
Abstract
Children from substance-affected families show an elevated risk for developing own substance-related or other mental disorders. Therefore, they are an important target group for preventive efforts. So far, such programs for children of substance-involved parents have not been reviewed together. We conducted a comprehensive systematic review to identify and summarize evaluations of selective preventive interventions in childhood and adolescence targeted at this specific group. From the overall search result of 375 articles, 339 were excluded, 36 full texts were reviewed. From these, nine eligible programs documented in 13 studies were identified comprising four school-based interventions (study 1–6), one community-based intervention (study 7–8), and four family-based interventions (study 9–13). Studies’ levels of evidence were rated in accordance with the Scottish Intercollegiate Guidelines Network (SIGN) methodology, and their quality was ranked according to a score adapted from the area of meta-analytic family therapy research and consisting of 15 study design quality criteria. Studies varied in program format, structure, content, and participants. They also varied in outcome measures, results, and study design quality. We found seven RCT’s, two well designed controlled or quasi-experimental studies, three well-designed descriptive studies, and one qualitative study. There was preliminary evidence for the effectiveness of the programs, especially when their duration was longer than ten weeks and when they involved children’s, parenting, and family skills training components. Outcomes proximal to the intervention, such as program-related knowledge, coping-skills, and family relations, showed better results than more distal outcomes such as self-worth and substance use initiation, the latter due to the comparably young age of participants and sparse longitudinal data. However, because of the small overall number of studies found, all conclusions must remain tentative. More evaluations are needed and their quality must be improved. New research should focus on the differential impact of program components and delivery mechanisms. It should also explore long-term effects on children substance use, delinquency, mental health, physical health and school performance. To broaden the field, new approaches to prevention should be tested in diverse cultural and contextual settings.
Similar content being viewed by others
Background
Substance misuse and dependency severely impact physical and mental health. They are often accompanied by comorbid mental disorders and behavioral problems, especially when consumption begins early in life [1, 2]. Increasing rates of adolescents’ legal and illicit substance use across industrialized countries in recent years [3], as well as risky consumption patterns in European and American youth [4–6], have elevated community concerns. Diverse prevention efforts have resulted from these concerns under which universal prevention approaches still remain the most common. By intervening early in life, these efforts aim at turning developmental pathways away from substance use problems and the danger of their developing into substance use disorders (SUDs) [7]. There is considerable research evidence for the effectiveness of substance abuse prevention programs. They appear to be strongest when they draw on social influence concepts, when they target high-risk groups early, for example from disadvantaged community areas [8], and when they are family-focused [9–11]. Effect sizes are small for universal youth-only substance abuse prevention programs. For selective and indicated family-focused prevention interventions, up to nine times greater effect sizes have been documented [12–17]. To increase the impact of drug prevention, universal prevention needs to be supplemented by more specific prevention programs geared to the needs of different populations at risk for developing a problematic use of substances.
The negative impact of parental drug use has been documented by a multitude of studies and reviews, especially for children of alcoholics. It includes physical, psychological, and cognitive consequences for children’s development [18–20]. Children and adolescents affected by parental drug use show higher rates of externalizing and internalizing problems such as antisocial behavior, emotional problems, attention deficits, or social isolation [21]. With regard to substance use problems, their records more often show an early onset of substance consumption [22, 23], earlier drunkenness experiences [24], increased binge drinking rates [25], and an elevated risk for developing substance use disorders at a younger age than comparable peers [26]. Approximately 33 to 40 percent of all children with a substance using parent will develop a substance use disorder themselves [27, 28].
Substance problems are transmitted to the next generation via several pathways, especially genetic disposition [29, 30], behavioral, and cognitive processes [31, 32]. Family environmental characteristics such as problematic family relationships [21], family conflict, or absence of supportive parenting [33] play an important part in transmitting substance use problems to offspring. The same goes for positive expectations about the effects of substance consumption acquired in familial context [34, 35]. Learning from the model substance-dependent parents set, children learn to use substances as coping strategies in stressful and difficult times [36–38]. Family environment can also be a significant resource. Family attachment or bonding, monitoring, and communication of positive family values and expectations are strong protective factors in preventing substance use and abuse [9]. Recent epigenetic animal research on the role of the prenatal and postnatal environment on expression of inherited diseases such as substance use disorders suggests that one of the most protective factors is nurturing parenting [39–41].
These findings have led practitioners and researchers to target children of substance using parents with family-focused prevention interventions that increase supportive and nurturing parenting. These family interventions are expected to reduce the risk for later substance abuse, and, consequently, the high societal costs of delinquency, mental and physical disorders, and child maltreatment [9–11]. Considering the research mentioned above, they seem more promising than interventions targeting only parents or only children. However, in the case of substance-affected families, parents frequently are not willing to participate in such a program. Nevertheless, they may endorse the benefits their children receive from a prevention program. Resilience theory and research [42, 43] demonstrate that children’s development is influenced by their own cognitive appraisal of a life with a substance-abusing parent as well as by their emotional and behavioral strategies of coping with difficult situations arising from parental substance use. Consequently, interventions enhancing these skills in children seem a further promising prevention form. They mainly focus on children aged 8–12 years since these children are old enough for cognitive teaching strategies while not yet in puberty where own substance consumption problems commence. Child-focused programs are frequently delivered in a peer-group format, for instance in a school setting, [17, 44, 45] so children can benefit from positive peer influence and mutual support.
While there is considerable evidence for the effectiveness of universal prevention programs [46–48], the field is only just evolving in relation to selective prevention programs for children of substance abusers. To date, programs specifically geared to this high-risk population have not yet been reviewed together, even though some of them have been mentioned in more general systematic reviews on the (universal) prevention of tobacco, alcohol, and drugs [12, 14, 49, 50]. One article reviews prevention for children of parents who abuse only alcohol [8], while another targets children of illicit drug users [51]. Woolfall and Sumnall [52] as well as Kumpfer [53] focus on outcome measures in evaluating interventions for children of substance using parents, but do not analyze the interventions. Barnard and McKeganey [54] review key evaluated interventions for families with SUD problems and conclude that interventions focusing directly on children’s needs are important but scarce. The aim of this paper is to gather the evidence on prevention programs designed specifically for children with a substance using parent.
We choose a systematic review approach because a meta-analytic strategy does not seem appropriate considering the small body of research and its heterogeneous designs. We focus on child outcomes, such as child functioning or child substance use, and on family attributes that, by definition, include child outcomes such as family cohesion. We also compare the interventions described in the studies with regard to similarities and differences and review the design quality of the studies. In the following, we describe our approach and methods. Then we present an overview of the relevant programs, their contents and their evaluation. The corresponding studies are rated according to their evidence level and design quality. In the subsequent discussion we integrate the results of the review based on the aspects mentioned above and draw conclusions for research and practice.
Methods
Identification of studies and inclusion criteria
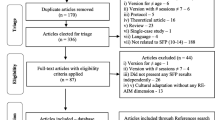
Our methodology was guided by guidelines for current systematic literature reviews [55, 56]. All studies describing or investigating validly established effects of preventive interventions on children and adolescents with substance abusing parents (or on affected families as a whole entity) were included in the review. We searched for relevant studies published during the period of 1994–2009, thus choosing a time span of 15 years. This is broad enough to incorporate a larger number of studies than the more common 10-year-span, but not too broad to ensure the comparability of the scientific methodology used in the studies. Using the search terms “prevention AND child* AND (parents AND (addict* OR alcohol))” delivered the most results. We used this combination to search the following databases: Cochrane database of systematic reviews, Ovid, MEDLINE(R), EMBASE, PsycINFO and PSYNDEXplus. The age of the target population ranged from 0–17 years, and only English or German literature was included. After removing duplicates our initial search on January 2, 2010, generated 348 articles. Of these, nine articles were identified as potentially relevant, and full texts were obtained. 339 articles were excluded because they did not deal with prevention programs specifically for children of substance using parents or affected families. Their topics can be summarized as follows: addiction and violence (12 articles), programs for substance using parents (5 articles), effects of parental addiction on children (37 articles), predicting SUD development (58 articles), addiction prevention in general (84 articles), alcohol in general (24 articles), other topics (119 articles). In addition to the search described above, an extensive hand search was conducted in public search engines (using keywords, program and researcher names) and by screening the references of the full texts. This yielded additional 27 articles, resulting in a total number of 36 potential articles to be included. The articles were examined by two independent reviewers (Katja Kruse and Gurli Herrmann) according to the following inclusion criteria:
Evidence-based outcome
All studies describing or investigating validly established effects of prevention programs on the target group considered here were included. Thus, a text was excluded if only program characteristics are described, but no empirical evidence is reported, or if case histories, case studies, or a single-case study are used as evidence for the effectiveness of the program.
Publication characteristics
The study is published in a peer-reviewed national or international scientific journal.
Age of child / children
The program is targeted at children and/or adolescents aged 0–17 years or at families with children of this age.
Substance consumption of parent(s)
At least one parent or legal guardian uses alcohol and/or other psychotropic substances (legal or illegal) in a risky or problematic way, or is dependent on at least one substance. Therefore, an article was excluded if the described program belongs to the category of universal prevention programs (e.g., whole school-class), or selective prevention programs for a more unspecific risk-group (e.g., whole school-class from inner-city setting). Regarding parental consumption, a DSM- or ICD-diagnosis was not required so as not to further diminish the few relevant studies identified. Thus, parental consumption was operationalized differently in the various studies and could be assessed via self-report (questionnaire, interview) of children, parents, or by report of third parties, such as teachers, therapists, or medical practitioners.
Type of intervention
The intervention is preventive and targets children and/or adolescents from substance-using homes. Thus, articles were excluded when programs described therein were classified as indicated prevention programs (e.g., when children and/or adolescents were already showing harmful substance use) or as therapeutic interventions (e.g., for children with mental problems diagnosed according to child and adolescent psychiatric standards; for information on different prevention forms see [49]).
Differences between reviewers were resolved by consensus. They occurred when studies were ambiguous about inclusion criteria (e.g., age-group of the children) or when their methodology seemed disputable. When there was doubt, and in view of the small number of relevant texts, the study was included. At the end of the review process 13 studies evaluating nine programs met our inclusion criteria (see Figure 1 for an overview of the selection process).

Study selection process.
Quality criteria
The studies’ levels of evidence were rated according to the methodology for grading recommendations in evidence-based guidelines of the Scottish Intercollegiate Guidelines Network (SIGN), ranging from Ia to IV [57, 58] see Table 1. This system is internationally accepted and used by guideline developers. The Society for Prevention Research[59] as well as Kumpfer and Alvarado [47] have published similar rating scales that include a even higher level of evidence of effectiveness specifying evidence from multiple randomized, controlled trials (RCTs) that include independent research teams and criteria for the quality of the research. In our case, however, the older version of the SIGN classification system was used, as it seemed better suited to distinguish between studies with comparably low overall quality levels. It contains four levels of evidence that are further differentiated into sub-levels, as shown in Table 1.
Since only a small number of adequate studies matched our inclusion criteria we included not only RCTs but also studies with lower levels of evidence. To quantify the quality of the included studies more precisely within the SIGN categories and to enable a ranking list of the studies, a methodology quality score (MQS) was applied that we adapted to our subject matter from a score used in the area of meta-analytic family therapy research [60, 61]. With this score we examined and rated studies according to 15 criteria of study design quality (see Table 2). The total score rates the design quality of a study as “low” (score 0–14), “modest” (score 14.5-19), “good” (score 19.5-24) or “very good” (score 24.5-30).
Effect Sizes
Effect sizes (ES) were computed in terms of (unweighted) correlation r. Using Fisher’s Z-transformation weighted mean correlations r(+) were also computed [62]. This could only be done in studies supplying appropriate data.
Results
Our search yielded 13 studies [63–75] with nine programs designed specifically for children of substance abusing parents., comprising four school-based interventions (study 1–6), one community-based intervention (study 7–8), and four family-based interventions (study 9–13). Some further studies were consulted for further information on the program or study [76–80]. With the exception of one program conducted in Spain Family Competence Programme (FCP)] [63] and another one with partial sampling in Canada [64] (both of these programs being culturally adapted versions of Kumpfer’s Strengthening Families Program with Kumpfer as a co-investigator), all programs and their evaluation were conducted in the United States. For an overview on program format, structure, content and participants, see Table 3. For an aggregated overview and effect sizes, see Table 4. For an overview on outcome measures, results and study design quality, see Table 5. In the following, we describe our results using the following approach: first, studies are compared with regard to their design quality. Second, program settings and structure are summarized. Third, study measures, findings, and effect sizes are summarized.
Study design quality
Study evidence levels differed in the studies examined here: We found seven RCT’s (Ia/Ib;1/2/3/5/9/10/11), two well designed controlled or quasi-experimential studies (IIa/IIb; 12/13), three well-designed descriptive studies (III; 4/6/7) and one qualitative study (IV; 8). Sample sizes ranged from N = 12 to N = 280. The methodological quality of the studies as rated with the MQS appears quite heterogeneous, with a substantial percentage of very good (1/9/10) or good design quality (2/3/5/11/12), some modest quality designs (7/13), and some studies of low quality (4/6/8). Limitations of the existing body of research are discussed below with regard to future research needs.
Program settings and structure
Most programs for children from substance-affected homes identified and reviewed in this article were school-based, two were family-based, and one was community-based. Intervention duration and intensity did not vary much. Most programs lasted between 8 and 14 weeks with weekly sessions of approximately 90 minutes. Group sizes were not always reported and usually ranged from 8 to 12 children. Only the community-based intervention (7/8), originally designed for ten weeks, lasted for two years on participants’ request. Program content did vary, but common themes for most of the programs emerged, such as coping with emotions, problem solving, education on drugs and addiction, family relations. Didactics usually included theory and practical exercises, discussion, role-play, and video material in some cases. Some programs pointed out structure and fixed rituals as especially important for the target group at hand. Few programs included several components. One intervention (5/6) included a peer mentoring program and homework assistance (the latter of which was not evaluated). The community-based intervention (7/8) included motivational leisure activities and offered family-based crisis intervention. One family-based program (9/10) combined parent and family sessions with home-based case management. Periodical buffer calls lasted for nine months after the intervention. The family-based programs stemming from the SFP (11/12/13) included a dinner break for participating families, but no further components.
In the school-based programs, parents (substance using parent or his/her spouse) were in no way involved in the program, other than giving their consent for participation of the children. They were also not included in data collection and therefore did not assess children’s behaviors, adjustment or problems, thus creating a possible bias regarding study results. In the community-based program, home-based case management was offered, but it remains unclear as to how extensively it was made use of, so that here too, parental involvement cannot be assumed. Family-based programs differed in the attention given to children, parents, and family sessions. One program for families with a methadone-treated parent (9/10) focused primarily on strengthening the adults in their role as parents and in preventing relapses. There were no sessions solely for the children; about a third of all sessions were conducted as family sessions. The SFP modifications (11/12/13) for families with parents addicted to different substances involved parents and children in joint, but also in separate sessions, parents and children receiving the same amount of time. Hence, individual needs could be accounted for, but the family also was recognized as an entity, and individual developments could be brought together and integrated.
Study measures and findings
The most frequent outcome measures were knowledge, self-worth, coping, and social behavior. Further attributes such as emotion regulation, depression, health behaviors, substance use, school attachment and performance, family and/or social relationships were also included. All of these outcome measures address parameters known to increase the risk for developing mental disorders [81]. Only two studies considered possible substance use of participating children (7/10). As listed in Table 4, unweighted effect sizes within the studies vary from r = .70 for knowledge (study 12) to r = .11 for social behavior (study 11). Weighted ES are r (+) = .55 for knowledge, .34 for coping, .27 for family functioning, and .17 for social behavior (not given in Table 4). Overall, the small amount of eligible studies as well as the heterogeneity of study designs, quality and programs allow nothing more than the following preliminary synthesis of findings:
-
(a)
Own reduction of substance consumption or abstinence was evaluated only in some studies, although almost all studies stated this as their ultimate preventive goal. In one study with good design quality (3), no reduction of substance consumption was found for the experimental groups, whereas the control groups’ consumption increased. In another program (7) with modest design quality evaluation the experimental group even showed a higher frequency of alcohol consumption. In the only long-term study (10) of a family-based program substance consumption was elevated in both study groups (intervention and control group) compared to other population samples, and the risk for developing SUD in adolescence or young adulthood was significantly reduced for males, but elevated for females. (b) An improvement in coping strategies was a central part of almost all studied programs, with the exception of one (9/10). Frequently, an improvement was observed. In one study with good design quality (3), only girls showed better coping strategies. (c) Social behavior was also frequently assessed and showed significant improvements in all studies, especially for family-based programs, but also otherwise. (d) Self-worth enhancement was assessed in four programs with inconsistent findings. One study with good design quality found improvement of self-worth (5), but only for a group that received additional training as mentors (not as mentees). A study with poorer design quality reported increase of self-worth, but the duration of the program was over two years, i.e. untypically long (7/8). Two further high quality studies did not reveal significant effects on self-worth (1/2). (e) Program-related knowledge such as facts about alcohol, drugs, addiction, and their effects on families was assessed in five of the studies (1/3/4/6/12) and increased substantially in all cases.
-
(f)
Unexpected findings / negative effects also occurred: positive alcohol expectations rose in one study (1) with very good design quality, even though the intended effect was the opposite. In the same study no outcome differences between groups with or without individual trainer component were found. This finding contrasts with another study, also with good design quality, in which positive effects of mentorship were reported (5). Also, high levels of loneliness and isolation were found at pre-test measurement in one study (2) with good design quality, which did not change after the 8-week program. In another study of low quality (6) that featured 11 sessions plus a mentorship component participants did report decreased levels of isolation. In a further study (3; good design quality) there were other unexpected findings such as increased medical complaints and diminished social integration for boys. In one program (5; good design quality), positive effects were also reported for the wait control groups, while this was either not the case or not reported in other programs.
In our review, we frequently find two studies focusing on the same program. Results could be interpreted more definitely if they were repeated in programs implemented several times. However, this is not the case in the studies examined here: In almost all cases, we find additional or follow-up information on only one program implementation (3/4, 7/8, 9/10). Only one program was implemented twice (5/6), but with very different sample sizes and different results, the only repeated result being school performance.
Discussion
The existing body of research on prevention programs for children in substance-affected families was reviewed, and some key points can be highlighted. While some school-based studies showed many effects, others did not, and while one family program showed very little effect (9/10), the SFP adaptations showed good results (11–13). A fairly homogeneous finding is the substantial increase in program-related knowledge in all studies that included this outcome measure. The weighted ES for knowledge was large with r(+) = .55. This demonstrates the effectiveness of psycho-educative program components. Self-worth was rarely enhanced by the programs with the exception of participants in an intervention that had received additional mentor training (5). The fact that only a multi-component group and a very long-term program (SFP) had any effects in this area indicates that self-worth may be an attribute of trait quality, and, therefore, not easy to improve. It is subject to many influences and long-term developments that are deeply rooted in identity issues. This seems to be different for coping strategies which improved frequently. The weighted ES for coping was medium sized with r(+) = .34. However, in one study with good design quality (3), only girls showed better coping strategies, an effect that the researchers attribute to the age group of the study (M = 15.5 years) in which girls may be more mature for developmental reasons. Further research on the interplay of age, gender and program effects is needed to explore differential aspects in tapping the coping resources of these children.
The frequent findings on improvement of social behavior are rendered somewhat inconclusive by the fact that no study described baseline social behavior levels. On the other hand, it is made more credible by the fact that social behavior improvements were not only reported by the children themselves, but also by parents and/or teachers. The weighted ES for social behavior was small with r(+) = .17. One possible reason for the lack of statistically significant reductions in substance use may be that many of these studies were conducted with children younger than 12 years of age. A majority of them probably were not consuming substances at this point. Longitudinal studies examining the development of own substance use at a later point in children’s development were rarely funded in the past. On the whole, the effect of preventive programs for children of substance-affected families on their own problems with substances remains unclear and merits more longitudinal research.
Over all studies providing appropriate data (see Table 4), and assuming homogeneity in overall outcome, ES would be r(+) = .33 or d(+) = .70, meaning that any randomly chosen child in the treatment conditions had a 69% probability to benefit from the prevention program. From this, we conclude that even though some study results seem promising, evidence is still too mixed for definite conclusions on “what worked best”. This is especially true for school-based programs. For instance, unexpected effects occurred such as the elevation of positive alcohol expectancies (1), or the increase of health complaints and decrease of social integration for boys (3). In other studies, negative findings were not mentioned – it is unclear whether they occurred or not. Even though some explanations are offered for negative effects authors generally made no suggestions how to deal with these effects. Future research should attempt to discuss such findings in the light of possible modifications of programming, recruiting or study design. Editors and funders should require reports on adverse events and findings. The success of short intervention programs may rest on the emphasis placed on tailoring programs to the needs of their target group, for instance, to age, gender, or cultural background. Programs that contained components over a longer period of time (i. e. over half a year or longer) produced superior effects compared with shorter interventions. Therefore we tentatively conclude that SMAAP (1) and CHOICES (5/6) were the programs with the best evidenced effects, and that CHOICES is superior to SMAAP because of its multi-component approach and long-term components. Teen-Club (7/8) also showed positive long-term effects, but the intervention was not well studied.
The success of family-based programs, especially SFP, is clearer and points to the value of integrating both parents and children into programs, wherever possible. This is a disadvantage of school-based programs, where parents hardly participated. On the other hand, recruiting substance-involved parents to participate in a program of this kind can be extremely difficult, so that low-threshold interventions remain necessary. Special “success factors“ in a family setting appear to be a focus on the family level, not only the individual level, and a broad integrated approach to many kinds of problem behavior. The program that focused more on parent training was less successful. This is in line with the research on parenting described in the Background section and with the conclusions stated by Kumpfer and Alvarado [47] in their reviews of family-based prevention programs. The weighted ES for family functioning was on a medium level with r (+) = .27.
Each of the nine programs except for the community-based one (7/8) was evaluated in at least one very good or at least good quality study. Often large sample sizes were employed and multiple change indices, assessed in different ways, but often with standardized instruments, were employed. This adds credibility to the findings described and synthesized in this article, even though the small study base must be taken into account. The following limitations to the body of research presented here point to conclusions for future research.
(a) Quantity of studies: Only 13 studies of 375 titles (3.5%) were included, representing to our knowledge all of the published work in this area conducted over 15 years of research (1994–2009). Almost no published work from other countries besides the United States exists to date. Clearly more programs and research agendas in different cultural and contextual settings are needed for this high-risk target group in the future. (b)Sample sizes: These varied considerably. They should be based on thorough power analysis to achieve adequate statistical power and enable subgroup analyses. (c) Treatment integrity: Even though most programs had well-trained staff, adherence to the program was often not reported. In some studies research staff also administered the program, which creates a possible bias. Future research should seek to document treatment fidelity in audio- or videotape analysis, not relying on group leader reports alone.
(d) Measurement of effects: The most important independent variable, parental substance use, was often not validated rigorously, but assessed solely by a short screening question or child self-report. A multitude of parameters were assessed, in many cases only by self-report of the children, sometimes by teacher or group-leader report, rarely by parental assessment. As often is the case, participating teachers and parents were not blinded to treatment condition, creating a consistent bias in all of the studies. Even though own substance problem prevention seemed the primary goal in most studies this was rarely assessed directly. Instead, it was assumed that certain indicators (e.g., behavioral problems, family relations, psychosocial adjustment) would indirectly contribute to achieving this goal. Future research should aim at clearly defining treatment goals and using validated instruments already utilized in other studies to enhance study comparability. Multiple perspectives, including parent perspective, should be employed to validate children’s self-reports. (e) Recording adverse events: Adverse events, i.e. adverse changes in health or side effects during program delivery are hardly reported in the literature mentioned here and in other current literature. This is a serious and important omission [82–84]. Documenting adverse events or their absence can uncover possible harm done by delivering the program. For instance, in the case of children from substance-affected families, their being educated about the parental problems without including parents in the intervention could cause serious conflict and hostility within a vulnerable family.
(f) Follow-ups: Most studies relied on pre-post-tests, only some studies conducted follow-ups (1/7/8/9/10), two studies of which were of inferior quality (7/8). These studies showed that effects tended to decrease over time. Nevertheless, it seems likely that in the context of parental substance use and for this age group, program effects may be more long-term, especially regarding own substance consumption status, but also regarding other psychosocial developments. Future research must seek to conduct longitudinal studies to identify possible delay effects as are found in meta-analytical family therapy research [85, 86], or their absence. (g) Component analysis: By employing wait-control lists no program effects were compared to effects of unspecific or different interventions. Therefore almost no study focused on which component was important for producing desired effects. Only study (5) compared effects of different components and found that participants receiving two instead of one component showed better results. A next generation of research must identify success factors in programs, i.e. effective program ingredients, to enhance efficiency and effectiveness of preventive interventions for children of substance abusing parents.
Conclusions
All forms of intervention, i.e., school-based, community-based, and family-based interventions, showed valuable results, but these are found in a very small number of program evaluation studies. Thus, while there is evidence for programs’ effectiveness in reducing high-risk children’s problems and improving positive behaviors, coping skills, and feelings, it remains preliminary. It is up to future work to broaden the body of research on programs for children from substance-affected families. Next to testing new approaches to prevention, using less expensive implementation methods such as web and DVD-based programs for wider dissemination in different contexts and with different age groups, more work is needed that explores different age groups and settings as well as cultural particularities in different countries. Program developers can draw on best practices identified in the broader area of family-based prevention programs [87]. For the public health system, the mixed results found here also call for investing more in carefully planned program evaluations to better allocate funding to effective programs. Also, more emphasis should be placed on program implementation after the evaluation is finished. This would enable re-testing program effects in more naturalistic settings. Funders should especially consider supporting efforts aimed at identifying long-term effects of prevention programs for children from substance-affected families. The fulfillment of the ultimate program goal, i.e., to reduce intergenerational transmission of SUD and other mental health problems, cannot be determined by any other means than by longitudinal research.
Authors’ information
Most authors of this paper work at the two partner institutes currently conducting a large national trial of a community-based intervention for children from substance-affected families in Germany (http://www.projekt-trampolin.de). For more information on our research, see http://www.dzskj.de, http://www.disup.de.
References
Stolle M, Sack P-M, Thomasius R: Substance abuse in children and adolescents – Early detection and intervention. Dtsch Arztebl. 2007, 104 (28–29): A2061-A2070.
Thomasius R, Jung M, Schulte-Markwort M: Suchtstörungen. Entwicklungspsychiatrie Biopsychologische Grundlagen und die Entwicklung psychischer Störungen [Developmental psychiatry biopsychological foundations and the development of mental disorders]. 2nd (vollständig überarb. und erw.) edition. Edited by: Herpertz-Dahlmann B, Resch F, Schulte-Markwort M, Stuttgart Warnke A. 2008, Schattauer, DE, 885-918.
European Monitoring Centre for Drugs and Drug Addiction: Annual Report 2009: The state of the drug problem. Lisbon, PO: European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). 2009
Friese B, Grube J: Youth drinking rates and problems: A comparison of European countries and the United States. 2010, [http://resources.prev.org/underagedrinking_resources.html], retrieved 29.10.2010, retrieved 29.10.2010
Hibell B, Guttormsson U, Ahlström S, Balakireva O, Bjarnason T, Kokevi A, Stockholm, SW: The 2007 ESPAD Report: substance use among students in 35 European countries. The Swedish Council for Information on Alcohol and Other Drugs (CAN). 2009
Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE: Monitoring the future national survey results on drug use, 1975–2009. Secondary school students (NIH Publication No. 10–7584). I. 2010, Bethesda, MD: National Institute on Drug Abuse
Toumbourou JW, Stockwell T, Neighbors C, Marlatt GA, Sturge J, Rehm J: Interventions to reduce harm associated with adolescent substance use. Lancet. 2007, 369: 1391-1401. 10.1016/S0140-6736(07)60369-9.
Cuijpers P: Prevention programmes for children of problem drinkers: A review. Drugs Educ Prev Pol. 2005, 12 (6): 465-475. 10.1080/09687630500337162.
Kumpfer KL, Alvarado R, Whiteside HO: Family-based interventions for substance abuse prevention. Subst Use Misuse. 2003, 38 (11–13): 1759-1789.
Spoth RL, Redmond C, Shin C: Randomized trial of brief family interventions for general populations: Adolescent substance use outcomes 4 years following baseline. J Consult Clin Psychol. 2001, 69: 627-642.
Spoth RL, Redmond C: Illustrating a framework for rural prevention research. Project family studies of rural family participation and outcomes. Preventing childhood disorders, substance abuse, and delinquency. Edited by: Peters R, McMahon RJ. 1996, Thousand Oaks, CA: Sage Publications, 299-328.
Foxcroft DR, Ireland D, Lister-Sharp DJ, Lowe G, Breen R: Longer-term primary prevention for alcohol misuse in young people: a systematic review. Addiction. 2003, 98: 397-411. 10.1046/j.1360-0443.2003.00355.x.
Foxcroft DR: Alcohol misuse prevention in young people: a rapid review of recent evidence. 2006, Oxford, UK: Oxford Brooks University
Midford R: Drug prevention programmes for young people. Where have we been and where should we be going. 2009, 1-8. Early View
Stolle M, Sack P-M, Stappenbeck J, Thomasius R: Family-based prevention for children and adolescents [Familienbasierte Prävention bei Kindern und Jugendlichen. Das Strengthening Families Program]. Sucht. 2010, 56 (1): 51-60. 10.1024/0939-5911/a000010.
Tobler NS, Kumpfer KL: Meta-analyses of family approaches to substance abuse prevention. 2001, Rockville, MD: Report prepared for CSAP
Tobler NS, Stratton H: Effectiveness of school-based drug prevention programs: A meta-analysis of the research. J Prim Prev. 1997, 18 (1): 71-128. 10.1023/A:1024630205999.
Denton RE, Kampfe CM: The relationship between family variables and adolescent substance abuse: A literature review. Adolescence. 1994, 29: 475-495.
Kilpatrick DG, Acierno R, Saunders B, Resnick HS, Best CL, Schnurr PP: Risk factors for adolescent substance abuse and dependence: Data from a national sample. J Consult Clin Psychol. 2000, 68: 19-30.
Reinherz HZ, Giaconia RM, Carmola Hauf AM, Wasserman MS, Paradis AD: General and specific childhood risk factors for depression and drug disorders by early adulthood. J Am Acad Child Adolesc Psychiatr. 2000, 39: 223-231. 10.1097/00004583-200002000-00023.
Velleman R, Templeton L: Understanding and modifying the impact of parental substance misuse on children. Adv Psychiatr Treat. 2007, 13: 79-89. 10.1192/apt.bp.106.002386.
Alford GS, Jouriles EN, Jackson SC: Differences and similarities in the development of drinking behavior between alcoholic offspring of alcoholics and alcoholic offspring of nonalcoholics. Addict Behav. 1991, 16: 341-347. 10.1016/0306-4603(91)90027-F.
Rothman EF, Edwards EM, Heeren T, Hingson RW: Adverse childhood experiences predict earlier age of drinking onset: results from a representative US sample of current or former drinkers. Pediatrics. 2008, 122 (2): 298-304. 10.1542/peds.2007-3412.
McKenna T, Pickens R: Alcoholic children of alcoholics. J Stud Alcohol. 1981, 42: 1021-1029.
Weitzman ER, Wechsler H: Alcohol abuse and related problems among children of problem drinkers: Findings from a national survey of college alcohol use. J Nerv Ment Dis. 2000, 188 (3): 148-154. 10.1097/00005053-200003000-00004.
Hussong A, Bauer D, Chassin L: Telescoped trajectories from alcohol initiation to disorder in children of alcoholic parents. J Abnorm Psychol. 2008, 117: 63-78.
Sher KJ, Waltzer K, Wood P: Characteristics of children of alcoholics: Putative risk factors, substance use and abuse and psychopathology. J Abnorm Psychol. 1991, 100: 427-448.
Windle M, Searles JS: Children of alcoholics: critical perspectives. 1990, New York: Guilford Press
Wiers RW: Bad expectations? Cognitive and neuropsychological indicators of enhanced risk for alcoholism. 1998, Delft, NL: Eburon P & L
Schuckit MA, Smith TL: An 8-year follow-up of 450 sons of alcoholic and control subjects. Arch Gen Psychiatr. 1996, 53: 202-210. 10.1001/archpsyc.1996.01830030020005.
Petratis J, Flay BR, Miller TQ: Reviewing theories of adolescent substance use: organizing pieces in the puzzle. Psychol Bull. 1995, 117 (1): 67-86.
Gifford E, Humphreys K: The psychological science of addiction. Addiction. 2007, 102: 352-361. 10.1111/j.1360-0443.2006.01706.x.
Kumpfer KL, Hu Q: What makes children resilient and resourceful despite family adversity and trauma in high risk populations. Trauma and Recovery. Edited by: Gow K, Celinski M. Hauppauge, NY: Nova Science Publishers, in press
Barnow S, Stopsack M, Spitzer C, Freyberger HJ: Correlates of alcohol expectancies in adolescence. Z Klin Psychol Psychiatr Psychother. 2007, 36 (1): 1-10. 10.1026/1616-3443.36.1.1.
Brown SA, Tate SR, Vik PW, Haas AL, Aarons GA: Modeling of alcohol use mediates the effect of family history of alcoholism on adolescent alcohol expectancies. Exp Clin Psychopharmacol. 1999, 7 (1): 20-27.
Chassin L, Pitts SC, DeLucia C, Todd M: A longitudinal study of children of alcoholics: Predicting young adult substance use disorders, anxiety, and depression. J Abnorm Psychol. 1999, 108: 106-119.
Ellis DA, Zucker RA, Fitzgerald HE: The role of family influences in development and risk. Alcohol Health Res World. 1997, 21 (3): 218-226.
Otten R, van der Zwaluw CS, van der Vorst H, Engels RCME: Partner effects and bi-directional parent–child effects in family alcohol use. Eur Addiction Res. 2008, 14: 106-112. 10.1159/000113725.
Weaver IC, Cervoni N, Champagne FA, D'Alessio AC, Sharma S, Seckl JR, Dymov S, Szyf M, Meaney MJ: Epigenetic programming by maternal behavior. Nat Neurosci. 2004, 7 (8): 847-854. 10.1038/nn1276.
Champagne F: Epigenetic influences of social interaction across the lifespan. Dev Psychobiol. 2010,http://www.interscience.wiley.com,
Barnes GM, Reifman AS, Farrell MP, Dintcheff BA: The effects of parenting on the development of adolescent alcohol misuse: A six-wave latent growth model. J Marriage and Family. 2000, 62 (1): 175-186. 10.1111/j.1741-3737.2000.00175.x.
Wolin S, Wolin S: Resilience among youth growing up in substance-abusing families. Pediatr Clin N Am. 1995, 42 (2): 415-442.
Velleman R, Templeton L: Alcohol, drugs and the family: results from a long running research programme within the UK. Eur Addict Res. 2003, 9: 103-112. 10.1159/000070978.
Emshoff JG, Price AW: Prevention and intervention strategies with children of alcoholics. Pediatrics. 1999, 103: 1112-1121.
Dies RR, Burghardt K: Group interventions for children of alcoholics. Prevention and treatment in the schools. J Child Adolesc Group Ther. 1991, 1 (3): 219-234. 10.1007/BF00995308.
Nation M, Crusto C, Wandersman A, Kumpfer KL, Seyboldt D, Morrissey-Kane E, Davino K: What works in prevention. Principles of effective prevention programs. Am Psychol. 2003, 58: 433-456.
Kumpfer KL, Alvarado R: Family-strengthening approaches for the prevention of youth problem behaviors. Principles of effective prevention programs. Am Psychol. 2003, 58: 457-465.
Ramey CT, Ramey SL: Early intervention and early experience. Am Psychol. 1998, 53: 109-120.
Cuijpers P: Three decades of drug prevention research. Drugs Educ Prev Pol. 2003, 10: 7-20. 10.1080/0968763021000018900.
Tobler NS, Roona M, Ochshorn P, Marshall D, Streke A, Stackpole K: School-based adolescent drug prevention programs: 1998 meta-analysis. J Prim Prev. 2000, 20 (4): 275-336. 10.1023/A:1021314704811.
Luthar SS, D'Avanzo K, Hites S: Maternal drug abuse versus other psychological disturbances. Resilience and vulnerability. Edited by: Luthar SS. 2005, New York: Cambridge University Press, 104-130.
Woolfall K, Sumnall H: Evaluating interventions for children of substance using parents: A review of outcome measures. Addiction Res Theor. 2010, 18 (3): 326-343. 10.3109/16066350903254767.
Kumpfer KL: Selective prevention interventions: the Strengthening Families Program. Drug abuse prevention through family interventions. Volume 177. Edited by: Ashhery RS, Robertson EB, Kumpfer KL. 1999a, NIDA Research Monograph, 207-
Barnard M, McKegany N: The impact of parental problem drug use on children: what is the problem and what can be done to help?. Addiction. 2004, 99: 552-559. 10.1111/j.1360-0443.2003.00664.x.
Higgins JPT, Green S: Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration. 2011, Available from www.cochrane-handbook.org
Centre for Reviews and Dissemination (CRD): Systematic reviews: CRD’s guidance for undertaking reviews in healthcare. [http://www.york.ac.uk/inst/crd/index_guidance.htm], Centre for Reviews and Dissemination University of York, 2008, Centre for Reviews and Dissemination University of York, 2008
Scottish Intercollegiate Guidelines Network: Methodology Review Group: Report on the review of the method of grading guideline recommendations. 1999, Scottish Intercollegiate Guidelines Network (SIGN), Edinburgh, GB
Harbour R, Miller J: A new system for grading recommendations in evidence based guidelines. Br Med J. 2001, 323: 334-336.
Flay BR, Biglan A, Boruch RF, Gonzalez Castro F, Gottfredson D, Kellam S, Mosciki EK, Schinke S, Valentine JC, Ji P: Standards of evidence: Criteria for efficacy, effectiveness and dissemination. Prev Sci. 2005, 6 (3): 151-175. 10.1007/s11121-005-5553-y.
Gurman AS, Kniskern DP: Research on marital and family therapy: Progress, perspective and prospect. Handbook of psychotherapy and behavior change. Edited by: Garfield SL, Bergin AE. 1978, New York NY: Wiley, 817-901. 2
Stanton MD, Shadish WR: Outcome, attrition and family-couples treatment for drug abuse: A meta-analysis and review of the controlled, comparative studies. Psychol Bull. 1997, 122: 170-191.
Rosenthal R, DiMatteo MR: Meta-analysis: Recent developments in quantitative methods for literature reviews. Annu Rev Psychol. 2001, 52: 59-82. 10.1146/annurev.psych.52.1.59.
Orte C, Touza C, Ballester L, March M: Children of drug-dependent parents: Prevention programme outcomes. Educ Res. 2008, 50 (3): 249-326. 10.1080/00131880802309390.
Maguin E, Safyer T: The impact of a family-based alcohol prevention program on children’s externalizing behavior problems. Alcohol Clin Exp Res. 2003, 27 (72A): 401-
Short JL, Roosa MW, Sandler IN, Ayers TS: Evaluation of a preventive intervention for a self-selected subpopulation of children. Am J Community Psychol. 1995, 23 (2): 223-247. 10.1007/BF02506937.
Dore MM, Nelson-Zlupko L, Kaufmann E: "Friends in Need": designing and implementing a psycho-educational group for school children from drug-involved families. Soc Work. 1999, 44 (2): 179-190. 10.1093/sw/44.2.179.
Gance-Cleveland B: Qualitative evaluation of a school-based support group for adolescents with an addicted parent. Nurs Res. 2004, 53 (6): 379-386. 10.1097/00006199-200411000-00006.
Gance-Cleveland B, Mays MZ: School-based support groups for adolescents with a substance-abusing parent. J Am Psychiatr Nurses Assoc. 2008, 14 (4): 297-309. 10.1177/1078390308321223.
Horn K, Kolbo JR: Using the Cumulative Strategies Model for drug abuse prevention: a small group analysis of the Choices Program. Am J Health Stud. 2000, 16 (1): 24-33.
Horn K, Kolbo JR: Application of a Cumulative Strategies Model for drug abuse prevention: exploring choices for high risk children. J Drug Educ. 2000, 30 (3): 291-312. 10.2190/UDC0-6ECT-EQCA-WVTT.
Tuttle J, Campbell-Heider N, Bidwell-Cerone S, Richeson G, Collins S: Teen Club: A nursing intervention for reducing risk-taking behavior and improving well-being in female African American adolescents. J Pediatr Health Care. 2000, 14 (3): 103-108.
Tuttle J, Campbell-Heider N, Bidwell-Cerone S, Richeson G, Collins S: Teen Club: intervention for adolescent children of substance abusing Parents: a study of five-year-options. Adolescent and Family Health. 2001, 2 (1): 47-
Catalano RF, Gainey RR, Fleming CB, Haggerty KP, Johnson NO: An experimental intervention with families of substance abusers: One-year follow-up of the Focus on Families project. Addiction. 1999, 94 (2): 241-254. 10.1046/j.1360-0443.1999.9422418.x.
Haggerty KP, Skinner M, Fleming CB, Gainey RR, Catalano RF: Long-term effects of the Focus on Families project on substance use disorders among children of parents in methadone treatment. Addiction. 2008, 103 (12): 2008-2016. 10.1111/j.1360-0443.2008.02360.x.
Aktan G, Kumpfer KL, Turner C: The Safe Haven program: effectiveness of a family skills training program for substance abuse prevention with inner city African American families. Int J Addict. 1996, 31: 158-175.
Campbell-Heider N, Tuttle J, Bidwell-Cerone S, Richeson G, Collins S: The buffering effects of connectedness: Teen Club intervention for children of substance abusing families. J Addict Nurs. 2003, 14: 175-182. 10.1080/jan.14.4.175.182.
Campbell-Heider N, Tuttle J, Knapp TR: The effect of positive life skills training on long term outcomes for high risk teens. J Addict Nurs. 2009, 20 (1): 6-15. 10.1080/10884600802693165.
Tuttle J, Campbell-Heider N, David TM: Positive adolescent life skills training for high risk teens. J Pediatr Health Care. 2006, 20 (3): 184-191. 10.1016/j.pedhc.2005.10.011.
Kumpfer KL: Outcome measures of interventions in the study of children of substance abusing parents. Pediatrics. 1999, 103 (5): 1128-1144.
Aktan G: Organizational framework for a substance use prevention program. Int J Addict. 1995, 30: 185-201.
Roth A, Fonagy P: What works for whom? A critical review of psychotherapy research. 2005, New York: Guilford Press, 2
Werch CE, Owen DM: Iatrogenic effects of alcohol and drug prevention programs. Journal of Studies on Alcohol. 2002, 63 (5): 581-590.
Moos RH: Iatrogenic effects of psychosocial interventions for substance use disorders: prevalence, predictors, prevention. Addiction. 2005, 100 (5): 595-604. 10.1111/j.1360-0443.2005.01073.x.
Lilienfeld SO: Psychological Treatments That Cause Harm. Perspect Psychol Sci. 2007, 2 (1): 53-70. 10.1111/j.1745-6916.2007.00029.x.
Cowan PA, Powell D, Cowan CP: Parenting interventions. A family systems perspective. Edited by: Sigle IE, Renninger KA. 1998, New York: Wiley, 3-72. 5
Markus E, Lange A, Pettigrew TF: Effectiveness of family therapy: A meta-analysis. J Fam Ther. 1990, 12: 205-221. 10.1046/j..1990.00388.x.
Small S, Conney SM, O’Connor C: Evidence-informed program improvement: Using principles of effectiveness to enhance the quality and impact of family-based prevention programs. Fam Relat. 2009, 58: 1-13. 10.1111/j.1741-3729.2008.00530.x.
Acknowledgements
Part of this work was supported by a grant from the Federal Ministy of Health, Germany (Grant number: 684 69).
We would like to thank Gurli Hermann for acting as second reviewer.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
Prof. Karol Kumpfer is a co-officer in Lutra Group, Inc. that disseminates the SFP curriculum, delivers the trainings, and conducts the evaluations. We declare that no further conflicts of interest exist. The authors declare that they have no competing interests.
Authors’ contributions
SB, KKu, KKr planned the design and drafted the manuscript. P-MS contributed methods consulting and critical revision. KKr, IS-B interpreted and analyzed data, ISB, SR, DM, EP collected data and researched articles. MK, RT were involved in all parts of the review as general supervisors of the research group. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Bröning, S., Kumpfer, K., Kruse, K. et al. Selective prevention programs for children from substance-affected families: a comprehensive systematic review. Subst Abuse Treat Prev Policy 7, 23 (2012). https://doi.org/10.1186/1747-597X-7-23
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1747-597X-7-23