
Abstract
Background
The utilization of plants and plant resources for various ethnobotanical purposes is a common practice in local towns and villages of developing countries, especially in regard to human and veterinary healthcare. For this reason, it is important to unveil and document ethnomedicinal plants and their traditional/folk usage for human and livestock healthcare from unexplored areas. Here we advance our findings on ethnomedicinal plants from Haripur District, Pakistan, not only for conservation purposes, but also for further pharmacological screenings and applied research.
Methodology
Information of ethnomedicinal plants was obtained using a carefully planned questionnaire and interviews from 80 local people and traditional healers (Hakims) in Haripur District, Pakistan, from 2015 to 2017. Informed consent was obtained from each participant before conducting the interview process. Quantitative ethnobotanical indices, such as relative frequency of citation (RFC), use value (UV) and Jaccard index (JI), were calculated for each recorded species. Correlation analysis between the RFC and UV was tested by Pearson’s correlation, SPSS (ver. 16).
Results
A total of 80 plant species (33 herbs, 24 trees, 21 shrubs and 2 climbers) belonging to 50 families were being used in the study area to treat livestock and human diseases. Lamiaceae was the most dominant family with 7 species (8.7%), followed by Fabaceae with 6 species (7.5%), and Moraceae with 5 species (6.2%). Local people used different methods of preparation for different plant parts; among them, decoction/tea (22 species) was the popular method, followed by powder/grained (20 species) and paste/poultice (14 species). It was observed that most of the species (~ 12 to 16 species) were utilized to treat human and livestock digestive system-related problems, respectively. The Jaccard index found that plant usage in two studies (District Abbottabad and Sulaiman Range) was more comparable. Local people mainly relied on folk medicines due to their rich accessibility, low cost and higher efficacy against diseases. Unfortunately, this important traditional knowledge is vanishing fast, and many medicinal plants are under severe threat. The most threats associated to species observed in the study area include Dehri, Garmthun, Baghpur, Najafpur and Pharala.
Conclusion
The study has indicated that local people have higher confidence in the usage of ethnomedicinal plants and are still using them for the treatment of various ailments. Comparative analysis with other studies may strongly reflected the novel use of these plants, which may be due to the deep-rooted and unique socio-cultural setup of the study area. However, awareness campaigns, conservation efforts and pharmacological and applied research are required for further exploration and may be a step in the right direction to unveil prospective pharmaceuticals.
Similar content being viewed by others


Introduction
Humans have a long history of utilizing plants to fulfill various daily requirements. Plants are used as medicines, food, fodder for livestock and materials to construct houses [1]. The application of medicinal plants and herbs for therapeutic purposes is a global practice, and almost every country has benefitted from their useful therapeutic and medicinal elements [2]. Herbal medicines play a distinctive role from the primitive period until today in healthcare systems. The first ethnomedicinal plant in sub-continent history was recorded in Rigveda during 4500–1600 BC and Ayurveda 2500–600 BC [3]. The concepts of ethnobotanical medicines are thought to have originated from Greece and adopted by Arabs, thereafter learned and spread by Indians and Europeans [4,5,6]. Medicinal plants are an important part of the conventional healthcare system, as various allopathic drugs are extracted or derived from medicinal plants [7, 8]. The utilization of alternative medicine may increase due to its low costs, higher efficacy and increased faith in herbal remedies. Although allopathic medicines can treat several diseases, they are often more expensive and may have adverse effects, which forces common people to take advantage of herbal medicines, which may have fewer side effects [9]. Scientific investigations on medicinal plants have been underway in various countries due to their vast therapeutic potential and are also used as an alternative therapy in various healthcare systems [10].
Traditional veterinary medicine was first practiced around 1800 B.C. during the age of King Hammurabi of Babylon, who formulated laws and introduced a veterinary fee structure for treating animals [11]. Ethnoveterinary medicine (EVM) is the major source for the treatment of diseases in livestock throughout the world, even today. Humans have used herbal remedies to treat different diseases in domesticated animals since the advent of civilization. It is estimated that medicinal plants, for several centuries, have been widely used as a primary source of prevention and control of livestock diseases [12, 13]. Many studies have been carried out on treating specific ailments in livestock with herbal medicines and their derivatives [14]. Traditional EVM provides affordable therapy and easy accessibility in comparison to western medicines [15].
Pakistan is an agricultural country, and about 80% of its population depends on farming and livestock. Pakistan is the world's fifth-largest milk-producing country because of its high reliance on farming and livestock [16]. About 84% of Pakistan’s population depended on traditional medicine in the early 1950s, and a rapid decrease was recorded in recent years from traditional knowledge, now limited only to remote areas of Pakistan [17, 18]. Resource-poor farmers of Pakistan substantially depend upon traditional medicine because of their minimal access to modern-day healthcare systems and lack of well-developed basic healthcare units in their areas [3]. While much work has been done worldwide on documenting ethnoveterinary practices, in Pakistan, very little attention has been given to documentation of plants used as EVM, and there is an immense need to document this knowledge [19].
While literature has revealed that many ethnobotanical researchers have visited most parts of Pakistan in recent years, but no/less areas has been thoroughly explored regarding the EVM [20]. A similar trend is evident in human medicinal plant inventories, where many researchers and ethnobotanists have visited most parts of Pakistan and contributed to the records [20,21,22,23,24,25,26]. Still, much information and traditional knowledge remain to be recorded. The main aim of this study was (1) to document the traditional knowledge of ethnomedicinal plants from Haripur District, Khyber Pakhtunkhwa (Pakistan), an unexplored area which lacks such documentation, (2) to report the traditional folk knowledge, ethnomedicinal plant utilization along with recipes, mode of preparation, parts used, used form in veterinary and human healthcare by local and ethnic communities, (3) to identify potential conservation threats, (4) to compile the data of traditional knowledge of ethnomedicinal plants by using quantitative ethnomedicinal indices like UV, RFC and JI in order to evaluate the most frequently used species and access their matching with other studies published from Pakistan in traditional ethnomedicinal plant utilization. It is hypothesized that studies conducted in surrounding areas may more similar to present study which can be evaluated by JI value; and (5) to provide further research baseline to pharmacologists, phytochemists and conservationists for further research studies.
Materials and methods
This study was authorized by the Department of Bioscience and Office of Research, Innovation and Commercialization University of Wah (ORIC-UW), Wah Cantt, Pakistan. Informed consent was obtained from each informant before conducting the semi-structured interview process.
The research study was completed in four phases as follows, (1) description of the study area, (2) ethnomedicinal field survey (primary data), (3) plant’s identification and statistical analysis (secondary data) and (4) data compilation/documentation.
Study area
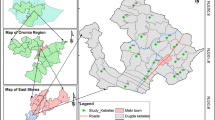
Haripur District is under the Khyber Pakhtunkhwa province of Pakistan, situated between 33° 44ʹ–34° 22ʹ N latitude and 72°–35ʹ to 73°–15ʹ E longitude, at approximately 610 m above the sea level (Fig. 1). The district's total area is 1725 km2, divided into sub-districts (Haripur, Khanpur and Ghazi) and subdivided into 44 Union Councils. Haripur District has distinct geographical significance as its boundaries touch Districts Abbottabad, Mansehra, Attock, Torghar, Swabi, Buner, Rawalpindi (Punjab province) and the capital of Pakistan (Islamabad) [27]. According to the National Institute of Population Studies (NIPS), the district's estimated population was 1,003,031 in 2017, having a population density of 580 residents per square kilometer. The dominant caste or tribe of District is Awan followed by Gujjar and Tanoli. The Haripur is largely a rural district, and about only 12% of the population resides in urban areas. The temperature in the area ranges from almost 39 °C in summer to less than 10 °C in winter. Agriculture is the primary source of livelihood of the rural population of the study area. The area's economic growth depends on pastures, crop diversity, cultivation of fodder species and the development of medicinal plants and livestock diversity.

Map of the study area showing sampling site of Haripur District, Pakistan
Field survey and data collection
The entire study area was regularly and seasonally (spring, summer, winter and autumn) visited from January 2015 to January 2017. In the study area, the primary target sites were Muslimabad, Barkot, Jatti Pind, Tofkian, Khanpur, Kalinjar, Barella, Hattar, Qazipur, Ghazi, Najafpur, Jabri, Nara Amazai, Rehana, Teer, Syria, Sirikot, Bagra, Beer and Dingi. The field survey aimed to gather field data and activities, such as (1) plant’s collection, (2) local knowledge concerning plants, (3) identifying associated consequences to plants through personal observation and interviews, (4) photography and (5) medicinal plant uses along with recipes, through semi-structured questionnaires, interviews, keen observations and group discussions. The questionnaire and interview method helped to document indigenous folk knowledge by involving knowledgeable persons, traditional healers (Hakims) and local people (Table 1). Respondents were chosen by random selection of residents who were considerably connected to plants and were interested in traditional healthcare. Interviews were conducted mostly in fields, and photographs were shown for identification with local plant name. Women were interviewed indirectly through male family members. Participants were briefed about the research objectives and were allowed to discontinue the interview at any time. Each informant was interviewed regularly every season. The national language of Pakistan (Urdu) and the native language of the study area (Hindko) were used as a medium of communication. Thereafter, an English language questionnaire was filled for each informant (Additional file 1).
Plant identification
Collected plant species were identified with the help of Flora of Pakistan, Flora of West Pakistan [28] and Flora of Punjab [29], and online Flora (www.efloras.org/). Plants names were also identified through literature, plant list (www.theplantlist.org), Medicinal plant names services (https://mpns.science.kew.org/mpns-portal/) [30]. The system proposed by Raunkiær [31, 32], and modified by Brown [33], was followed to categorize the collected plant specimens into their habits and life forms. Plants were submitted to the Herbarium, Department of Botany, Hazara University Mansehra (Pakistan), and vouchers were issued. For voucher specimen, standard herbarium techniques [34, 35] were strictly followed.
Quantitative and correlative analysis of ethnomedicinal data
The collected ethnomedicinal data were analyzed using different quantitative analyses, including relative frequency citation (RFC), use value (UV) of medicinal plant and Jaccard index (JI) analysis by comparing the present study with published work to access knowledge variation among different communities. The obtained data were presented in percentages and proportions.
Relative frequency citation (RFC)
The RFC was calculated without taking into account the use categories by following the formula [36].
RFC shows the importance of each species in the study area given by the FC (FC is the number of local informants reported the uses of plant species) divided by the total number of informants (N).
Use value (UV) of plant species
Use value (UV) determines the relative importance of plant species uses. It was calculated using the following formula [37].
where “UV” indicates the use value of individual species, “Ui” is the number of uses recoded for a given species by each informant and “N” represents the number of total informants.
Pearson’s correlation
Pearson’s correlation, SPSS (ver. 16), tested correlation analysis between the RFC and UV.
Jaccard index (JI)
To compare the study with published literature and to access the similarity and dissimilarity of traditional knowledge among different communities and areas, the Jaccard index was calculated using the following formula [38].
where ‘a’ represents the total number of species in area A (our study area), ‘b’ represents the number of species from other published area B and ‘c’ represents the number of common species in both A and B.
Results
Description of medicinal plant families
The high diversity of plant families in the study area can be deduced from the presence of 50 different families. Among them, Lamiaceae was the largest family having 7 species, followed by Fabaceae (6 species), Moraceae (5 species), Apocynaceae (4 species), Asteraceae, Euphorbiaceae, Rhamnaceae and Solanaceae (3 species each), Amaranthaceae, Apiaceae, Brassicaceae, Malvaceae, Meliaceae, Menispermaceae (2 species each) (Fig. 2) and remaining families with one species each.

Distribution of medicinal plant species according to their family in the study area
Medicinal plant enumerations
Eighty plants were recorded covered in this study; herbs (33, 41.2%) were dominant, followed by shrubs (21, 26.2%), trees (24, 30%) and climbers (2, 2.5%). Furthermore, life spans for the majority of plants were recorded as perennial (62, 77.5%), followed by annual (16, 20%) and biennial (2, 2.5%) (Fig. 3). Among these, 40 plant species were used for livestock healthcare, and 49 plant species were used to treat human diseases, including 9 plant species which were commonly used for both (human and livestock). Complete information about each plant species includes botanical name, family, local name, voucher number, habit, life span, locality, part used, either utilized to treat human or animal diseases or both, and their recipes are listed with RFC and UV in Tables 2, 3 and 4.

Description of medicinal A plant enumeration, B plant habit and C plant life span of the study area
Plant part(s) used
Locals utilized different plant parts (either in combination or separately) in the study area for the management of livestock and human diseases. Among them, leaves (47.9%) were the most commonly used part in herbal preparations, followed by fruits (16%), whole plant (8.5%), roots (7.4%), seeds (4.3%), bark (3.2%), gum, bulb, twigs, flower, resin (2.1% each), spines and pods (1.1% each) (Fig. 4A). In combination, leaves were the most common plant parts combined/utilized with fruits (3), flower, roots, seed and gum, twigs and stem (1 each). The combination of gum with the spine was utilized only one time (Fig. 4B).

Utilization of A plant parts B plant parts in combination for management of livestock and human diseases
Mode of preparation, administration and application
The remedies/recipes preparations of the 80 plant species are categorized according to their type of preparation, which revealed that decoction/tea (22 species) was a widely used preparation method by locals, followed by powdered/grinded (20 species), paste/poultice (14 species), directly eaten (12 species), juice/extract (09 species), roasted/cooked (07 species), crushed (04 species) and chewed (one species) (Fig. 5). It was also recorded that the local people use preparations/recipes of ethnomedicinal plant, both as externally (25%) and internally (75%) application.

Commonly used methods in the preparation of plant recipes
Species richness for the management of human and livestock diseases
Local people of the study area used 49 medicinal plants to treat 42 different ailments related to humans. These 42 ailments were further categorized into 12 major diseases categories. It was found that single medicinal plant species can treat several human ailments, and several medicinal plant species can treat single disease. In the study area, 34 livestock ailments were identified to be treated by 40 medicinal plants. These 34 ailments were further categorized into 07 major disease categories (Table 5). The ethnoveterinary medicinal plants were utilized mostly for cows (35%), followed by buffaloes (34%) and goats (31%).
Quantitative analysis
To analyze ethnomedicinal data, quantitative value indices were determined in this study. The RFC value ranges from 0.07 to 0.81 for the recorded species, and the highest value of RFC was recorded for Melia azedarach, Dodonaea viscosa, Grewia optiva and Mallotus philippensis (0.81, 0.77, 0.71 and 0.7), respectively.
The UV of plant species determines the relative importance of plants in the study area. The UV values for Curcuma longa, Adhatoda vasica, Viola odorata, Berberis lycium, Achyranthus aspera, Melia azedarach and Chenopodium album were 1.06, 1.01, 1.03, 0.98, 0.93, 0.91, 0.88, 0.87, 0.87 and 0.85, respectively, Phyllanthus emblica and Catharanthus roseus (0.82 each), Amaranthus viridis, Cannabis sativa, and Cynodon dactylon (0.81 each), and Ailanthus altissima and Solanum surattense (0.8 each). The other remaining plant species were recorded with a UV value of < 0.81, which indicated that they were less exploited by local people (Table 2). RFC and UV were significantly correlated (Pearson’s test; p = 0.01), and the correlated values explained approximately 31% of the data (Additional file 2: Table S1).
Comparison and Jaccard index
The comparative analysis exhibited a significant difference in the medicinal plant utilization among different communities of Pakistan. Twenty national studies from different areas of Pakistan were compared with the present study. Overall, 49 species were reportedly used to manage human diseases. Similarity percentages ranged from 0 to 57.1%. The similarity index (JI) value ranges from 1.76 to 16.85 (Table 6).
Furthermore, 25 national studies from the different areas of Pakistan were compared with the present 40 reported species for management of veterinary diseases. The similarity percentage ranges from 0 to 60%. The degree of similarity index (JI) value ranges from 1.17 to 32.78 (Table 7).
Major threats to plant diversity
Plant resources are under severe threats; the major threats (fires, overgrazing, overexploitation and mining activities) were observed in the visited localities of the study area. Among them, the plant diversity of Garmthun, Najafour, Dartian, Baghpur dehri and Jabri was exposed to all these major threats. Moreover, Sarae Nehmat Khan and Ghazi were less/non exposed to the threat activities except only overgrazing (Table 8).
Discussion
The utilization of medicinal plant species belonging to the dominant plant families (Lamiaceae, Moraceae, Apocynaceae, Asteraceae, etc.) in the study area suggests that the families may have wide distribution, or the plant species are well known to communities for their medicinal purpose. The traditional knowledge of various plant families had been published around the world; among them, Asteraceae, Lamiaceae and Moraceae are well known for their medicinal purpose among the people of Pakistan [20], and other parts of the world [3, 80,81,82]; this knowledge may be transferred over many different communities. In the traditional medicine system, herbaceous medicinal plant have been commonly used on a large scale compared to other types of plants [83,84,85,86]. The medicinal plant or their parts are collected in different seasons depending upon their availability or frequency of active constituent deposition. The accessibility and availability of plant species may also involve their utilization rate, such as perennial plants having longer life cycles than other plant life cycles [1, 87,88,89]. Thus, indigenous communities in the present study area were more likely to prefer perennial plants due to their long life-cycle and availability.
Plant parts, modes of preparation and application play a significant role in herbal medicine [90]. Most herbalists believe that plant leaves have various bioactive chemical compounds which can be easily extracted [5, 91]. Leaves were the most exploited part for medicinal purposes in the present study and several other studies [92, 93]. Furthermore, the collection of leaves may not threaten the plant survival compared to the collection of the whole plant, stem, or roots, which can drive the plant species to extinction if over-collected [94]. While extraction from fresh material would be considered more useful to avoid microbial fermentation [95], previous studies demonstrated that decoction is the most commonly used preparation method for ethnobotanical medicines by traditional healers in herbal recipes [96, 97]. This method may be commonly used due to its simplicity [98], or due to the heating process which speeds up biological reaction and results in higher availability of bioactive compounds [99,100,101]. In our study area, other areas of Pakistan [5, 82, 102, 103] and a few other countries [104,105,106,107,108], the most frequently used method of plant-based medicine preparation is decoction. In regard to the various preparation methods documented in our study, other studies have also revealed similar findings; the most frequently used method of preparation in Azad Jammu and Kashmir, Pakistan was decoction (18%), followed by powder and juice (17%), paste (15.5%), chewing (11%), extract (8%), infusion (7%) and poultice (5.5%) [97].
The traditional knowledge of herbal remedies for the management of various diseases may vary due to cultural differences, areas and communities. However, it is also believed that one plant species/part can treat various types of disease due to its diverse chemical constituents. Likewise, the present study demonstrated the traditional uses of Achyranthus aspera roots for tonsillitis, while its leaves were previously practiced for wound healing [109], Datura stramonium for bleeding piles, while in Haramosh and Bugrote Valleys, Pakistan, its leaves are practiced for injuries, wounds, bleedings and pains [52], Zanthoxylum armatum for jaundice, while in southern Himalayan regions of Pakistan, its branches are employed for toothache and edible fruits in cardiac disorders [110]. Moreover, in comparison with other studies revealed that some species have similar uses, and some plant species are exploited for different diseases [111,112,113], in addition to the folk herbal medicinal literature.
Likewise, some plant species we recorded in our study area reflect similar traditional veterinary uses compared to other traditional knowledge of ethnomedicinal plant studies. For example, Mallotus philippensis seed powder is used in abdominal worms to remove the threadworms [73], and Melia azedarach is used to reduce intestinal worm load in cattle, recoded with high a (100%) fidelity level [114]. In contrast, some studies reflect dissimilar traditional uses of plants, such as Grewia optiva for wound healing [58], leaves paste of Dodonaea viscosa is used as tonic and for wound healing [62, 115], fruits of Solanum surattense are used for pregnancy improvement [115], and in curing myiasis [31], the leaves and shoot of Carissa opaca are fed to increase the milk yield in goats [116], Berberis lycium root and stem powder for treat trauma in livestock in Afghanistan [117], Punica granatum is used in foot infection [118], fever, dehydration, internal parasite, tonic, indigestion, paralysis, gastric troubles, burns, flatulence and several other diseases [32, 118, 119], Adhatoda vasica leaves are used for cough in cow and goat [120], Cynodon dactylon leaves are used in burn injuries [121], leaves of Mentha arvensis are given to the animal if he stops taking food and also to cure bloat [116], Curcuma longa rhizome and Acacia modesta gums are used for skeleton-muscular ailments [122], and Amaranthus viridis fresh plant was given to cattle as purgative in case of constipation [19], Furthermore, Acacia nilotica is used to treat jaundice and dysentery [123], which may reflect the novel and the new uses of plant species in the present study area. Comparing present findings with previous studies shows that the same medicinal plant are used in different parts of the country for different diseases. Moreover, people also used different plant parts of the same plant for similar or different diseases.
Use value and RFC value are dynamic as it changes with area and depend on the traditional knowledge of the local people, so the UV and RFC value may vary within the same area or area to area and community to community [90]. The plant species with low UV or RFC value is considered less important species for the local people; in fact, young people may have limited knowledge to these species and may consider them unimportant, which is an alarming risk to traditional knowledge that is dependent on transference from generation to generation. As a result, this knowledge may gradually disappear.
Indigenous knowledge of the people may vary greatly due to discrepancies in their origins and cultures. Documenting and comparing this knowledge may reveal a considerable depth of knowledge among communities, resulting in novel sources for drug development [124]. Such studies also illustrate the value of indigenous medicinal plant information, with disparities between areas arising as a result of ecological [125], historical [126], phytochemical and even organoleptic differences [127]. Similar in terms of their cultural values and climatic conditions to the study area, the Jaccard index showed significant results; the highest degree of similarity index was with studies by Abbasi et al. [49], Shah and Khan [57], Ahmad [56], Mussarat et al. [13], with JI values 16.85, 11.86, 10.65 and 9.40, respectively, for the management of human diseases. Likewise, Tariq et al. [66], Abbasi et al. [69], Ch et al. [79],, Badar et al. [60] had JI values of 32.78, 16.9, 16.85, 13.88 and 13.33, respectively, for ethnoveterinary medicinal plant. The studies might have a cross-cultural exchange of knowledge between the communities through any means, historical and ecological factors, common ethnic values and similar vegetation types. The lowest JI values were for the studies conducted by Ahmad et al. [43], Afzal et al. [50], with JI values 1.76 and 1.98, respectively, for human disease management. Likewise, Dilshad et al. [27], Raziq et al. [75], Khuroo et al. [78] and Mirani et al. [68] had JI values of 0.98, 1.17, 2.04 and 2.08, respectively, for ethnoveterinary medicinal plant. These findings are in agreement with studies carried out by Kayani et al. [128]. This might be due to a greater difference in ethnobotanical knowledge due to differences in population size, species diversity, habitat structure, or less chance of exchanging cultural knowledge between the areas. The Jaccard index analysis may strengthen the value of reported medicinal plant species with their matching uses to other studies, which may provide a baseline for phytochemical, and pharmacognostic studies.
On the other hand, the JI analysis may reflect the novel uses of medicinal plant from the present study area, which may be due to the areas: (1) unique phytogeography, (2) distinguished indigenous culture and history, (3) remarkable phytodiversity, (4) existence of different tribes and castes, (5) differences in methods of medicinal plant collection, their processing, preparations, usage and storage, (6) ethnobotanical knowledge variations, (7) less chance of the exchange of cultural knowledge between the study area to other areas may be due to restricted movement of people because of their residences in remote and hilly areas, (8) absence of a proper system of documentation, sharing and conservation of folk knowledge, (9) least interest of the younger generation in folk knowledge and practices, (10) differences in plant parts used, diseases treated and recipes, such as our study area's preparation methods, are different from other areas of Pakistan for the same plant part and treated disease, and (11) ethnomedicinal use of plant in our study area may not be documented or published from other study areas.
During surveys, it was observed that local plant resources are severely threatened by forest fires in summer, overgrazing (nomadic and normal), overexploitation and mining activities. People living in the far-flung mountains of the area have no/or less modern healthcare system, so most people rely on medicinal plant, and unsustainable collection may drive the flora to extinction [129,130,131]. During our study, it was also unveiled that over time, important folk indigenous knowledge about plants was limited to older people only, as the younger people have less interest in folk knowledge and traditional practices due to transforming lifestyle and culture; this can be inferred from the informant’s knowledge by age, which showed informants 6.2%, ≤ 30 years of age.
Conclusion
In summary, the current study reported the important ethnomedicinal plant practiced in veterinary and human healthcare by the local people of District Haripur, Pakistan. Like the rural population of other countries, the local people also rely on medicinal plant to treat livestock and human diseases may due to traditional culture, easy availability and cheaper sources. Comparative analysis of the present study and their matching with other studies from Pakistan may reflect the novel use of these plants, which can provide a base line for pharmacognostic studies. Scientific and experimental validation of traditional knowledge is necessary to ensure safety and efficacy; therefore, the phytochemical, toxicological and clinical studies on the documented flora are recommended for a better understanding. In the study area, ethnomedicinal plant are also under severe threats, and combined efforts should be made to secure both the plant resources and folk knowledge. In this regard, awareness campaigns, conservation efforts and pharmacological and applied research studies are required.
Availability of data and materials
All the data are in manuscript and supporting documents.
Abbreviations
- EVM:
-
ethnoveterinary medicine
- RFC:
-
relative frequency of citation
- FC:
-
frequency citation
- ∑Ui:
-
sum of uses
- UV:
-
use values
- S:
-
shrubs
- H:
-
herbs
- C:
-
climbers
- T:
-
trees
- A:
-
annual
- B:
-
biennial
- P:
-
perennial
- RT:
-
root
- LE:
-
leaf
- ST:
-
stem
- FR:
-
fruit
- SH:
-
shoot
- WP:
-
whole plant
- BA:
-
bark
- SD:
-
seed
- RH:
-
rhizome
- FL:
-
flower
- GM:
-
gum
- RE:
-
resin
- BB:
-
bulb
- TW:
-
twigs
- PP:
-
pulp
- SP:
-
spine
References
Shinwari MI, Khan MA. Folk use of medicinal herbs of Margalla hills national park, Islamabad. J Ethnopharmacol. 2000;69:45–56.
Serrentino J. How natural remedies work. Point Roberts: Hartley & Marks Publishers; 1991. p. 224–7.
Abbasi AM, Khan MA, Shah MH, Shah MM, Pervez A, Ahmad M. Ethnobotanical appraisal and cultural values of medicinally important wild edible vegetables of Lesser Himalayas-Pakistan. J Ethnobiol Ethnomed. 2013;9:66.
Ahmad H. Issues regarding medicinal plants of Pakistan. Udyana Today. 1999;6:6–7.
Ahmad M, Sultana S, Fazl-i-Hadi S, Ben Hadda T, Rashid S, Zafar M, Khan MA, Khan MPZ, Yaseen G. An ethnobotanical study of medicinal plants in high mountainous region of Chail valley (District Swat-Pakistan). J Ethnobiol Ethnomed. 2014;10:36.
Khan M, Musharaf S. Ethnobotanical studies on plant resources of Sheikh Maltoon, District Mardan, Pakistan. Med Plant Res. 2014;4:35–45.
Rashid A, Arshad M. Medicinal plant diversity, threat imposition and interaction of a mountain people community. In: Proceedings of workshop on curriculum development in applied ethnobotany. Published by the Ethnobotany Project, WWF Pakistan; p. 84–90.
Maroyi A. Traditional use of medicinal plants in south-central Zimbabwe: review and perspectives. J Ethnobiol Ethnomed. 2013;9:31.
Kala CP. Current status of medicinal plants used by traditional Vaidyas in Uttaranchal state of India. Ethnobot Res Appl. 2005;3:267–78.
Ahmad I, Beg AZ. Antimicrobial and phytochemical studies on 45 Indian medicinal plants against multi-drug resistant human pathogens. J Ethnopharmacol. 2001;74:113–23.
Schillhorn van Veen TW. Sense or nonsense? Traditional methods of animal disease prevention and control in the African savannah. London: Ethnoveterinary Research and Development Intermediate Technology Publications; 1996. p. 25–36.
Hoareau L, DaSilva EJ. Medicinal plants: a re-emerging health aid. Electron J Biotechnol. 1999;2:3–4.
Mussarat S, AbdEl-Salam NM, Tariq A, Wazir SM, Ullah R, Adnan M. Use of ethnomedicinal plants by the people living around Indus River. Evid Based Complement Alternat Med. 2014;2014:14.
McGaw LJ, Van der Merwe D, Eloff J. In vitro anthelmintic, antibacterial and cytotoxic effects of extracts from plants used in South African ethnoveterinary medicine. Vet J. 2007;173:366–72.
Ganesan S, Chandhirasekaran M, Selvaraj A. Ethnoveterinary healthcare practices in southern districts of Tamil Nadu, Indian. J Tradit Knowl. 2008;7(2):347–435.
Ul Hassan H, Murad W, Tariq A, Ahmad A. Ethnoveterinary study of medicinal plants in Malakand Valley, District Dir (Lower), Khyber Pakhtunkhwa, Pakistan. Ir Vet J. 2014;67:6.
Baloch M, Marri M, Qaisrani M. Plants treasures, traditional knowledge and Baloch society. Bi-Annu Res J Balochistan Rev. 2013;28:1–5.
Ahmad KS, Habib S. Indigenous knowledge of some medicinal plants of Himalaya Region, Dawarian village, Neelum valley, Azad Jammu and Kashmir, Pakistan. Univ J Plant Sci. 2014;2:40–7.
Shah G, Ahmad M, Arshad M, Khan M, Zafar M, Sultana S. Ethno-phyto-veterinary medicines in northern Pakistan. J Anim Plant Sci. 2012;22:791–7.
Sharif A, Asif H, Younis W, Riaz H, Bukhari IA, Assiri AM. Indigenous medicinal plants of Pakistan used to treat skin diseases: a review. Chin Med. 2018;13:52.
Altaf R, Bhatti K, Mirza S, Ajaib M, Ishtiaq M. Ethnomedicinal Study of Tehsil Wazirabad Gujranwala Punjab Pakistan. Pak J of Sci. 2019;71:260.
Ishtiaq M, Mahmood A, Maqbool M. Indigenous knowledge of medicinal plants from Sudhanoti district (AJK), Pakistan. J Ethnopharmacol. 2015;168:201–7.
Ishtiaq M, Maqbool M, Ajaib M, Ahmed M, Hussain I, Khanam H, Mushtaq W, Hussain T, Azam S, Hayat Bhatti K. Ethnomedicinal and folklore inventory of wild plants used by rural communities of valley Samahni, District Bhimber Azad Jammu and Kashmir, Pakistan. PLoS ONE. 2021;16:e0243151.
Ishtiaq M, Maqbool M, Hussain T, Shah A. Role of indigenous knowledge in biodiversity conservation of an area: a case study on tree ethnobotany of Soona Valley, District Bhimber Azad Kashmir, Pakistan. Pak J Bot. 2013;45:245–56.
Ishtiaq M, Mumtaz AS, Hussain T, Ghani A. Medicinal plant diversity in the flora of Leepa Valley, Muzaffarabad (AJK), Pakistan. Afr J Biotechnol. 2012;11:3087–98.
Maqbool M, Ajaib M, Ishtiaq M, Azam S, Hussain T. Ethnomedicinal study of plants used in phytotherapeutics among indigenous communities of District Bhimber, Azad Kashmir and migrants to United Kingdom. Proc Pak Acad Sci B Life Environ Sci. 2019;2019(56):55–74.
Dilshad SR, Rehman N, Ahmad N, Iqbal A. Documentation of ethnoveterinary practices for mastitis in dairy animals in Pakistan. Pak Vet J. 2010;30:167–71.
Jabbar A, Raza MA, Iqbal Z, Khan MN. An inventory of the ethnobotanicals used as anthelmintics in the southern Punjab (Pakistan). J Ethnopharmacol. 2006;108:152–4.
Farooquee NA. Indigenous ethnoveterinary knowledge and livestock management amongst transhumant pastoralists of Central Himalaya. J Hum Ecol. 2000;11:319–22.
Yousufzai SA, Khan N, Wahab M, Ajaib M. Ethnomedicinal study of Marghazar valley, Pakistan. Int J Biol Biotechnol. 2010;7:409–16.
Farooq Z, Iqbal Z, Mushtaq S, Muhammad G, Iqbal MZ, Arshad M. Ethnoveterinary practices for the treatment of parasitic diseases in livestock in Cholistan desert (Pakistan). J Ethnopharmacol. 2008;118:213–9.
Dilshad SMR, Iqbal Z, Muhammad G, Iqbal A, Ahmed N. An inventory of the ethnoveterinary practices for reproductive disorders in cattle and buffaloes, Sargodha district of Pakistan. J Ethnopharmacol. 2008;117:393–402.
Hussain A, Khan MN, Iqbal Z, Sajid MS. An account of the botanical anthelmintics used in traditional veterinary practices in Sahiwal district of Punjab, Pakistan. J Ethnopharmacol. 2008;119:185–90.
Jain SK. Handbook of field and herbarium methods. Delhi: Today and Tomorrow Printers and Publishers; 1977.
Alexiades MN, Sheldon JW. Selected guidelines for ethnobotanical research: a field manual; advances in economic botany, vol. 10. Bronx: The New York Botanical Garden; 1996.
Vitalini S, Iriti M, Puricelli C, Ciuchi D, Segale A, Fico G. Traditional knowledge on medicinal and food plants used in Val San Giacomo (Sondrio, Italy): an alpine ethnobotanical study. J Ethnopharmacol. 2013;145:517–29.
Tardío J, Pardo-de-Santayana M. Cultural importance indices: a comparative analysis based on the useful wild plants of Southern Cantabria (Northern Spain). Econ Bot. 2008;62:24–39.
González-Tejero M, Casares-Porcel M, Sánchez-Rojas C, Ramiro-Gutiérrez J, Molero-Mesa J, Pieroni A, Giusti M, Censorii E, De Pasquale C, Della A. Medicinal plants in the Mediterranean area: synthesis of the results of the project Rubia. J Ethnopharmacol. 2008;116:341–57.
Jan H, Jan S, Ahmad N, Aysha M. Ethno-medicinal survey of indigenous medicinal plants used by the local population of Goleen Valley, Chitral, Pakistan. SM J Med Plant Stud. 2017;1:1–8.
Ullah Z, Ullah R, Shah GM, Majeed A, Hussain M, Ullah H. Ethnomedicinal plants of district charsadda Khyber Pakhtunkhwa, Pakistan. J Biodivers Environ Sci. 2016;9(2):254–64.
Shah GM, Jamal Z, Hussain M. Phytotherapy among the rural women of district Abbotabad. Pak J Bot. 2013;45:253–61.
Qureshi R. Medicinal flora of hingol national park, Baluchistan, Pakistan. Pak J Bot. 2012;44:725–32.
Ahmad KS, Qureshi R, Hameed M, Ahmad F, Nawaz T. Conservation assessment and medicinal importance of some plants resources from Sharda, Neelum Valley, Azad Jammu and Kashmir, Pakistan. Int J Agric Biol. 2012;14:997–1000.
Ghani A, Batool M. Folk recipes of some medicinal plants used by the inhabitants of soon valley khushab (Pakistan). Int J Curr Pharm Res. 2012;4:60–3.
Noor MJ, Kalsoom U. Ethnobotanical studies of selected plant species of Ratwal village, district Attock, Pakistan. Pak J Bot. 2011;43:781–6.
Arshad M, Nisar MF, Majeed A, Ismail S, Ahmad M. Ethnomedicinal flora in district Sialkot, Punjab, Pakistan. Middle East J Sci Res. 2011;9:209–14.
Tareen RB, Bibi T, Khan MA, Ahmad M, Zafar M, Hina S. Indigenous knowledge of folk medicine by the women of Kalat and Khuzdar regions of Balochistan, Pakistan. Pak J Bot. 2010;42:1465–85.
Wazir SM, Farooq A. Ethnobotanical survey of plants of Kurram river beds of district Bannu, Pakistan. Pak J Plant Sci. 2010;16:22–5.
Abbasi AM, Khan MA, Ahmed M, Zafar M. Herbal medicines used to cure various ailments by the inhabitants of Abbottabad district, North West Frontier Province, Pakistan. Anusandhan Bhawan: Council of Scientific and Industrial Research; 2010. p. 175–83.
Afzal S, Afzal N, Awan MR, Khan TS, Gilani A, Khanum R, Tariq S. Ethno-botanical studies from Northern Pakistan. J Ayub Med Coll Abbottabad. 2009;21:52–7.
Qureshi R, Waheed A, Arshad M, Umbreen T. Medico-ethnobotanical inventory of tehsil Chakwal, Pakistan. Pak J Bot. 2009;41:529–38.
Khan SW, Khatoon S. Ethnobotanical studies on some useful herbs of Haramosh and Bugrote valleys in Gilgit, northern areas of Pakistan. Pak J Bot. 2008;40:43.
Qureshi RA, Gilani SA, Ghufran MA. Ethnobotanical studies of plants of Mianwali district Punjab, Pakistan. Pak J Bot. 2007;39:2285–90.
Qureshi R, Gilani S, Ashraf M. Ethnobotanical studies with special reference to plants phenology at Sudhan Gali and Ganga Chotti Hills (District Bagh, AK). Elec J Env Agricult Food Chem. 2007;6:2207–15.
Panhwar AQ, Abro H. Ethnobotanical studies of Mahal Kohistan (Khirthar national park). Pak J Bot. 2007;39:2301–15.
Ahmad SS. Medicinal wild plants from Lahore-Islamabad motorway (M-2). Pak J Bot. 2007;39:355.
Shah GM, Khan MA. Checklist of Medicinal Plants of Siran Valley, Mansehra, Pakistan. Ethnobot Leafl. 2006;2006:6.
Aziz MA, Adnan M, Khan AH, Sufyan M, Khan SN. Cross-cultural analysis of medicinal plants commonly used in ethnoveterinary practices at South Waziristan Agency and Bajaur Agency, Federally Administrated Tribal Areas (FATA), Pakistan. J Ethnopharmacol. 2018;210:443–68.
Aziz MA, Khan AH, Adnan M, Ullah H. Traditional uses of medicinal plants used by Indigenous communities for veterinary practices at Bajaur Agency, Pakistan. J Ethnobiol Ethnomed. 2018;14:11.
Badar N, Iqbal Z, Sajid M, Rizwan H, Jabbar A, Babar W, Khan M, Ahmed A. Documentation of ethnoveterinary practices in district Jhang, Pakistan. J Anim Plant Sci. 2017;27:398–406.
Ahmad KS, Hamid A, Nawaz F, Hameed M, Ahmad F, Deng J, Akhtar N, Wazarat A, Mahroof S. Ethnopharmacological studies of indigenous plants in Kel village, Neelum Valley, Azad Kashmir, Pakistan. J Ethnobiol Ethnomed. 2017;13:68.
Adil S, Adnan, Ali M, Ajmal M, Ahmad N, Khan F. Ethno-veterinary medicinal plants of Chail valley. J Bio Env Sci. 2017;10:133–9.
Tariq A, Adnan M, Mussarat S. Use of ethnoveterinary medicines by the people living near Pak-Afghan border region. Slov Vet Res. 2016;53:119–30.
Khattak NS, Nouroz F, Rahman IU, Noreen S. Ethno veterinary uses of medicinal plants of district Karak, Pakistan. J Ethnopharmacol. 2015;171:273–9.
Khan MA, Ullah A, Rashid A. Ethnoveterinary medicinal plants practices in district Peshawar, Khyber Pakhtunkhwa Pakistan. Pak J Bot. 2015;47:105–14.
Tariq A, Mussarat S, Adnan M, AbdElsalam NM, Ullah R, Khan AL. Ethnoveterinary study of medicinal plants in a tribal society of Sulaiman range. Sci World J. 2014;2014:10.
Mussarat S, Amber R, Tariq A, Adnan M, AbdElsalam NM, Ullah R, Bibi R. Ethnopharmacological assessment of medicinal plants used against livestock infections by the people living around Indus river. BioMed Res Int. 2014;2014:14.
Mirani A, Mirbahar K, Bhutto A, Qureshi T. Use of medicinal plants for the treatment of different sheep and goat diseases in Tharparkar, Sindh, Pakistan. Pak J Agric Agric Eng Vet Sci. 2014;30:242–50.
Abbasi AM, Khan SM, Ahmad M, Khan MA, Quave CL, Pieroni A. Botanical ethnoveterinary therapies in three districts of the Lesser Himalayas of Pakistan. J Ethnobiol Ethnomed. 2013;9:84.
ul Islam M, Anwar Z, Tabassum S, Khan SA, Zeb AC, Abrar M, Khattak KU, Khattak JZK. Plants of ethno-veterinary uses of Tunglai mountain Baffa Mansehra, Pakistan. Int J Anim Vet Adv. 2012;4:221–4.
Haq F. The ethno botanical uses of medicinal plants of Allai Valley, Western Himalaya Pakistan. Int J Plant Res. 2012;2:21–34.
Sindhu ZUD, Ullah S, Rao ZA, Iqbal Z, Hameed M. Inventory of ethno-veterinary practices used for the control of parasitic infections in district Jhang. Pakistan. Int J Agric Biol. 2012;14:922–8.
Khan MA, Khan MA, Hussain M. Ethno veterinary medicinal uses of plants of Poonch Valley Azad Kashmir. Pak J Weed Sci Res. 2012;18:495–507.
Zia-ud-Din S, Zafar I, Khan MN, Jonsson N, Muhammad S. Documentation of ethnoveterinary practices used for treatment of different ailments in a selected hilly area of Pakistan. Int J Agric Biol. 2010;12:353–8.
Raziq A, de Verdier K, Younas M. Ethnoveterinary treatments by dromedary camel herders in the Suleiman Mountainous Region in Pakistan: an observation and questionnaire study. J Ethnobiol Ethnomed. 2010;6:16.
Khan FM. Ethno-veterinary medicinal usage of flora of Greater Cholistan desert (Pakistan). Pak Vet J. 2009;29:75–80.
Deeba F, Muhammad G, Iqbal Z, Hussain I. Appraisal of ethno-veterinary practices used for different ailments in dairy animals in peri-urban areas of Faisalabad (Pakistan). Int J Agric Biol. 2009;11:535–41.
Khuroo AA, Malik AH, Dar A, Dar G, Khan Z. Ethnoveterinary medicinal uses of some plant species by the Gujjar tribe of the Kashmir Himalaya. Asian J Plant Sci. 2007;6:148–52.
Ch MI, Khan M, Hanif W. Ethno veterinary medicinal uses of plants from Samahni valley dist. Bhimber, (Azad Kashmir) Pakistan. Asian J Plant Sci. 2006;5:390–6.
Ahmed N, Mahmood A, Tahir S, Bano A, Malik RN, Hassan S, Ashraf A. Ethnomedicinal knowledge and relative importance of indigenous medicinal plants of Cholistan desert, Punjab Province, Pakistan. J Ethnopharmacol. 2014;155:1263–75.
Kadir MF, Sayeed MSB, Setu NI, Mostafa A, Mia M. Ethnopharmacological survey of medicinal plants used by traditional health practitioners in Thanchi, Bandarban Hill Tracts, Bangladesh. J Ethnopharmacol. 2014;155:495–508.
Bibi T, Ahmad M, Tareen RB, Tareen NM, Jabeen R, Rehman S-U, Sultana S, Zafar M, Yaseen G. Ethnobotany of medicinal plants in district Mastung of Balochistan province-Pakistan. J Ethnopharmacol. 2014;157:79–89.
Giday M, Asfaw Z, Woldu Z. Ethnomedicinal study of plants used by Sheko ethnic group of Ethiopia. J Ethnopharmacol. 2010;132:75–85.
Ragupathy S, Steven NG, Maruthakkutti M, Velusamy B, Ul-Huda MM. Consensus of the’Malasars’ traditional aboriginal knowledge of medicinal plants in the Velliangiri holy hills, India. J Ethnobiol Ethnomed. 2008;4:8.
Uniyal SK, Singh K, Jamwal P, Lal B. Traditional use of medicinal plants among the tribal communities of Chhota Bhangal, Western Himalaya. J Ethnobiol Ethnomed. 2006;2:14.
Singh G, Joyce EM, Beddow J, Mason TJ. Evaluation of antibacterial activity of ZnO nanoparticles coated sonochemically onto textile fabrics. J Microbiol Biotechnol Food Sci. 2020;9:106–20.
Ahmed E, Arshad M, Saboor A, Qureshi R, Mustafa G, Sadiq S, Chaudhari SK. Ethnobotanical appraisal and medicinal use of plants in Patriata, New Murree, evidence from Pakistan. J Ethnobiol Ethnomed. 2013;9:13.
Moerman DE. An analysis of the food plants and drug plants of native North America. J Ethnopharmacol. 1996;52:1–22.
Andriamparany JN, Brinkmann K, Jeannoda V, Buerkert A. Effects of socio-economic household characteristics on traditional knowledge and usage of wild yams and medicinal plants in the Mahafaly region of south-western Madagascar. J Ethnobiol Ethnomed. 2014;10:82.
Shoaib G, Shah GM, Shad N, Dogan Y, Siddique Z, Shah AH, Farooq M, Khan KR, Nedelcheva A. Traditional practices of the ethnoveterinary plants in the Kaghan Valley, Western Himalayas-Pakistan. Rev Biol Trop. 2020;69(1):1–11.
Bano A, Ahmad M, Zafar M, Sultana S, Rashid S, Khan MA. Ethnomedicinal knowledge of the most commonly used plants from Deosai Plateau, Western Himalayas, Gilgit Baltistan, Pakistan. J Ethnopharmacol. 2014;155:1046–52.
Šavikin K, Zdunić G, Menković N, Živković J, Ćujić N, Tereščenko M, Bigović D. Ethnobotanical study on traditional use of medicinal plants in South-Western Serbia, Zlatibor district. J Ethnopharmacol. 2013;146:803–10.
Khan MPZ, Ahmad M, Zafar M, Sultana S, Ali MI, Sun H. Ethnomedicinal uses of edible wild fruits (EWFs) in Swat Valley, Northern Pakistan. J Ethnopharmacol. 2015;173:191–203.
Zheng X, Xing F. Ethnobotanical study on medicinal plants around Mt. Yinggeling, Hainan Island, china. J Ethnopharmacol. 2009;124:197–210.
Organization WH. WHO guidelines on good herbal processing practices for herbal medicines. WHO technical report series; 2018.
Umair M, Altaf M, Abbasi AM. An ethnobotanical survey of indigenous medicinal plants in Hafizabad district, Punjab-Pakistan. PLoS ONE. 2017;12:0177912.
Amjad MS, Qaeem MF, Ahmad I, Khan SU, Chaudhari SK, Zahid Malik N, Shaheen H, Khan AM. Descriptive study of plant resources in the context of the ethnomedicinal relevance of indigenous flora: a case study from Toli Peer National Park, Azad Jammu and Kashmir, Pakistan. PLoS ONE. 2017;12:e0171896.
El Amri J, El Badaoui K, Zair T, Bouharb H, Chakir S, Alaoui TEM. Ethnobotanical study of medicinal plants in the region El Hajeb (central Morocco). J Res Biol. 2015;4:1568–80.
Chen G, Yang M, Song Y, Lu Z, Zhang J, Huang H, Guan S, Wu L, Guo D. Comparative analysis on microbial and rat metabolism of ginsenoside Rb1 by high-performance liquid chromatography coupled with tandem mass spectrometry. Biomed Chromatogr. 2008;22:779–85.
Han J, Ye M, Guo H, Yang M, Wang B, Guo D. Analysis of multiple constituents in a Chinese herbal preparation Shuang-Huang-Lian oral liquid by HPLC-DAD-ESI-MSn. J Pharm Biomed Anal. 2007;44:430–8.
Zhang J, Cui M, He Y, Yu H, Guo D. Chemical fingerprint and metabolic fingerprint analysis of Danshen injection by HPLC–UV and HPLC–MS methods. J Pharm Biomed Anal. 2005;36:1029–35.
Kayani S, Ahmad M, Zafar M, Sultana S, Khan MPZ, Ashraf MA, Hussain J, Yaseen G. Ethnobotanical uses of medicinal plants for respiratory disorders among the inhabitants of Gallies-Abbottabad, Northern Pakistan. J Ethnopharmacol. 2014;156:47–60.
Mahmood A, Mahmood A, Malik RN, Shinwari ZK. Indigenous knowledge of medicinal plants from Gujranwala district, Pakistan. J Ethnopharmacol. 2013;148:714–23.
Belayneh A, Bussa NF. Ethnomedicinal plants used to treat human ailments in the prehistoric place of Harla and Dengego valleys, eastern Ethiopia. J Ethnobiol Ethnomed. 2014;10:1–17.
Inta A, Trisonthi P, Trisonthi C. Analysis of traditional knowledge in medicinal plants used by Yuan in Thailand. J Ethnopharmacol. 2013;149:344–51.
Manandhar NP. An inventory of some herbal drugs of Myagdi District, Nepal. Econ Bot. 1995;49:371–9.
Song M-J, Kim H, Heldenbrand B, Jeon J, Lee S. Ethnopharmacological survey of medicinal plants in Jeju Island, Korea. J Ethnobiol Ethnomed. 2013;9:48.
Šarić-Kundalić B, Dobeš C, Klatte-Asselmeyer V, Saukel J. Ethnobotanical study on medicinal use of wild and cultivated plants in middle, south and west Bosnia and Herzegovina. J Ethnopharmacol. 2010;131:33–55.
Fikru A, Makonnen E, Eguale T, Debella A, Mekonnen GA. Evaluation of in vivo wound healing activity of methanol extract of Achyranthes aspera L. J Ethnopharmacol. 2012;143:469–74.
Qureshi RA, Ghufran MA, Gilani SA, Yousaf Z, Abbas G, Batool A. Indigenous medicinal plants used by local women in southern Himalayan regions of Pakistan. Pak J Bot. 2009;41:19–25.
Hussain K, Shahazad A, Zia-ul-Hussnain S. An ethnobotanical survey of important wild medicinal plants of Hattar district Haripur, Pakistan. Ethnobot Leafl. 2008;2008:5.
Sarwat S, Ahmad N. Screening of potential medicinal plants from district Sawat specific for controlling women diseases. Pak J Bot. 2012;44:1193–8.
Hazrat A, Nisar M, Shah J, Ahmad S. Ethnobotanical study of some elite plants belonging to Dir, Kohistan valley, Khyber Pukhtunkhwa. Pakistan Pak J Bot. 2011;43:787–95.
Ahmed MJ, Murtaza G. A study of medicinal plants used as ethnoveterinary: harnessing potential phytotherapy in Bheri, district Muzaffarabad (Pakistan). J Ethnopharmacol. 2015;159:209–14.
Khan MS, Razzaq A. Ethnobotanical indices based ethnoveterinary plant profile of Jabban hills, Malakand, Hindukush range. Pakistan Pak J Bot. 2018;50:1899–905.
Sharma R, Manhas R, Magotra R. Ethnoveterinary remedies of diseases among milk yielding animals in Kathua, Jammu and Kashmir. India J Ethnopharmacol. 2012;141:265–72.
Davis DK, Quraishi K, Sherman D, Sollod A, Stem C. Ethnoveterinary medicine in Afghanistan: an overview of indigenous animal health care among Pashtun Koochi nomads. J Arid Environ. 1995;31:483–500.
Chetri BK. Ethnobotanical study of south eastern foothills of Bhutan. Asian Plant Res J. 2019;2:1–20.
Pande P, Tiwari L, Pande H. Ethnoveterinary plants of Uttaranchal—a review. Indian J Tradit Knowl. 2007;3:444–58.
Parthiban R, Vijayakumar S, Prabhu S, Yabesh JGEM. Quantitative traditional knowledge of medicinal plants used to treat livestock diseases from Kudavasal taluk of Thiruvarur district, Tamil Nadu. India Rev Bras Farmacogn. 2016;26:109–21.
Sehgal AB, Sood S. Ethnoveterinary practices for herbal cure of livestock used by rural populace of Hamirpur, (HP), Inida. IOSR J Agri Vet Sci. 2013;3:7–14.
Ahmad K, Ahmad M, Weckerle C. Ethnoveterinary medicinal plant knowledge and practice among the tribal communities of Thakht-e-Sulaiman hills, west Pakistan. J Ethnopharmacol. 2015;170:275–83.
Kumar GMP, Nagayya S. Utilization of ethno-veterinary medicinal plants in Hassan district of Karnataka, India. Int J Pharm Pharm Sci. 2017;9:40.
Leonti M. The future is written: impact of scripts on the cognition, selection, knowledge and transmission of medicinal plant use and its implications for ethnobotany and ethnopharmacology. J Ethnopharmacol. 2011;134:542–55.
Ladio A, Lozada M, Weigandt M. Comparison of traditional wild plant knowledge between aboriginal communities inhabiting arid and forest environments in Patagonia. Argent J Arid Environ. 2007;69:695–715.
Moerman DE. Native American ethnobotany: Timber press. Edinb J Bot. 1998;56(2):317–8.
Leonti M, Sticher O, Heinrich M. Antiquity of medicinal plant usage in two Macro-Mayan ethnic groups (Mexico). J Ethnopharmacol. 2003;88:119–24.
Kayani S, Ahmad M, Sultana S, Shinwari ZK, Zafar M, Yaseen G, Hussain M, Bibi T. Ethnobotany of medicinal plants among the communities of Alpine and Sub-alpine regions of Pakistan. J Ethnopharmacol. 2015;164:186–202.
Ishtiaq M, Iqbal P, Hussain T. Ethnobotanical uses of gymnosperms of Neelam valley and Muzaffarabad of Kashmir. Pak J Bot. 2012;44:245–56.
Ishtiaq M, Maqbool M, Hussain T. Interrelationship of cultural diversity and biodiversity and its impact on conservation. Pak J Bot. 2012;44:245–56.
Majid A, Ahmad H, Saqib Z, Rahman IU, Khan U, Alam J, Shah AH, Jan SA, Ali N. Exploring threatened traditional knowledge; ethnomedicinal studies of rare endemic flora from Lesser Himalayan region of Pakistan. Rev Bras Farmacogn. 2019;29:785–92.
Acknowledgements
The authors thankfully acknowledge the free participation of the traditional healers and other local respondents who provided relevant information about the medicinal plant and made this survey possible. The authors also extend their thanks to Russell Gray (Wildlife Ecology & Conservation Consultant) for the English language editing of the manuscript.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
N.S. and A.N. contributed to conceptualization; G.M.S., Z.S. and N.S. provided methodology; N.S. provided software; Z.S., M.H. and A.M. performed validation; N.S. and Z.S. carried out formal analysis and investigation; A.N., M.S. and L.Y. performed data curation; Z.S. and N.S. performed writing—original draft preparation; N.S., G.M.S. and A.N. performed writing—review and editing; G.M.S. and M.I. done supervision; I.K. contributed to funding acquisition. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was authorized by the Department of Bioscience and Office of Research, Innovation and Commercialization University of Wah (ORIC-UW), Wah Cantt, Pakistan.
Consent for publication
All authors read and approved the final manuscript for publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: File S1
. Sample of questionnaire used during field survey for obtaining ethnobotanical information
Additional file 2: Fig. S1
. Description of the study area, Haripur District, Khyber Pakhtunkhwa, Pakistan. Fig. S2. Images of some ethnoveterinary medicinal plant of District Haripur. Table S1. Relationship between Relative frequency of citation (RFC) and Use Value (UV)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Siddique, Z., Shad, N., Shah, G.M. et al. Exploration of ethnomedicinal plants and their practices in human and livestock healthcare in Haripur District, Khyber Pakhtunkhwa, Pakistan. J Ethnobiology Ethnomedicine 17, 55 (2021). https://doi.org/10.1186/s13002-021-00480-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13002-021-00480-x