ke Za Zhi. 2009;47:450–3.
Cushing SL, Palme CE, Audet N, Eski S, Walfish PG, Freeman JL. Prognostic factors in well-differentiated thyroid carcinoma. Laryngoscope. 2004;114:2110–5.
Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA. High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res. 2003;63:1454–7.
Nikiforova MN, Kimura ET, Gandhi M, et al. BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J Clin Endocrinol Metab. 2003;88:5399–404.
Xing M. BRAF mutation in papillary thyroid cancer: pathogenic role, molecular bases, and clinical implications. Endocr Rev. 2007;28:742–62.
Xing M. BRAF mutation in thyroid cancer. Endocr Relat Cancer. 2005;12:245–62.
McCarthy RP, Wang M, Jones TD, Strate RW, Cheng L. Molecular evidence for the same clonal origin of multifocal papillary thyroid carcinomas. Clin Cancer Res. 2006;12:2414–8.
Jovanovic L, Delahunt B, McIver B, Eberhardt NL, Grebe SK. Most multifocal papillary thyroid carcinomas acquire genetic and morphotype diversity through subclonal evolution following the intra-glandular spread of the initial neoplastic clone. J Pathol. 2008;215:145–54.
Shattuck TM, Westra WH, Ladenson PW, Arnold A. Independent clonal origins of distinct tumor foci in multifocal papillary thyroid carcinoma. N Engl J Med. 2005;352:2406–12.
Giannini R, Ugolini C, Lupi C, et al. The heterogeneous distribution of BRAF mutation supports the independent clonal origin of distinct tumor foci in multifocal papillary thyroid carcinoma. J Clin Endocrinol Metab. 2007;92:3511–6.
Park SY, Park YJ, Lee YJ, et al. Analysis of differential BRAF(V600E) mutational status in multifocal papillary thyroid carcinoma: evidence of independent clonal origin in distinct tumor foci. Cancer. 2006;107:1831–8.
Passler C, Scheuba C, Asari R, Kaczirek K, Kaserer K, Niederle B. Importance of tumour size in papillary and follicular thyroid cancer. Br J Surg. 2005;92:184–9.
Shaha A. Selective surgical management of well-differentiated thyroid cancer. Ann N Y Acad Sci. 2008;1138:58–64.
Haigh PI, Urbach DR, Rotstein LE. Extent of thyroidectomy is not a major determinant of survival in low- or high-risk papillary thyroid cancer. Ann Surg Oncol. 2005;12:81–9.
Ito Y, Uruno T, Nakano K, et al. An observation trial without surgical treatment in patients with papillary microcarcinoma of the thyroid. Thyroid. 2003;13:381–7.
Acknowledgment
This study was supported by National Basic Research Program of China (973 Program, no. 2009CB521704). We thank Peng Lu and Yaqi Jiang for patients’ clinical follow-up, and Fei Teng (Division of Engineering Science, University of Toronto, Toronto, Canada) for technical assistance. We are also grateful to Dr. Robert Wohlhueter (Centers for Disease Control and Prevention, Atlanta, GA; retired) for his contributions to the preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, W., Zhao, W., Wang, H. et al. Poorer Prognosis and Higher Prevalence of BRAF V600E Mutation in Synchronous Bilateral Papillary Thyroid Carcinoma. Ann Surg Oncol 19, 31–36 (2012). https://doi.org/10.1245/s10434-011-2096-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-011-2096-2