
Abstract
Background
The chronic health effects from exposure to ambient air pollution are still unclear. This study primarily aims to examine the relationship between long-term exposure to ambient air pollution and respiratory morbidities in Chinese children.
Methods
A cross-sectional study was conducted among 2,203 school children aged 8–10 in three districts with different air pollution levels in Hong Kong. Annual means for ambient PM10, SO2, NO2 and O3 in each district were used to estimate participants’ individual exposure. Two questionnaires were used to collect children’s respiratory morbidities and other potential risk factors. Multivariable logistic regression was fitted to estimate the risks of air pollution for respiratory morbidities.
Results
Compared to those in the low-pollution district (LPD), girls in the high-pollution district (HPD) were at significantly higher risk for cough at night (ORadj. = 1.81, 95% CI: 1.71-2.78) and phlegm without colds (ORadj. = 3.84, 95% CI: 1.74-8.47). In addition, marginal significance was reached for elevated risks for asthma, wheezing symptoms, and phlegm without colds among boys in HPD (adjusted ORs: 1.71-2.82), as well as chronic cough among girls in HPD (ORadj. = 2.03, 95% CI: 0.88-4.70).
Conclusions
Results have confirmed certain adverse effects on children’s respiratory health from long-term exposure to ambient air pollution. PM10 may be the most relevant pollutant with adverse effects on wheezing and phlegm in boys. Both PM10 and NO2 may be contributing to cough and phlegm in girls.
Similar content being viewed by others


Background
Air pollution is a major environmental health risk in both developing and developed countries [1, 2]. It has been estimated that globally each year about 1.3 million premature deaths are attributed to ambient air pollution. In general, people living in less polluted cities have better respiratory and cardiovascular health and the related disease burden can be reduced by improving the ambient air quality [1]. Children are vulnerable to ambient air pollution as they spend more time outdoors, are more physically active, and have higher ventilation rates than adults. Though acute health effects on children’s respiratory morbidities from short-term exposure to air pollution have been well documented, the chronic effects from long-term exposure are still subject to debate. Two Harvard studies revealed chronic adverse effects on children’s cough and bronchitis from exposure to particulate matters (PMs) and sulphur dioxide (SO2) [3, 4], whilst a Southern California 24-city study reported insignificant associations between PMs and SO2 and childhood respiratory morbidities [5]. In addition, this study observed a significant association between nitrogen dioxide (NO2) and wheezing in boys [5]. Several studies in Europe and Asia have suggested that traffic-related pollution is significantly associated with children’s asthma, allergic rhinitis, and related symptoms [6–9]. Whilst findings from the International Study of Asthma and Allergies in Childhood (ISAAC) indicated that particulate matters than 10 μm in aerodynamic diameter (PM10) was not significantly associated with asthma and rhinoconjunctivities [10].
Hong Kong is located on the coast of Southern China and has a subtropical climate. The ambient air pollution level has improved since 1990, as the result of the implementation of a series of government regulations to restrict fuel’s sulphur content. However, in recent years, progress improvement has slowed down and the air quality has deteriorated, due to the fact that the local air quality is being influenced by the regional air pollution problem of the entire Southern China [11]. Previous studies in the 1990’s have revealed significant adverse effects of ambient air pollution on respiratory morbidities among Hong Kong school children, including cough, phlegm, and asthma [12]. Decreased bronchial hyperactivity among asthmatic children was also observed after a marked reduction in ambient PM10 and SO2 concentrations [13]. In addition, a four-city study in China showed significant associations between PMs and persistent cough, persistent phlegm, and bronchitis [14]. However, no significant adverse effect was found for SO2 and nitrogen oxides (NOx) [14]. These Chinese studies were conducted at least a decade ago and air pollution levels at that time were relatively high. Furthermore, none of these studies considered the potential health effects of ozone (O3), which is currently a routinely monitored air pollutant in urban China. This study primarily aims to investigate the associations between exposure to ambient air pollution and respiratory morbidities among Chinese primary school children in Hong Kong. In addition, the risks from indoor household factors for respiratory health were also examined.
Methods
Study population
This cross-sectional study was conducted from March to June among primary school students in three of Hong Kong. Given that PM10 is the major pollutant in Hong Kong and existing evidence suggests that PMs may be the most relevant air pollutant causing children’s respiratory morbidities through long-term exposure [11, 15, 16], three districts, labelled as low-pollution district (LPD), moderate-pollution district (MPD) and high-pollution district (HPD), were selected from ten districts with urban general air monitoring stations based on the rank of their annual means for PM10 over the previous 10 years. LPD and HPD were the districts with the lowest and highest PM10 values respectively to maximise the difference in exposure levels. MPD was selected as its PM10 annual mean was nearest to the average of those in LPD and HPD. LPD and HPD are new towns with predominantly residential buildings, while MPD is an old urban area with a combination of residential, commercial and factory buildings [11]. Three or four primary schools in each district, which are located within 1 km from the local air monitoring station, were invited to participate in the study using the “the closest to the station, the first to be selected” criterion. In addition, schools with any factories/industrial plants within a 100-meter range were excluded from the study to avoid the influences from point pollution sources. Only Chinese students in grades three and four were invited into the study, as the questionnaires were only in Chinese. In order to reduce exposure misclassification, only students who had been currently living in the district where their school was located for more than 12 consecutive months prior to the study were selected for data analysis. In addition, only children aged 8–10 were included in the data analysis, as few students (3.4%) were beyond this age range.
Ethics statement
Ethical approval was obtained from the Ethics Committee of the Chinese University of Hong Kong. Informed written consent was obtained from parents or guardians of all participants prior to the study.
Air pollution data
Four study pollutants, namely PM10, NO2, SO2, and O3 are continuously measured in Hong Kong [11]. Annual mean average in the past 10 years (covering the lifetime of the participants) and annual mean in the year prior to the study were used to estimate lifetime and current exposure levels of the participants, respectively [11].
Questionnaires
Two self-administered questionnaires, Parent Questionnaire and Child Questionnaire based on the Children’s Questionnaire recommended by the American Thoracic Society (ATS-DLD-78-C), were developed to collect information related to children’s respiratory morbidities and potential confounding factors [17]. Questions to assess asthma-suggesting symptoms were adopted from the Asthma and Allergies in Childhood Written Questionnaire (ISAAC WQ) Chinese version [18]. Parents completed the Parent Questionnaire and reported on children’s respiratory symptoms and diseases, socio-demographic characteristics, indoor housing environmental factors, parental history of asthma and allergy, children’s birth weight, birth place and breastfeeding history. Children completed the Child Questionnaire and reported smoking habits, time spent outdoors, amount and type of physical activities, participation in team sports and playing with furry toys in the past 12 months.
Respiratory diseases, including asthma, bronchitis and allergic rhinitis, were defined as doctor-diagnosed diseases at any time in the child’s life (life-time condition) and in the previous 12 months (current condition). Symptoms experienced in the past 12 months included wheezing with shortness of breath, wheezing with medication, any wheezing, cough at night, chronic cough, phlegm with/without colds and sneeze with itchy-watery eyes.
Statistical analysis
Data were analysed with SPSS for windows 16.0. Percentage and mean and standard deviation (SD) were used to describe the distribution of all variables. Chi-square and one-way ANOVA were performed to compare between-group differences. Multivariable logistic regressions were fitted to estimate the risk of air pollution (independent variable, indicated by district) for respiratory morbidities (dependent variables), after adjustment for other confounders. Adjusted odds ratio (adjusted OR) and 95% confidence intervals (95% CI) were then derived. Age, father’s job, and birth place were forcedly included in all models. Other binary variables were selected in a stepwise method using P < 0.10 and P < 0.15 as entry and removal criteria of variables respectively, including low birth weight (<2.5 kg), breastfeeding, parental asthma, parental allergy, active smoking, physical activity, member of team sports, time spent outdoors, playing with furry toys, having mould in the home, adding new furniture, raising pets, burning incense, passive smoking at home, home more-ventilated in summer and home more-ventilated in winter [19].
Results
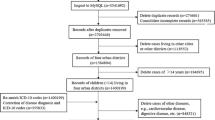
A total of 3,186 children in 11 primary schools were approached and 2,641 (82.9%) participated in the study. More than 95% of the participants (n = 2,534) completed questionnaires and finally 2,203 students (1141 boys and 1062 girls) met our selection criteria and were included in data analyses. Of the 331 students who were excluded from data analysis, 93 were living in other districts (cross-district students), 149 had lived in their school’s district for less than 12 consecutive months, and 89 were below 8 or above 10 years old.
The averages of historical annual means for PM10, NO2, SO2 and O3 in the past decade were 48.9 μg/m3, 48.4 μg/m3, 13.4 μg/m3, 38.6 μg/m3 in LPD, 55.0 μg/m3, 71.0 μg/m3, 16.3 μg/m3, 22.9 μg/m3 in MPD, and 57.6 μg/m3, 57.6 μg/m3, 18.6 μg/m3, 25.8 μg/m3 in HPD, respectively. O3 concentrations steadily increased over time, whilst no obvious increasing or decreasing trends were observed for the other three pollutants. PM10, NO2 and SO2 were positively correlated with each other, with significant correlations between PM10 and SO2, and between PM10 and NO2 (r = 0.70 and 0.51 respectively, P < 0.05). O3 was negatively correlated with the other three pollutants, and significantly correlated with PM10 and NO2 (r = −0.59 and −0.61 respectively, P < 0.05). The negative correlations for O3 with PM10 and NO2 are due to motor vehicles, which is the major source of air pollution in Hong Kong. O3 is readily scavenged by reactions with nitric oxide emitted from motor vehicles. In the past 12 months, the annual means for PM10, NO2, SO2 and O3 were 55.1 μg/m3, 51.4 μg/m3, 15.4 μg/m3, 42.5 μg/m3 in LPD, 56.3 μg/m3, 64.7 μg/m3, 15.2 μg/m3, 35.2 μg/m3 in MPD, and 63.8 μg/m3, 64.1 μg/m3, 22.2 μg/m3, 31.7 μg/m3 in HPD, respectively. Compared with the historical data, the concentrations of PM10 and SO2 in LPD, and that of NO2 in HPD had increased in the past 12 months towards the levels monitored in MPD.
Table 1 demonstrates the comparison of the participants’ characteristics across districts after stratification by gender. Significant differences were observed in: father’s job, birth place, breastfeeding history, parental allergy, physical activity, member of team sports, playing with furry toys, household mould, pets, burning incense at home, passive smoking, and house ventilation in summer and winter, for single or both genders.
Table 2 demonstrates the prevalence of respiratory morbidities by gender and district. Few students (<6.0%) experienced wheezing symptoms, chronic cough and phlegm without colds, in the past 12 months, whilst cough at night, phlegm with colds, and sneeze with itchy-watery eyes were common (20%-32.3%). Few students were diagnosed with asthma, whilst more than 30% of them had allergic rhinitis. In addition, differences across districts reached significance in the following morbidities: cough at night in girls, sneeze with itchy-watery eyes and life-time allergic rhinitis in boys, and phlegm without colds, current and life-time allergic rhinitis in both genders.
Tables 3 and 4 present the risks of ambient air pollution for respiratory morbidities after stratification by gender and adjustment for other risk factors. Compared to those in LPD, girls in HPD were at significantly higher risk for cough at night and phlegm without colds (ORadj. = 1.81, 95%CI = 1.17-2.78; and ORadj. = 3.84, 95%CI = 1.78-8.47, P < 0.05), and girls in MPD were at significantly higher risk for cough at night only (ORadj. = 1.65, 95%CI = 1.08-2.52, P < 0.05). Contrary to our hypothesis, both boys and girls in MPD were significantly less likely to have current and life-time allergic rhinitis compared to their counterparts in LPD (adjusted ORs ranged from 0.71 to 0.56, P < 0.05). In addition, boys in HPD were found to be at marginally significant higher risk for wheezing symptoms, phlegm without colds, and current and life-time asthma compared to those in LPD (adjusted ORs ranged from 1.71 to 2.82, P < 0.10). Marginal significance for elevated risk for cough at night was also found among boys in MPD (ORadj. = 1.43, 95%CI = 0.98-2.08, P < 0.10).
In the multivariable analysis (Tables 3 and 4), age, father’s job and birth place were adjusted for in all models no matter their significance. Blue-collar job of father was significantly and negatively associated with phlegm without colds and life-time allergic rhinitis for girls (adjusted ORs ranged from 0.56 to 0.71, P < 0.05). Boys born in Hong Kong were significantly less likely to have cough at night (ORadj. = 0.63, 95%CI = 0.40-0.98, P < 0.05), but significantly more likely to suffer from sneeze with itchy-watery eyes, and allergic rhinitis (adjusted ORs ranged from 1.80 to 2.27, P < 0.05). Parental asthma and parental allergy were risk factors for most respiratory conditions (adjusted ORs ranged from 1.89 to 5.32, P < 0.05). In terms of the other confounders, physical activity, being a member of a sports team, raising pets, and more-ventilated in summer were significantly and negatively associated with some respiratory conditions; whilst children with low birth weight, spending more time outdoors, playing with furry toys, having mould at home, new furniture, burning incense, passive smoking and more-ventilated in winter were significantly more vulnerable to some morbidities (Tables 3 and 4). It is worth noting that more-ventilated in summer seemed to be a protective factor for allergic rhinitis, and sneeze with itchy-watery eyes, whilst more-ventilated in winter had adverse effects on allergic rhinitis. In addition, being physically active was a significantly high risk factor for life-time asthma in girls.
We hypothesised that exposure to current air pollution (in the past 12 months) would have more influence on respiratory symptoms and diseases (in the past 12 months), when compared to historical exposure. Thus, the average monthly means for the air pollutants over the past 12 months allowed us to estimate the associations between some individual pollutants and current symptoms and diseases through regrouping the districts as follows: 1) LPD and MPD were combined together and then compared with HPD, as PM10 in LPD and MPD were both at a low level (55.1 μg/m3 and 56.3 μg/m3 respectively); 2) MPD and HPD were combined and then compared with LPD to reflect the same high level of NO2 in MPD and HPD (64.7 μg/m3 and 63.8 μg/m3 respectively). Significant or marginally significant adjusted ORs and their 95% CIs after regrouping are presented in Table 5. Boys in HPD were at significantly higher risk for wheezing symptoms and phlegm without colds compared to those in the combined LPD and MPD (adjusted ORs ranged from 2.03-2.76, P < 0.05), suggesting that it was PM10, but not NO2, which was mainly responsible for these adverse effects. However, both PM10 and NO2 contributed to the adverse effects on cough and phlegm in girls, as shown in Table 5 (adjusted ORs ranged from 1.71-2.87, P < 0.05). Contrary to our hypothesis, NO2 was significantly and negatively associated with current allergic rhinitis in girls.
Discussion
We conducted a cross-sectional study among 2,203 Hong Kong primary school students aged 8–10 years and uncovered certain adverse effects of ambient air pollution on respiratory symptoms and diseases. Girls living in HPD were at significantly higher risk for cough at night and phlegm without colds. Marginal significance for elevated risks was found for wheezing symptoms, phlegm without colds, and asthma in HPD boys, as well as chronic cough in HPD girls. Both genders in MPD were significantly less likely to have allergic rhinitis. Individual pollutant analysis further revealed that PM10 was the major pollutant responsible for the adverse effects on wheezing and phlegm in boys, whilst both PM10 and NO2 were contributing to cough and phlegm in girls.
Our findings confirmed similar adverse effects of air pollution in several one-city cross-sectional studies in China [12, 20–25]. Higher prevalence rates of wheezing, cough, phlegm and asthma were consistently found among children living in high pollution areas, though outcome indicators across the studies were not exactly the same. In a previous study in Hong Kong, Yu et al. revealed that children living in a high pollution district were at high risk for frequent cough, frequent phlegm and asthma, but not for wheezing, bronchitis and allergic rhinitis [12]. Marginal significance was found for high risks for chronic cough and wheezing with shortness of breath [12]. In Yu’s study, the risk of ambient air pollution was estimated without further breakdown by gender and therefore the potential gender difference in response to exposure was unclear. In addition, the air pollutants assessed in the previous study consisted of only PM10, SO2, and NO2. The differences in the annual mean concentrations of the three pollutants between high and low pollution districts in Yu’s study were larger than those between HPD and LPD in the current study.
In this study, further individual pollutant analyses suggests that PM10 was mainly responsible for the elevated risk for some respiratory morbidities in children (including wheezing for boys, cough for girls, and phlegm for both genders), whilst NO2 could negatively affect cough and phlegm for girls only. PM10 is a mixture of solid, liquid or solid and liquid particles, and a large body of chemicals within PM10 (e.g. sulphates, polycyclic aromatic hydrocarbons, metals) can solely, or in combination, cause biological harm, which gives scientific support for its stronger associations with respiratory morbidities than the other pollutants observed in this study. Similar to our results, two previous cross-sectional studies in China, examining the health effects of individual pollutants, found that PMs were more responsible for the adverse effects than other pollutants [14, 26]. A four-city study in China reported a significantly adverse effect of PM10 on phlegm, whilst the effects of NOx and SO2 were weak and insignificant [14]. A six-city study in Northern China (Liaoning Province) found that total suspended particles (TSP), NOx and SO2 were significantly and positively associated with cough, phlegm, and asthma in single pollutant models, whilst the adverse effects of SO2 on all morbidities and that of NOx on asthma decreased and were no longer significant in three-pollutant models, suggesting TSP was a stronger pollutant than the two other gaseous pollutants [26]. A meta-analysis involving four cross-sectional studies in China, examining the relationship between long-term exposure to ambient air pollution and child respiratory symptoms and diseases, indicated that an increase of per μg/m3 annual mean for PM10 could increase the likelihood of respiratory morbidity by 0.44% (S.E. 0.02) [27]. It is noteworthy that, in our study, the results of the individual pollutant analysis (Table 5) should be considered cautiously, as we were unable to remove the potential effects of other pollutants from that of the individual pollutant. For instance, the combination of the two low PM10 districts (LPD + MPD) also had lower levels of SO2 compared to HPD, which limited our ability to distinguish the health effects of PM10 from SO2. Similarly, the combination of the two high NO2 districts (MPD + HPD) was also low in O3, if taking O3 into consideration.
Contrary to our hypothesis, we found significantly negative associations between air pollution and allergic rhinitis. Compared to LPD, children of both genders in MPD were less likely to suffer from allergic rhinitis. After regrouping the districts, results from the further individual pollutant analysis, showed that children in the high NO2 but low O3 districts (MPD + HPD) were less likely to suffer from allergic rhinitis than those in the low NO2 but high O3 district (LPD) in girls only (Table 5). It is biologically impossible that exposure to high NO2 could be of benefit to health. Thus, the high O3 in LPD might have contributed to the negative associations. In our study, O3 was negatively correlated with the three other pollutants due to the fact that background O3 in more polluted areas can be removed through reacting with NO [11]. In line with our study, a cross-sectional study in 331,686 middle-school students in Taiwan reported that allergic rhinitis was positively associated with long-term exposure to O3 [10]. However, other studies failed to find any chronic adverse effects of O3 on respiratory morbidities (including allergic rhinitis) in school children [5, 28]. Unlike acute effects, the chronic effect of O3 has not yet been well documented. One possibility is that the strong associations between PMs and respiratory morbidities in many studies may make it difficult to assess the individual role of ozone per se [2].
The gender-different responses to air pollution and greater NO2 effects on girls observed in our study were consistent with some previous studies [29–31], while other studies reported no gender differences [9], or greater effects of NO2 on boys [5]. Children with fathers in blue-collar jobs in this study were less likely to suffer from phlegm without colds and allergic rhinitis, which confirmed the findings from another study in Hong Kong [12]. Children born in Hong Kong were at higher risk for allergic rhinitis, reflecting the fact that the prevalence of allergic rhinitis was higher in Hong Kong Children than those in other places of China [12, 18]. Low birth weight was a risk factor for wheezing with shortness of breath and chronic cough, which is consistent with results from a study in China [26]. Children spending more time outdoors are expected to be exposed to more air pollution, however we only found an adverse relationship with cough at night in girls. In terms of housing environmental factors, we found that mould, passive smoking, burning incense, and adding new furniture were positively associated with some respiratory morbidities, in line with the findings from many other studies around the world. A more ventilated home in winter was a risk factor, whilst a more ventilated home in summer was a protective factor for respiratory morbidities. One possibility is that ambient air pollution in winter was heavy; thus, more ventilation might increase the exposure level to ambient air pollution, and therefore increase the likelihood of respiratory morbidities. However, outdoor air quality in summer was relatively clear, and therefore good ventilation could improve the indoor air quality and reduce the risks for respiratory symptoms and diseases. Some factors in our study were observed to have opposite associations with respiratory conditions, contrary to our hypothesis, such as being a team sport member for current asthma in boys, and pet keeping for life-time asthma in girls. It is possible that asthmatic children might not join in any team sports, and families with asthmatic children might avoid keeping pets, because parents of asthmatic children in Hong Kong are well aware of these two risk factors.
This study is subject to several limitations. It is a cross-sectional study, and therefore we are unable to establish the temporal order of cause and effect. Exposure misclassification may inevitably exist and bias our findings most likely towards the null, like other studies using ambient air monitoring data as a proxy of personal exposure levels [32]. As individual exposures among children living in the same district can vary largely due to influences from diverse micro-environmental and personal factors, such as different air pollution levels at home and different physical activity levels. Though we controlled for several potential household and behavioural factors, the bias could not be entirely corrected. Recall bias may be unavoidable with self-reported retrospective data. For example, parents were more likely to recall severe respiratory conditions than mild ones, and recent episodes than older ones. Such bias may have introduced misclassification of diseases and resulted in underestimations of the adverse health effects [32]. In this study, we only recruited Chinese students, although overall less than 1% of students in Hong Kong mainstream primary schools are non-Chinese. However, our results are unable to reflect the situation of non-Chinese children in Hong Kong. The length of residual time of the participants may affect the associations between air pollution and respiratory morbidities, especially for life-time diseases. However, we did not collect such data, and therefore could not control for its influence. If students in HPD had ever lived in a less polluted district than HPD, and/or students in LPD had ever lived in a more polluted district than LPD, the health risks of air pollution in this study might have been underestimated, and vice versa. Unlike those in western countries, most families having children in Hong Kong would not prefer to move in order to create a stable environment for their children’s growth. As shown in this study, only 5.6% of the participants (149/2641) had ever moved from one district to another over the past 12 months. Thus, the confounding effect of the length of time living in an area might not be a major threat to this study. In the future, there is a need for cohort studies to confirm the associations between air pollution and children’s respiratory morbidities observed in this study. In addition, the relatively small differences in air pollution level across the three study districts limits our ability to test significant effects of air pollution on children’s respiratory morbidities. Further studies should enlarge the range of air pollutant concentrations via multi-city studies. There were only three districts in this study; we were therefore unable to distinguish health effects of individual pollutant (e.g. PM10) from those of other pollutants.
Conclusions
In conclusion, we have confirmed certain adverse effects on child respiratory health from exposure to ambient air pollution in a Chinese urban setting. The adverse effects observed for PM10 appear to be stronger than other pollutants. Girls were more vulnerable to NO2 than boys. Our findings may be transferable to other developing countries characterized by similar air pollution patterns to China. Along with the publicity of air quality monitoring data and the introduction of PM2.5 as a routine monitoring air pollutant in some big Chinese cities in 2012, the relatively high level of ambient air pollution and its health impact have been recently received unprecedented attentions from the Chinese public. There is an urgent call for the government to take effective actions to reduce air pollution level. Our findings provide some evidence for professionals and policy-makers to improve air quality, in particular PM10 and NO2, to protect the health of children.
Abbreviations
- 95% CI:
-
95% confidence intervals
- ATS-DLD-78-C:
-
Children’s Questionnaire recommended by the American Thoracic Society
- HKEPD:
-
Environmental Protection Department of Hong Kong
- HPD:
-
High-pollution district
- ISAAC:
-
International Study of Asthma and Allergies in Childhood
- ISAAC WQ:
-
Asthma and Allergies in Childhood Written Questionnaire
- LPD:
-
Low-pollution district
- MPD:
-
Moderate-pollution district
- NO2:
-
Nitrogen dioxide
- NOx:
-
Nitrogen Oxides
- O3:
-
Ozone
- OR:
-
Odds ratio
- PM10:
-
Particulate matters less than 10 μm in aerodynamic diameter
- SD:
-
Standard deviation
- SO2:
-
Sulphur dioxide.
References
World Health Organization: WHO Air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide - Global update 2005 - Summary of risk assessment. 2006, Geneva: WHO Press
World Health Organization Regional Office for Europe: WHO Regional Publications, European Series, No. 91. Air quality guidelines for Europe, second edition, 2000. 2000, Copenhagen: WHO Regional Office for Europe
Ware JH, Ferris BG, Dockery DW, Spengler JD, Stram DO, Speizer FE, et al: Effects of ambient sulfur oxides and suspended particles on respiratory health of preadolescent children. Am Rev Respir Dis. 1986, 133: 834-842.
Dockery DW, Cunningham J, Damokosh AI, Neas LM, Spengler JD, Koutrakis P, et al: Health effects of acid aerosols on north American children: respiratory symptoms. Environ Health Perspect. 1996, 104: 500-5005. 10.1289/ehp.96104500.
Peters JM, Avol E, Navidi W, London SJ, Gauderman WJ, Lurmann F, et al: A study of twelve southern California communities with differing levels and types of air pollution. I. Prevalence of respiratory morbidity. Am J Respir Crit Care Med. 1999, 159: 760-767. 10.1164/ajrccm.159.3.9804143.
Wjst M, Reitmeir P, Dold S, Wulff A, Nicolai T, von Loeffelholz-Colberg EF, et al: Road traffic and adverse effects on respiratory health in children. BMJ. 1993, 307: 596-600. 10.1136/bmj.307.6904.596.
Edwards J, Walters S, Griffiths RK: Hospital admissions for asthma in preschool children: relationship to major roads in Birmingham, United Kingdom. Arch Environ Health. 1994, 49: 223-227. 10.1080/00039896.1994.9937471.
Shima M, Adachi M: Effect of outdoor and indoor nitrogen dioxide on respiratory symptoms in schoolchildren. Int J Epidemiol. 2000, 29: 862-870. 10.1093/ije/29.5.862.
Hwang BF, Lee YL, Jaakkola JJK, Guo YL: Traffic related air pollution as a determinant of asthma among Taiwanese school children. Thorax. 2005, 60: 467-473. 10.1136/thx.2004.033977.
Anderson HR, Ruggles R, Pandey KD, Kapetanakis V, Brunekreef B, Lai CKW, et al: Ambient particulate pollution and the world-wide prevalence of asthma, rhinoconjunctivitis and eczema in children: phase one of the International Study of Asthma and Allergies in Childhood (ISAAC). Occup Environ Med. 2010, 67: 293-300. 10.1136/oem.2009.048785.
Environmental Protection Department of Hong Kong: Air quality annual report. data is available on http://www.aqhi.gov.hk/en/download/air-quality-reportse469.html?showall=&start=1 on 27 June, 2012
Yu TS, Wong TW, Wang XR, Song H, Wong SL, Tang JL: Adverse effects of low-level air pollution on the respiratory health of schoolchildren in Hong Kong. J Occup Environ Med. 2001, 43: 310-316. 10.1097/00043764-200104000-00004.
Wong CM, Lam TH, Peters J, Hedley AJ, Ong SG, Tam AY, et al: Comparison between two districts of the effects of an air pollution intervention on bronchial responsiveness in primary school children in Hong Kong. J Epidemiol Community Health. 1998, 52: 571-578. 10.1136/jech.52.9.571.
Zhang JJ, Hu W, Wei F, Wu G, Korn LR, Chapman RS: Children’s respiratory morbidity prevalence in relation to air pollution in four Chinese cities. Environ Health Perspect. 2002, 110: 961-967. 10.1289/ehp.02110961.
Gao Y, Chan EYY, Zhu YJ, Wong TW: Adverse effect of outdoor air pollution on cardiorespiratory fitness in Chinese children. Atmos Environ. 2013, 64: 10-17.
Gao Y, Chan EYY, Li LP, Wong TW: Chronic effects of ambient air pollution on lung function among Chinese children. Arch Dis Child. 2013, 98: 128-135. 10.1136/archdischild-2011-301541.
Ferris BG: Epidemiology standardization project (American Thoracic Society). Am Rev Respir Dis. 1978, 118: 1-120.
Leung R, Wong G, Lau J, Ho A, Chan JK, Choy D, et al: Prevalence of asthma and allergy in Hong Kong schoolchildren: an ISAAC study. Eur Respir J. 1997, 10: 354-360. 10.1183/09031936.97.10020354.
Katz MH: Multivariable analysis: a practical guide for clinicians. 1999, Cambridge: Cambridge University Press
Wang SL, Guo XB, Zhang JL: Study on the effect of ambient air pollution on respiratory disease and symptoms among school-age children in Beijing [in Chinese]. J Environ Health. 2004, 21: 41-44.
Ye LJ, Sun WJ, Yu W: Study on the influence of air pollution inside door or outside door on the health of the school children [in Chinese]. Mod Prev Med. 2007, 34: 4686-4687.
Tian QX, Zhou LZ, Wang R, Tian ZM: The study about influences of the air pollution on the respiratory system health of the children and their parents in Lanzihou [in Chinese]. Environ Monit China. 2001, 17: 48-51.
Kong LL, He QC, Xu F, Xu KY, Guo H: Study on the effects of indoor and outdoor air pollution on the respiratory system of school-age children [in Chinese]. Environ Monit China. 2001, 17: 43-48.
Wu J, He Q, Du L: Cross-sectional study on the relationship of outdoor air pollution with children’s respiratory health in Guangzhou City [in Chinese]. South China J Prev Med. 2012, 38: 1-5.
Wu Y, Zhang J, Zhao X: Relationship between ambient air pollution and Children’s respiratory health in China. J Environ Health. 2009, 26: 471-477.
Pan GW, Zhang SJ, Feng YP, Takahashi K, Kagawa J, Yu LZ: Air pollution and children’s respiratory symptoms in six cities of Northern China. Respir Med. 2010, 104: 1903-1911. 10.1016/j.rmed.2010.07.018.
Aunan K, Pan XC: Exposure-response functions for health effects of ambient air pollution applicable for China - A meta-analysis. Sci Total Environ. 2004, 329: 3-16. 10.1016/j.scitotenv.2004.03.008.
Braun-Fahrlander C, Vuille JC, Sennhauser FH, Neu U, Kunzle T, Grize L: Respiratory health and long-term exposure to air pollutants in Swiss schoolchildren. SCARPOL Team: Swiss Study on Childhood Allergy and Respiratory Symptoms with Respect to Air Pollution, Climate and Pollen. Am J Respir Crit Care Med. 1997, 155: 1042-1049. 10.1164/ajrccm.155.3.9116984.
Pershagen G, Rylander E, Norberg S, Eriksson M, Nordvall SL: Air pollution involving nitrogen dioxide exposure and wheezing bronchitis in children. Int J Epidemiol. 1995, 24: 1147-1153. 10.1093/ije/24.6.1147.
Kramer U, Koch T, Ranft U, Ring J, Behrendt H: Traffic-related air pollution is associated with atopy in children living in urban areas. Epidemiology. 2000, 11: 64-70. 10.1097/00001648-200001000-00014.
Venn AJ, Lewis SA, Cooper M, Hubbard R, Britton J: Living near a main road and the risk of wheezing illness in children. Am J Respir Crit Care Med. 2001, 164: 2177-2180. 10.1164/ajrccm.164.12.2106126.
HEI Accountability Working Group: Assessing Health Impact of Air Quality Regulations: Concepts and Methods for Accountability Research, Communication 11. 2003, Boston MA: Health Effects Institute
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/14/105/prepub
Acknowledgments
We are very grateful to the students, their parents, the teachers in the participating schools and all of the field investigators. We would also like to extend our special thanks to Ms Amanda Jane PITKETHLY for kindly proofreading our manuscript in the revision process.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors declare that they have no competing interests.
Authors’ contributions
YG conceived the idea of the study, prepared the study proposal, collected data in the field, performed the data analysis, and drafted the manuscript. EYYC and LL participated in data analysis and assisted with the interpretation of data, and critically reviewed the manuscript. PWCL critically reviewed the manuscript. TWW conceived the study idea, supervised the preparation of the study proposal, data collection, data analysis, interpretation of data, and critically reviewed the manuscript. All authors read and approved the final manuscript. All authors participated in critical appraisal and revision of the manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Gao, Y., Chan, E.Y., Li, L. et al. Chronic effects of ambient air pollution on respiratory morbidities among Chinese children: a cross-sectional study in Hong Kong. BMC Public Health 14, 105 (2014). https://doi.org/10.1186/1471-2458-14-105
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-14-105