
Abstract
Background
The aim of this study was to compare conventional open thyroidectomy with robotic thyroidectomy in terms of postoperative pain.
Methods
We compared the intensity of postoperative pain experienced by patients who received conventional open thyroidectomy (n = 45) versus those who underwent robotic thyroidectomy (n = 45). During surgery, we carefully controlled the anesthetic conditions. All the patients underwent a total thyroidectomy with ipsilateral central compartment node dissection. Postoperative pain in the 2 groups was compared using a visual analog scale and the amount of rescue analgesic at 30 min, 4 h, 1, 2, 3, and 10 days after surgery.
Results
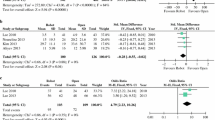
The postoperative pain at 30 min and 4 h after surgery were 3.0 ± 0.9 and 2.6 ± 0.9 (p = .066) and 4.9 ± 1.3 and 4.4 ± 1.3 (p = .055) in the conventional open group and the robotic group, respectively. The mean pain scores at 1, 2, 3, and 10 days after surgery were 3.8 ± 1.3 and 3.0 ± 1.3 (p = .001), 2.6 ± 1.2 and 2.0 ± 0.9 (p = .005), 1.7 ± 0.9 and 1.3 ± 0.6 (p = .034), and 0.9 ± 0.7 and 1.2 ± 1.1 (p = .093), respectively. No significant differences were observed between the 2 groups in terms of postoperative rescue analgesic use (1.1 ± 1.1 and 0.8 ± 0.9, p = .264).
Conclusions
Even though robotic thyroidectomy using the transaxillary technique requires a more extensive subcutaneous dissection than conventional open thyroidectomy, robotic thyroidectomy does not result in more postoperative pain or use of analgesic when compared with open thyroidectomy.


Similar content being viewed by others


Reference
Ganger M. Endoscopic subtotal parathyroidectomy in patients with primary hyperparathyroidism. Br J Surg. 1996;83:875.
Hüscher CS, Chiodini S, Napolitano C, Recher A. Endoscopic right thyroid lobectomy. Surg Endosc. 1997;11:877.
Palazzo FF, Sebag F, Henry JF. Endocrine surgical technique: endoscopic thyroidectomy via the lateral approach. Surg Endosc. 2006;20:339–42.
Chung YS, Choe JH, Kang KH, Kim SW, Chung KW, Park KS, et al. Endoscopic thyroidectomy for thyroid malignancies: comparison with conventional open thyroidectomy. World J Surg. 2007;31:2302–6.
Lee KE, Rao J, Youn YK. Endoscopic thyroidectomy with the da Vinci robot system using the bilateral axillary breast approach (BABA) technique: our initial experience. Surg Laparosc Endosc Percutan Tech. 2009;19:e71–e75.
Del Rio P, Sommaruga L, Cataldo S, Robuschi G, Arcuri MF, Sianesi M. Minimally invasive video-assisted thyroidectomy: the learning curve. Eur Surg Res. 2008;41:33–6.
Gozal Y, Shapira SC, Gozal D, Magora F. Bupivacaine wound infiltration in thyroid surgery reduces postoperative pain and opioid demand. Acta Anaesthesiol Scand. 1994;38:813–5.
Kang SW, Lee SC, Lee SH, Jeong JJ, Lee YS, Nam KH, et al. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: the operative outcomes of 338 consecutive patients. Surgery. 2009;146:1048–55.
Kang SW, Jeong JJ, Yun JS, Sung TY, Lee SC, Lee YS, et al. Robot-assisted endoscopic surgery for thyroid cancer: experience with the first 100 patients. Surg Endosc. 2009;23:2399–406.
Ikeda Y, Takami H, Sasaki Y, Takayama J, Niimi M, Kan S. Clinical benefits in endoscopic thyroidectomy by the axillary approach. J Am Coll Surg. 2003;196:189–95.
Lee J, Nah KY, Kim RM, Ahn YH, Soh EY, Chung WY. Differences in postoperative outcomes, function, and cosmesis: open versus robotic thyroidectomy. Surg Endosc. 2010;24:3186–94.
Miccoli P, Rago R, Massi M, Panicucci E, Metelli MR, Berti P, et al. Standard versus video-assisted thyroidectomy: objective postoperative pain evaluation. Surg Endosc. 2010;24:2415–7.
Del Rio P, Berti M, Sommaruga L, Arcuri MF, Cataldo S, Sianesi M. Pain after minimally invasive videoassisted and after minimally invasive open thyroidectomy—results of a prospective outcome study. Langenbecks Arch Surg. 2008;393:271–3.
Jeong JJ, Kang SW, Yun JS, Sung TY, Lee SC, Lee YS, et al. Comparative study of endoscopic thyroidectomy versus conventional open thyroidectomy in papillary thyroid microcarcinoma (PTMC) patients. J Surg Oncol. 2009;100:477–80.
Ryu HR, Kang SW, Lee SH, Rhee KY, Jeong JJ, Nam KH, et al. Feasibility and safety of a new robotic thyroidectomy through a gasless, transaxillary single-incision approach. J Am Coll Surg. 2010;211:e13–9.
Lee J, Lee JH, Nah KY, Soh EY, Chung WY. Comparison of endoscopic and robotic thyroidectomy. Ann Surg Oncol. 2011;18:1439–46.
Breivik H. Postoperative pain management: why is it difficult to show that it improves outcome? Eur J Anaesthesiol. 1998;15:748–51.
Carr D, Goudas LC. Acute pain. Lancet. 1999;353:2051–8.
Breivik H, Stubhaug A. Management of acute postoperative pain: still a long way to go! Pain. 2008;137:233–4.
Rolke R, Baron R, Maier C, Tölle TR, Treede RD, Beyer A, et al. Quantitative sensory testing in the German Research Network on Neuropathic Pain (DFNS): standardized protocol and reference values. Pain. 2006;123:231–43.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ryu, H.R., Lee, J., Park, JH. et al. A Comparison of Postoperative Pain After Conventional Open Thyroidectomy and Transaxillary Single-Incision Robotic Thyroidectomy: A Prospective Study. Ann Surg Oncol 20, 2279–2284 (2013). https://doi.org/10.1245/s10434-012-2557-2
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-012-2557-2