
Abstract
Introduction
Patients with unilateral breast cancer have an increased risk of developing contralateral breast cancer. A recent population-based study demonstrated that the proportion of patients with unilateral breast cancer in the United States who underwent contralateral prophylactic mastectomy (CPM) has increased by 150% in recent years. The current study evaluated patients who underwent breast cancer surgery in a metropolitan-based hospital system to determine factors associated with CPM.
Methods
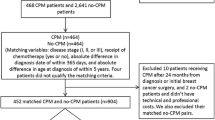
We reviewed the records of all patients who underwent surgical treatment for breast cancer in 2006 and 2007 in a single health care system, which included six different hospitals. Exclusion criteria included preoperative diagnosis of bilateral disease, stage IV disease, and a history of previous breast cancer. We recorded patient, treatment, tumor, and surgeon characteristics. Multivariate logistic regression models were used to predict CPM use.
Results
Of 571 eligible patients, 276 (48.3%) underwent breast-conserving surgery (BCS), 130 (22.8%) underwent unilateral mastectomy, and 165 (28.9%) underwent mastectomy and a CPM. Among mastectomy patients, 55.9% underwent CPM. Young age (<40 vs. >55 years), large tumor size (>5 vs. <2 cm), positive family history, lobular histology, multicentric disease, and surgeon gender (female) were independent predictors of increased CPM rates. Body mass index, tumor grade, estrogen receptor status, and preoperative breast magnetic resonance imaging were not associated with increased CPM rates.
Conclusions
Our study is the first to evaluate specific surgeon characteristics associated with CPM use. Prospective studies are needed to examine factors affecting patient decision-making to develop resources that may assist patients in this process.
Similar content being viewed by others

References
Hislop TG, Elwood JM, Coldman AJ, Spinelli JJ, Worth AJ, Ellison LG. Second primary cancers of the breast; incidence and risk factors. Br J Cancer. 1984;49:79–85.
Kollias J, Ellis IO, Elston CW, Blamey RW. Clinical and histological predictors of contralateral breast cancer. Eur J Surg Oncol. 1999;25:584–9.
Saphner T, Tormey DC, Gray R. Annual hazard rates of recurrence for breast cancer after primary therapy. J Clin Oncol. 1996;14:2738–46.
Rosen PP, Groshen S, Kinne DW, Hellman S. Contralateral breast carcinoma: an assessment of risk and prognosis in stage I (T1N0M0) and stage II (T1N1M0) patients with 20-year follow-up. Surgery. 1989;106:904–10.
Healey EA, Cook EF, Orav EJ, Schnitt SJ, Connolly JL, Harris JR. Contralateral breast cancer: clinical characteristics and impact on prognosis. J Clin Oncol. 1993;11:1545–52.
Lostumbo L, Carbine N, Wallace J, Ezzo J. Prophylactic mastectomy for the prevention of breast cancer. Cochrane Database Syst Rev. 2004;18(4):CD002748. Review.
McDonnell SK, Schaid DJ, Myers JL, et al. Efficacy of contralateral prophylactic mastectomy in patients with a personal and family history of breast cancer. J Clin Oncol. 2001;19:3938–43.
Peralta EA, Ellenhorn JD, Wagman LD, Dagis A, Andersen JS, Chu DZ. Contralateral prophylactic mastectomy improves the outcome of selected patients undergoing mastectomy for breast cancer. Am J Surg. 2000;180:439–45.
van Sprundel TC, Schmidt MK, Rookus MA, et al. Risk reduction of contralateral breast cancer and survival after contralateral prophylactic mastectomy in BRCA1 or BRCA2 mutation carriers. Br J Cancer 2005;93:287–92.
Herrinton LJ, Barlow WE, Yu O, et al. Efficacy of prophylactic mastectomy in patients with unilateral breast cancer: a cancer research network project. J Clin Oncol. 2005;23:4275–86.
Barton MB, West CN, Liu IL, et al. Complications following bilateral prophylactic mastectomy. J Natl Cancer Inst Monogr. 2005;35:61–6.
Tuttle TM, Habermann EB, Grund EH, Morris TJ, Virnig BA. Increasing use of contralateral prophylactic mastectomy for breast cancer patients: a trend toward more aggressive surgical treatment. J Clin Oncol. 2007;25:5203–9.
Tuttle TM, Jarosek S, Habermann EB, Arrington A, Abraham A, Morris TJ, Virnig BA. Increasing rates of contralateral prophylactic mastectomy among patients with ductal carcinoma in situ. J Clin Oncol. 2009;27:1362–7.
NIH Consensus Conference. Treatment of early stage breast cancer. JAMA. 1991;265:391–5.
Katipamula R, Hoskin TL, Boughey JC, et al. Trends in mastectomy rates at the Mayo Clinic Rochester: effect of surgical year and preoperative MRI. J Clin Oncol. 2008;26(Suppl 15S):509.
Sorbero ME, Dick AW, Beckjord EB, Ahrendt G. Diagnostic breast magnetic resonance imaging and contralateral prophylactic mastectomy. Ann Surg Oncol. 2009;16:1597–605.
Metcalfe K, Lynch HT, Ghadirian P et al. Contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2004;22:2328–35.
Schrag D, Kuntz KM, Garber JE, Weeks JC. Life expectancy gains from cancer prevention strategies for patients with breast cancer and BRCA1 or BRCA2 mutations. JAMA. 2000;283:617–24.
Fisher B, Dignam J, Wolmark N, et al. Tamoxifen in treatment of intraductal breast cancer: National Surgical Adjuvant Breast and Bowel Project B-24 randomised controlled trial. Lancet. 1999;353:1993–2000.
Chagpar AB, Studts JL, Scoggins CR, et al. Factors associated with surgical options for breast carcinoma. Cancer. 2006;106:1462–6.
Montgomery LL, Tran KN, Heelan MC, Van Zee KJ, Massie MJ, Payne DK, Borgen PI. Issues of regret in patients with contralateral prophylactic mastectomies. Ann Surg Oncol. 1999;6:546–52.
Nekhlyudov L, Bower M, Herrinton LJ, et al. Patients’ decision-making roles regarding contralateral prophylactic mastectomy. J Natl Cancer Inst Monogr. 2005;35:55–60.
Silliman RA, Demissie S, Troyan SL. The care of older patients with early-stage breast cancer: what is the role of surgeon gender? Med Care. 1999;37:1057–67.
Weinberg E, Wood S, Grannen K. The influence of gender of the surgeon on surgical procedure preference for breast cancer. Am Surg. 2002;68:398–400.
Hershman DL, Buono D, Jacobson JS, McBride RB, Tsai WY, Joseph KA, Neugut AI. Surgeon characteristics and use of breast conservation surgery in women with early stage breast cancer. Ann Surg. 2009;249:828–33.
Goldflam K, Hunt KK, Gershenwald JE, et al. Contralateral prophylactic mastectomy. Predictors of significant histologic findings. Cancer. 2004;101:1977–86.
Fisher B, Redmond C. New perspective on cancer of the contralateral breast: a marker for assessing tamoxifen as a preventive agent. J Natl Cancer Inst. 1991;83:1278–80.
Stewart HJ for the Scottish Cancer Trials Breast Group. The Scottish trial of adjuvant tamoxifen in node-negative breast cancer. J Natl Cancer Inst Monogr. 1992;11:117–20.
Rutvist LE, Cedermark B, Glas U, et al. Contralateral primary tumors in breast cancer patients in a randomized trial of adjuvant tamoxifen therapy. J Natl Cancer Inst. 1991;83:1299–306.
Baum M, Budzar AU, Cuzick J, Forbes J, Houghton JH, Klijn JG, Sahmoud T; ATAC Trialists’ Group. Anastrozole alone or in combination with tamoxifen versus tamoxifen alone for adjuvant treatment of post-menopausal patients with early breast cancer: First results of the ATAC randomised trial. Lancet. 2002;359:2131–9.
Meakin JW, Hayward JL, Panzarella T, et al. Ovarian radiation and prednisone following surgery and radiotherapy for carcinoma of the breast. Breast Cancer Res Treat. 1996;37:11–9.
Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breast cancer: an overview of the randomised trials. Lancet. 1998;351:1451–67.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Arrington, A.K., Jarosek, S.L., Virnig, B.A. et al. Patient and Surgeon Characteristics Associated with Increased Use of Contralateral Prophylactic Mastectomy in Patients with Breast Cancer. Ann Surg Oncol 16, 2697–2704 (2009). https://doi.org/10.1245/s10434-009-0641-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-009-0641-z