
Abstract
Background
Asthma is often poorly controlled and guidelines are often inadequately followed in medical practice. In particular, the prescription of non-asthma-specific drugs can affect the quality of care. The goal of this study was to measure the frequency of the prescription of antibiotics and anxiolytics/hypnotics to asthmatic patients and to look for associations between sex or age and the prescription of these drugs.
Methods
A cross-sectional study was conducted using computerised medical records from French and Italian general practitioners’ networks. Patients were selected according to criteria adapted from the HEDIS (Healthcare Effectiveness Data and Information Set) criteria. The outcome measure was the number of antibiotics or anxiolytics/hypnotics prescriptions per patient in 1 year. Parallel multivariate models were developed.
Results
The final sample included 3,093 French patients (mean age 27.6 years, 49.7% women) and 3,872 Italian patients (mean age 29.1 years, 48.7% women). In the univariate analysis, the French patients were prescribed fewer antibiotics than the Italian patients (37.1% vs. 42.2%, p < 0.00001) but more anxiolytics/hypnotics (17.8% vs. 6.9%, p < 0.0001). In the multivariate models, the female patients were more likely to receive antibiotics (odds ratio: 1.5 [1.3–1.7]) and anxiolytics/hypnotics (odds ratio: 1.8 [1.5–2.1]).
Conclusions
The prescription of antibiotics and anxiolytics/hypnotics to asthmatic patients is frequent, especially in women. Asthma guidelines should address this issue by referring to other guidelines covering the prescription of non-asthma-specific drugs, and alternative non-pharmacological interventions should be considered.
Similar content being viewed by others

Background
Despite international guidelines [1], the proportion of patients with uncontrolled asthma remains high, independent of disease severity [2,3]. Among asthma-specific drugs, inhaled corticosteroids are often underused, and rescue medication is frequently overused [4,5]. Studies investigating insurance claims data have suggested that non-asthma-specific drugs such as antibiotics [6] or anxiolytics/hypnotics are widely prescribed to asthmatic patients [7] and to the general population [8,9]. The prescription of first-line antibiotics in primary care increases the population carriage of resistant organisms in the community and the use of second-line antibiotics [10]. Prescription of anxiolytics and hypnotics in primary care leads to addiction and other side effects such as daytime fatigue, ataxia, falls, and road traffic incidents [11]. Importantly, the actual prescribing of these drugs to asthmatic patients has been poorly studied in primary care practice. Direct comparisons of patients receiving and not receiving these prescriptions are lacking. This study aimed to measure the frequency of the prescription of antibiotics and anxiolytics/hypnotics to asthmatic patients and to look for any association between sex or age and the prescriptions of these drugs. We specifically compared the prescription profiles in general practice in two European countries with different healthcare systems for which comparable databases are available, namely France and Italy.
Methods
Data sources
We conducted a cross-sectional study using data from computerised French and Italian primary care databases. These two clinical databases, operated by Cegedim Strategic Data, collect consultation data from a network of 1200 general practitioners (GPs) (3% of French GPs) [12] distributed across France and a network of 700 GPs (1.3% of Italian GPs) [13] across Italy. Participating GPs continuously and voluntarily provide anonymised and coded patient data to a centralised database using an electronic health record system that is common within each country. In both countries, participating GPs are selected to be representative of the French and Italian populations, respectively, according to three main criteria: geographical area, age, and sex. Activity and prescription habits of the panels have also been compared with national data and shown to be representative [14-16]. This procedure has been approved in France by the National Data Protection Authority (ethics committee) since 2002 (reference number: 770334) and in Italy by the National Data Protection Authority since 2004 (no reference number). The data include patient demographic characteristics and the diagnoses and prescriptions related to each consultation. The quality of these databases has been checked regularly, and they have been used frequently for pharmacoepidemiological studies [17,18].
Data extraction
The following variables were extracted from the databases: patient age and sex, number of visits to the GP and prescribed drugs, classified according to the Anatomical Therapeutic Chemical classification (ATC) [19]. Asthma drug categories belong to the ATC class R03 (Drugs for obstructive airway diseases) and include short-acting inhaled beta-agonists, long-acting inhaled beta-agonists (R03AC), oral beta-agonists (R03CC), theophylline (R03DA04), cromoglicic acid (R03BC), inhaled corticosteroids (R03BA), anticholinergics and leukotriene receptor antagonists (alone or in combination) (R03DC). We also extracted data on the use of oral corticosteroids (HA02AB). The following antibiotics were used for respiratory tract infections: tetracyclines (J01A), amphenicols (J01B), macrolides (J01F), beta-lactams (J01C), sulphonamides (J01E), cephalosporins (J01D), aminoglycosides (J01G) and quinolones (J01M). We also extracted data on all anxiolytics (N05B), hypnotics/sedatives (N05C), nasal preparations (R01) and antidepressants (N06A).
Inclusion criteria
From a pre-selected group of patients with at least one R03 prescription in 2007, we included in the analyses all patients between the ages of 13 and 40 years on the first of January 2008 who consulted during the year 2007 or 2008 and who fulfilled the asthma criteria derived from Health Employer Data and Information Set criteria (HEDIS criteria) [20]. These criteria are based on prescriptions and are more accurate in retrieving data on asthmatic patients than criteria based on diagnostic label [21]. These criteria consisted of the prescription of four or more units of any ATC R03 class drug (alone or in combination), or four or more outpatient visits with a diagnosis of asthma and two or more drug prescriptions used in the treatment of asthma, within a year. Patients with any prescription of tiotropium bromide (R03BB04) in 2007 or 2008 were excluded, as well as those over 40 years old, to limit the risk of confusion with chronic obstructive pulmonary disease diagnosis.
Statistical analyses
We used the issue of at least one prescription (one drug box versus none) as the outcome variable. First, the proportion of patients who received a prescription of at least one box of antibiotics or anxiolytics/hypnotics in 2008 was estimated for France and Italy. Then, these patients were compared with the other patients using a chi-square test for univariate analyses and a logistic regression model for multivariate analyses. These statistical analyses were performed using SAS 9.3 software (SAS Institute Inc., Cary, NC, USA). The selected level of significance was 0.05. In the univariate analyses, we estimated the prescription frequencies of at least one antibiotic and one hypnotic/sedative or anxiolytic in 2008. Using chi-square tests, we compared these frequencies between France and Italy and assessed the influence of patient age and sex, as well as the influence of the prescription of nasal preparations and antidepressants, as indicators of conditions frequently associated with asthma, such as rhinitis and depression.
Multivariate analyses were then conducted, based on logistic regression models after combining the French and Italian samples. We estimated odds ratios adjusted for asthma control criteria and severity (aOR), i.e. more than six prescriptions of short-acting inhaled beta-agonists (R03AC excluding R03AC12, R03AC13, R03AC14 and R03AC18) in 2008; the prescription of at least one inhaled corticosteroid (R03BA) in 2008, one inhaled asthma controller (R03AC12, R03AC13, R03AC14, R03AC18, R03AK06, R03AK07, R03BA, R03BC, R03DC, R03DA, R03DB or R03DX05), one oral corticosteroid (HA02AB) or the number of asthma drug units (R03; 1–7, 8–14, ≥15); and more than 12 visits to the GP with a prescription of an ATC R03 class medication in 2008.
Results
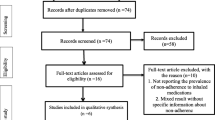
The final sample included 3,093 French patients (mean age 27.6 years, 49.7% women) and 3,878 Italian patients (mean age 29.1 years, 48.7% women) (Figure 1). From our database, we estimated baseline proportions of 29.1% in France and 36.2% in Italy for non-asthmatic patients aged from 13 to 40 years in 2008 who were prescribed at least one box of antibiotics. For anxiolytics/hypnotics, the respective estimates were 9.5% in France and 3.2% in Italy. After adjustment for age, the prescription of antibiotics and anxiolytics/hypnotics was higher in asthmatic patients, as compared with non-asthmatic patients both in France (OR = 1.4, 95% CI [1.3–1.5] and OR = 2.1, 95% CI [1.9–2.3]) and in Italy (OR = 1.3, 95% CI [1.2–1.4] and OR = 2.2, 95% CI [1.9–2.5]) (Table 1).

Sample selection in France and Italy.
Prescription of antibiotics
The proportion of asthmatic patients having at least one prescription of antibiotics in 2008 was higher in Italy than in France (42.1% vs. 37.1%, p < 0.0001). These prescriptions were more frequent in older patients in Italy and in female patients in both France and Italy (Table 2).
Prescription of anxiolytics/hypnotics
The proportion of asthmatic patients with at least one prescription for anxiolytics or hypnotics in 2008 was more frequent in France than in Italy (17.8% vs. 6.9%, p < 0.0001). The prescription of anxiolytics or hypnotics was more frequent in older and female patients in both countries (Table 3).
In the multivariate analyses (Table 4), the prescription of antibiotics was less frequent in France than in Italy (aOR = 0.8, 95% CI [0.7–0.9]) and more frequent in female than in male patients (aOR = 1.5, 95% CI [1.3–1.6]). The prescription of antibiotics was also associated with the prescription of nasal preparations (aOR = 2.0, 95% CI [1.7–2.2]). The prescription of anxiolytics or hypnotics was more frequent in France than in Italy (aOR = 5.0, 95% CI [3.4–5.3]), in female patients (aOR = 1.8, 95% CI [1.5–2.1]) and in older patients (aOR = 1.9, 95% CI [1.3–2.8] between 18 and 30 years and 3.3, 95% CI [2.3–4.7] between 31 and 40 years). The prescription of these drugs was associated with the prescription of antidepressants (aOR = 9.6, 95% CI [7.7–11.9]).
Discussion
Main findings
Using the data from two large computerised databases, we observed that non-asthma-specific drugs are commonly prescribed to asthmatic patients in France and Italy. In particular, in 2008, 37.1% of the French patients and 42.1% of the Italian patients were prescribed antibiotics, and 17.8% of the French patients and 6.9% of the Italian patients were prescribed anxiolytics or hypnotics. A higher frequency of prescription was observed for female patients for these two drug categories in both countries and in older patients for anxiolytics or hypnotics in France. These results are comparable to known rates of prescription for antibiotics, anxiolytics and hypnotics in non-asthmatic patients.
Strengths and limitations
A strength of this study is the use of accurate drug prescription data from community-based general practice, where asthmatic patients are treated most of the time. Our data come from France and Italy, countries with poor documentation of primary care performance [22]. Our analyses are based on prescription data, not on claims data or on data on drugs dispensed over the counter. Although they do not capture the over-the-counter drug consumption or perfectly document adherence to prescribed drug regimens, these prescription data reflect the actual practice of French and Italian GPs [23]. Although we selected antibiotics typically indicated for respiratory tract infections, their prescription may have also been for reasons other than asthma exacerbation. We were unable to assess severity factors not readily available (such as socioeconomic factors or spirometry) or unreliable (such as smoking status) [24]. Because the derived HEDIS criteria are partly based on drug prescriptions to identify patients with persistent asthma, we may have underestimated the proportion of asthmatic patients in the GPs’ lists and the frequency of non-asthma-specific drug prescriptions [25]. We used as outcome criteria the prescription of at least one box of drug rather than the defined daily dose because the aim of the study was primarily to measure the frequency of prescription of antibiotics and anxiolytics/hypnotics.
Antibiotic prescription
When presented with an asthma exacerbation, GPs are likely to overestimate the risk of bacterial infection and prescribe antibiotics [26,27]. This trend is associated with the underuse of inhaled corticosteroids, probably because of a misunderstanding of the immunosuppressive effect of corticosteroids [28]. However, antibiotics are frequently not useful in asthma exacerbations (for those caused by viral infections, for example), unless they are of bacterial origin or are associated with bacterial acute sinusitis in children [1,29]. A computed tomography scan is recommended for confirmation when sinusitis is suspected in adult patients [1]. However, because the clinical features of sinusitis lack diagnostic precision [30,31], GPs can face delays in getting access to a computed tomography scan for their patients and may prescribe antibiotics as a precautionary measure [32]. Independently, evidence is lacking on the actual value of the use of antibiotics, such as macrolide treatment for at least 4 weeks, in the treatment of chronic asthma [33]. The over-prescription of antibiotics to asthmatic patients may cause adverse events, increase costs, and contribute to the development of antibiotic resistance in microbes [17]. Interestingly, antibiotic use in the first year of life is a risk factor for asthma [34].
France and Italy belong to the group of European countries with a high level of antibiotic consumption (17–24 daily doses per day per 1000 inhabitants); France is currently ranked second and Italy third, behind Greece [35]. The small difference that we observed in the numbers of antibiotic prescriptions between France and Italy may be because such prescriptions are specific for respiratory tract infections. Our results confirm that women are prescribed more antibiotics than men [36,37], which may be owing to poorer control of their asthma, among possible reasons [3].
Anxiolytic and hypnotic prescriptions
Our estimation of the frequency of prescription of anxiolytics or hypnotics in French asthmatic patients (17.8 %) is consistent with observations from the available dispensing data (25.6% for anxiolytics and 13.0% for hypnotics) [26]. In Italy, we observed less frequent prescription of drugs in this category (6.9%) compared with France. A possible explanation for this finding is that patients must pay for all benzodiazepine prescriptions [38]. Thus, a GP may preferentially prescribe other reimbursable drugs. The high prevalence of anxiety disorders and insomnia in France, especially in older people, may explain the high numbers of prescriptions for anxiolytics and hypnotics [39]. More specifically, these prescriptions may be related to poor asthma control [3,40-42]. This relationship could be interpreted in two ways: asthma exacerbation could induce anxiety [43] or psychiatric disorders could be risk factors for asthma exacerbations [44].
There are guidelines that promote the provision of psychological support to asthmatic patients and that recommend the limited prescription of psychotropic drugs [31]. The long-term use of anxiolytics and hypnotics should be avoided because of their addictive effect [45], and their use should be avoided during asthma exacerbations because of their respiratory depressant effects, which are potentially lethal [44]. Although cognitive-behavioural therapies focussed on worry proneness and the overvaluation of worry and uncertainty may be as effective as drug treatment and may be more durable for treating anxiety disorders [46], these results remain to be confirmed in asthmatic patients [47].
In Europe and North America, women are generally prescribed twice as many psychotropic drugs as men [48]. Psychiatric disorders and complaints are indeed more common in women than in men [49]. Women are also exposed to specific situations such as pregnancy, which can both worsen asthma and generate anxiety [26,50]. In addition, women have fewer opportunities than men to control symptoms of anxiety through social activities outside the home, including the use of alcohol [51-53].
Implications for research, policy and practice
The high prevalence of antibiotic prescription in asthmatic patients suggests a likely antibiotic over-prescription in France and Italy. While anxiety is frequent in asthmatic patients, the prescription of anxiolytics and hypnotics should be avoided and the use of non-pharmacological interventions should be considered in these patients. Apart from international guidelines, there is only one French guideline from 2004 on long-term asthma management. The French guideline does not mention the prescription of antibiotics and anxiolytics/hypnotics, and there are no specific Italian recommendations on asthma management.
Conclusions
While it is known that many asthmatic patients do not take specific controllers, the prescription of non-asthma-specific drugs is common, especially in women. Asthmatic patients often have additional health and life concerns. GPs should use safe interventions and take a biopsychosocial perspective. The prescription of antibiotics and anxiolytics/hypnotics to asthmatic patients should follow the same rules that apply to their prescription in non-asthmatic patients. Asthma guidelines should address this issue and refer to other guidelines covering the prescription of these drugs. Alternative non-pharmacological interventions should be considered.
Abbreviations
- aOR:
-
Adjusted odds ratios
- ATC:
-
Anatomical Therapeutic Chemical classification
- GP:
-
General practitioner
- HEDIS:
-
Health Employer Data and Information Set
References
GINA report, global strategy for asthma management and prevention. updated 2012. Available from: http://www.ginasthma.org. (last access 02/05/13).
Rabe KF, Adachi M, Lai CKW, Soriano JB, Vermeire P, Weiss KB, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys. J Allergy Clin Immunol. 2004;114:40–7.
Demoly P, Annunziata K, Gubba E, Adamek L. Repeated cross-sectional survey of patient-reported asthma control in Europe in the past 5 years. Eur Respir Rev. 2012;21:66–74.
Lagerløv P, Veninga CCM, Muskova M, Sta C. Asthma management in five European countries: doctors’ knowledge, attitudes and prescribing behaviour. Eur Respir J. 2000;15:25–9.
Van Ganse E, Antonicelli L, Zhang Q, Laforest L, Yin DD, Nocea G, et al. Asthma-related resource use and cost by GINA classification of severity in three European countries. Respir Med. 2006;100:140–7.
Glauber JH, Fuhlbrigge AL, Finkelstein JA, Homer CJ, Weiss ST. Relationship between asthma medication and antibiotic use. Chest. 2001;120:1485–92.
Wahlström R, Hummers-Pradier E, Lundborg CS, Muskova M, Lagerløv P, Denig P, et al. Variations in asthma treatment in five European countries–judgement analysis of case simulations. Fam Pr. 2002;19:452–60.
Ohayon MM, Lader MH. Use of psychotropic medication in the general population of France, Germany, Italy, and the United Kingdom. J Clin Psychiatry. 2002;63:817–25.
Goossens H, Ferech M, Vander Stichele R, Elseviers M. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365:579–87.
Costelloe C, Metcalfe C, Lovering A, Mant D, Hay ADA. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096.
Weich S, Pearce H, Croft P, Singh S. Effect of anxiolytic and hypnotic drug prescriptions on mortality hazards: retrospective cohort study. BMJ. 2014;1996(March):1–12.
Conseil national de l’ordre des médecins: ATLAS DE LA DÉMOGRAPHIE MÉDICALE EN FRANCE. 2014.
Sanità e salute 2012. Available from: http://www3.istat.it/dati/catalogo/20111216_00/PDF/cap3.pdf. (last access 01/08/14).
Bouée S, Charlemagne A, Fagnani F, Le Jeunne P, Sermet C, Naudin F, et al. Changes in osteoarthritis management by general practitioners in the COX2-inhibitor era-concomitant gastroprotective therapy. Joint Bone Spine. 2004;71:214–20.
Mazzaglia G, Yurgin N, Boye KS, Trifir G, Allen E, Filippi A, et al. Prevalence and antihyperglycemic prescribing trends for patients with type 2 diabetes in Italy : A 4-year retrospective study from national primary care data. Pharmacol Res. 2008;57:358–63.
Cricelli C, Mazzaglia G, Samani F, Marchi M, Sabatini A, Nardi R, et al. Prevalence estimates for chronic diseases in Italy: exploring the differences between self-report and primary care databases. J Public Health (Bangkok). 2003;25:254–7.
Laforest L, Pacheco Y, Bousquet J, Kocevar VS, Yin D, Van Ganse E. How appropriate is asthma therapy in general practice? Fundam Clin Pharmacol. 2005;19:107–15.
CEGEDIM strategic data Scientific Publications Bibliography. Available from: www.cegedimstrategicdata.com. (last access 05/05/14).
WHO Collaborating Centre for Drug Statistics Methodology, Guidelines for ATC classification and DDD assignment 2010. 13th ed. Oslo: WHO; 2009
Jones-Vessey K. Using HEDIS Measures to Evaluate Medicaid Managed Care Organization Performance: The Treatment of Persistent Asthma in the Pediatric Medicaid. Raleigh: Center for Health Informatics and Statistics; 2001
Blais L, Lemière C, Menzies D, Berbiche D. Validity of asthma diagnoses recorded in the Medical Services database of Quebec. Pharmacoepidemiol Drug Saf. 2006;15:245–52.
Ovhed I, van Royen P, Håkansson A, HAKANSSON A. What is the future of primary care research? Scand J Prim Heal Care. 2005;23:248–53.
Van Weel C, de Grauw W. Family practices registration networks contributed to primary care research. J Clin Epidemiol. 2006;59:779–83.
McGinnis KA, Brandt CA, Skanderson M, Justice AC, Shahrir S, Butt AA, et al. Validating smoking data from the Veteran’s Affairs Health Factors dataset, an electronic data source. Nicotine Tob Res. 2011;13:1233–9.
Afrite A, Allonier C, Com-ruelle L, Le GN. L’asthme en France en 2006: prévalence et contrôle des symptômes. Quest d’économie la santé. 2008;138:1–8.
Laforest L, Van Ganse E, Devouassoux G, Osman LM, Pison C, El Hasnaoui A, et al. Factors influencing dispensing of psychotropic medications to patients with asthma: a community pharmacy-based survey. Ann Allergy Asthma Immunol. 2008;100:230–6.
Heckerling PS. Clinical Prediction Rule for Pulmonary Infiltrates. Ann Intern Med. 1990;113:664.
Cicutto LC, Llewellyn-Thomas HA, Geerts WH. The management of asthma: a case-scenario-based survey of family physicians and pulmonary specialists. J Asthma. 2009;37:235–46.
Morris PS, Leach AJ. Antibiotics for persistent nasal discharge (rhinosinusitis) in children. Cochrane Database Syst Rev. 2008;2:CD001094.
Rossi OV, Pirilä T, Laitinen J, Huhti E. Sinus aspirates and radiographic abnormalities in severe attacks of asthma. Int Arch Allergy Immunol. 1994;103:209–13.
Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31:143–78.
Lindbaek M, Butler C. Antibiotics for sinusitis-like symptoms in primary care. Lancet. 2008;371:874–6.
Richeldi L, Ferrara G, Fabbri LM, Lasserson TJ, Gibson PG. Macrolides for chronic asthma. Cochrane Database Syst Rev. 2005;4:CD002997.
Kozyrskyj AL, Ernst P, Becker AB. Increased risk of childhood asthma from antibiotic use in early life. Chest. 2007;131:1753–9.
Muller A, Coenen S, Monnet DL, Goossens H. European Surveillance of Antimicrobial Consumption (ESAC): outpatient antibiotic use in Europe, 1998–2005. Euro Surveill. 2007;12:E071011.1.
Pan A, Buttazzi R, Marchi M, Gagliotti C, Resi D, Moro ML. Secular trends in antibiotic consumption in the adult population in Emilia-Romagna, Italy, 2003–2009. Clin Microbiol Infect. 2011;17:1698–703.
Cavalié P. Évolution 2000–2010 de la consommation d ’antibiotiques en France. BEH. 2012;42-43:0–4.
Bellantuono C, Fiorio R, Williams P, Martini N, Boaaini L, Bozzini L. Psychotropic drug monitoring in general practice in Italy: a two-year study. Fam Pr. 1987;4:41–9.
Lépine J-P, Gasquet I, Kovess V, Arbabzadeh-Bouchez S, Nègre-Pagès L, Nachbaur G, et al. [Prevalence and comorbidity of psychiatric disorders in the French general population]. Encéphale. 2005;31:182–94.
Lavoie KL, Bacon SL, Barone S, Cartier A, Ditto B, Labrecque M. What is worse for asthma control and quality of life: depressive disorders, anxiety disorders, or both? Chest. 2006;130:1039–47.
Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113:59–65.
Karlstad Ø, Tverdal A. A prospective study of asthma and subsequent use of hypnotics in young adults. Pharmacoepidemiol Drug Saf. 2011;20:370–7.
Ampon R, Williamson M, Correll P, Marks G. Impact of asthma on self-reported health status and quality of life: a population based study of Australians aged 18–64. Thorax. 2005;60:735–9.
Joseph KS, Blais L, Ernst P, Suissa S. Increased morbidity and mortality related to asthma among asthmatic patients who use major tranquillisers. BMJ. 1996;312:79–82.
O’brien CP. Benzodiazepine use, abuse, and dependence. J Clin Psychiatry. 2005;66 Suppl 2:28–33.
Hunot V, Churchill R, Silva de Lima M, Teixeira V. Psychological therapies for generalised anxiety disorder. Cochrane Database Syst Rev. 2007;24(1):CD001848.
Yorke J, Fleming SL, Shuldham C. Psychological interventions for adults with asthma: a systematic review. Respir Med. 2007;101:1–14.
Alonso J, Angermeyer MC, Bernert S, Bruffaerts R, Brugha TS, Bryson H, et al. Psychotropic drug utilization in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl. 2004;420:55–64.
Astbury J. Gender Disparities in Mental Health. Geneva, Switzerland: WHO; 2001.
Barron W, Leff A. Asthma in pregnancy. Am Rev Respir Dis. 1993;147:510–1.
Ashton H. Psychotropic-drug prescribing for women. Br J Psychiatry Suppl. 1991;10:30–5.
Swartz M, Landerman R, George LK, Melville ML, Blazer D, Smith K. Benzodiazepine anti-anxiety agents: prevalence and correlates of use in a southern community. Am J Public Heal. 1991;81:592–6.
Araya R, Rojas G, Fritsch R, Acuña J, Lewis G. Common mental disorders in Santiago, Chile: prevalence and socio-demographic correlates. Br J Psychiatry. 2001;178:228–33.
Acknowledgements
We thank Marie Sophie Schwalm for her support and Cegedim Strategic Data for allowing the use of their data.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
EVG reports a non-conditional grant from Cegedim Strategic Data and consultancy fees from Danone, ALK, and ABELLO, and expertise fees from UCB, grants from IMS, personal fees from Boehringer Ingelheim. CVW reports grants from Boehringer Ingelheim, personal fees from Novartis, and grants from GSK. DD, LLa, FP and LLe report no conflicts of interest.
Authors’ contributions
DD, LLa, EVG and LLe had the original idea for the manuscript. DD and LLa contributed to the statistical analysis. DD and LLe drafted the manuscript, which was reviewed and approved by DD, LLa, EVG, FP, CVW and LLe.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Darmon, D., Laforest, L., Van Ganse, E. et al. Prescription of antibiotics and anxiolytics/hypnotics to asthmatic patients in general practice: a cross-sectional study based on French and Italian prescribing data. BMC Fam Pract 16, 14 (2015). https://doi.org/10.1186/s12875-015-0222-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12875-015-0222-0