
Abstract
Background
Little is known about the interaction among surgeons, patients, and other physicians in selecting breast cancer surgery.
Methods
We contacted attending surgeons (n = 456) of a population-based sample of 2645 breast cancer patients diagnosed in Detroit and Los Angeles from December 2001 to January 2003. Eighty percent completed a written survey with clinical scenarios.
Results
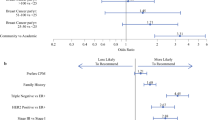
The mean surgeon age was 50 years, 50% practiced in a community hospital, and breast cancer averaged 31% of practice volume. The mean number of years in practice was 17.2. Female surgeons made up 14.4% of the sample and 35% of the high-volume surgeons. Conflict with patients and other providers was reported by 58% and 32% of surgeons, respectively. When the patient preferred mastectomy and the surgeon favored BCS, conflict was reported by 49.9% of surgeons. Compared with low-volume surgeons, high-volume surgeons were significantly more likely to report conflict in this scenario (44% vs 62%; P = .047). When another provider preferred mastectomy and the respondent surgeon favored BCS, conflict was reported by 34% of surgeons and was more common for high-volume surgeons (P < .001). In a logistic regression model, surgeon volume and practice setting were strongly associated with conflict in this scenario.
Conclusion
High-volume surgeons and those in cancer centers more frequently endorse current clinical guidelines that favor BCS over mastectomy, resulting in greater conflict with patients. These findings support patient reports that patient choice is a key factor in continued mastectomy use.


Similar content being viewed by others


References
Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med 2002; 347(16):1227–32
Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med 2002; 347(16):1233–41
Poggi MM, Danforth DN, Sciuto LC, et al. Eighteen-year results in the treatment of early breast carcinoma with mastectomy versus breast conservation therapy: the National Cancer Institute Randomized Trial. Cancer 2003; 98(4):697–702
Arriagada R, Le MG, Rochard F, Contesso G. Conservative treatment versus mastectomy in early breast cancer: patterns of failure with 15 years of follow-up data. Institut Gustave-Roussy Breast Cancer Group. J Clin Oncol 1996; 14(5):1558–64
Morrow M, White J, Moughan J, et al. Factors predicting the use of breast-conserving therapy in stage I and II breast carcinoma. J Clin Oncol 2001; 19(8):2254–62
Baxter NN, Virnig BA, Durham SB, Tuttle TM. Trends in the treatment of ductal carcinoma in situ of the breast. J Natl Cancer Inst 2004; 96(6):443–8
Farrow DC, Hunt WC, Samet JM. Geographic variation in the treatment of localized breast cancer. N Engl J Med 1992; 326(17):1097–101
Nattinger AB, Gottlieb MS, Veum J, et al. Geographic variation in the use of breast-conserving treatment for breast cancer. N Engl J Med 1992; 326(17):1102–7
Guadagnoli E, Weeks JC, Shapiro CL, et al. Use of breast-conserving surgery for treatment of stage I and stage II breast cancer. J Clin Oncol 1998; 16(1):101–6
Ernster VL, Barclay J, Kerlikowske K, et al. Incidence of and treatment for ductal carcinoma in situ of the breast. JAMA 1996; 275(12):913–8
Clauson J, Hsieh YC, Acharya S, et al. Results of the Lynn Sage Second-Opinion Program for local therapy in patients with breast carcinoma. Changes in management and determinants of where care is delivered. Cancer 2002; 94(4):889–94
Wennberg JE. Unwarranted variations in healthcare delivery: implications for academic medical centres. BMJ 2002; 325(7370):961–4
Lantz PV, Zemencuk JK, Katz SJ. Is mastectomy overused? A call for an expanded research agenda. Health Serv Res 2002; 37(2):417–31
Katz SJ, Lantz PM, Janz NK, et al. Patterns and correlates of local therapy for women with ductal carcinoma-in-situ. J Clin Oncol 2005; 23(13):3001–7
Katz SJ, Lantz PM, Janz NK, et al. Surgeon perspectives about local therapy for breast carcinoma. Cancer 2005; 104(9):1854–61
Katz SJ, Lantz PM, Janz NK, et al. Patient involvement in surgery treatment decisions for breast cancer. J Clin Oncol 2005; 23(24):5526–33
Dillman D. Mail and Telephone Surveys. New York: John Wiley and Sons, Inc., 1978
Anema MG, Brown BE. Increasing survey responses using the total design method. J Contin Educ Nurs 1995; 26(3):109–14
White J, Morrow M, Moughan J, et al. Compliance with breast-conservation standards for patients with early-stage breast carcinoma. Cancer 2003; 97(4):893–904
Fagerlin A, Lakhani I, Lantz PM, et al. An informed decision? Breast cancer patients and their knowledge about treatment. Patient Educ Couns 2006; 64(1–3):303–12
Morrow M, Mujahid M, Lantz PM, et al. Correlates of breast reconstruction: results from a population-based study. Cancer 2005; 104(11):2340–6
Lantz PM, Janz NK, Fagerlin A, et al. Satisfaction with surgery outcomes and the decision process in a population-based sample of women with breast cancer. Health Serv Res 2005; 40(3):745–67
Mastaglia B, Kristjanson LJ. Factors influencing women’s decisions for choice of surgery for Stage I and Stage II breast cancer in Western Australia. J Adv Nurs 2001; 35(6):836–47
Back A. Patient-physician communication in oncology: What does the evidence show? Oncology 2006; 20(1):67–74
Whelan T, Levine M, Willan A, et al. Effect of a decision aid on knowledge and treatment decision making for breast cancer surgery: a randomized trial. JAMA 2004; 292(4):435–41
Acknowledgment
We thank the American College of Surgeons Commission on Cancer (Connie Bura and David P. Winchester, MD) for their support.
This work was funded by a grant from the National Cancer Institute (RO1 CA8837-A1) to the University of Michigan. This project has been funded in part with Federal funds from the National Cancer Institute, National Institutes of Health, Department of Health and Human Services, under Contract No. N01-PC-35139 and NO1-PC-65064.
The collection of cancer incidence data used in this publication was supported by the California Department of Health Services as part of the statewide cancer reporting program mandated by California Health and Safety Code Section 103885. The ideas and opinions expressed herein are those of the author, and no endorsement by the State of California, Department of Health Services is intended or should be inferred.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Opatt, D., Morrow, M., Hawley, S. et al. Conflicts in Decision-Making for Breast Cancer Surgery. Ann Surg Oncol 14, 2463–2469 (2007). https://doi.org/10.1245/s10434-007-9431-7
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-007-9431-7