
Abstract
Background
An increase in macular thickness due to fluid accumulation in the macula in patients with diabetes mellitus. Optical coherence tomography (OCT) has been shown to be highly reproducible in measuring macular thickness in normal individuals and diabetic patients. OCT can detect subtle changes of macular thickness. The aim of this study is to compare central macular thickness (CMT) of diabetic patients with type 2 diabetes without clinical retinopathy and normal controls, in order to assess possible increased macular thickness associated with diabetes mellitus.
Methods
Optical coherence tomography (OCT) measurements were performed in 124 eyes of 62 subjects with diabetes mellitus without clinically retinopathy (study group: 39 female, 23 male, mean age: 55.06 ± 9.77 years) and in 120 eyes of 60 healthy subjects (control group: 35 female, 25 male, mean age: 55.78 ± 10.34 years). Blood biochemistry parameters were analyzed in all cases. The data for central macular thickness (at 1 mm) and the levels of the fasting plasma glucose and glycosylated hemoglobin (HbA1c) were compared in both groups.
Results
The mean central macular thickness was 232.12 ±24.41 μm in the study group and 227.19 ± 29.94 μm in the control group.
The mean HbA1c level was 8.92 ± 2.58% in the study group and 5.07 ± 0.70% in the control group (p=0.001). No statistically significant relationship was found between CMT, HbA1c, and fasting plasma glucose level in either group (p=0.05).
Conclusions
Central macular thickness was not significantly thicker in patients with type 2 diabetes without clinical retinopathy than in healthy subjects.
Similar content being viewed by others


Background
Diabetic retinopathy is the leading cause of blindness in working aged adults in westernized countries. Diabetic macular edema (DME) has been reported at rates of 10% and occurs more frequently in type 2 diabetes mellitus than in type 1. Diabetic patients also have multiple risk factors for retinopathy, such as hyperglycemia and hypertension [1]. Their visual acuity is often dependent the central foveal involvement, perifoveal capillary blood flow velocity, severity of perifoveal capillary occlusion, and retinal thickness at the central fovea [2, 3]. The clinical findings of diabetic retinopathy are microaneurysms, soft exudates, accumulation of hard exudates, and neovascularisation.
Macular edema can develop at any stage of diabetic retinopathy. In the past, macular edema was diagnosed with slit-lamp view. Fundus fluorescein angiography provides guidance for treatment of macular edema. Optical coherence tomography (OCT) has been used for detection of macular edema secondary to different pathologies, such as diabetes mellitus, central or branched retinal vein occlusion, uveitis, and age related macular degeneration [4]–[11].
Methods
The central macular thickness (CMT) was measured in both groups by OCT (Optovue Inc. Co., RTVue 100 model, Fremont, CA). The CMT was measured after providing pupil dilation with tropicamide drops 2 times, 10 minutes before measurement (Tropicamide 1%, Alcon Lab. Inc, USA). Three measurements were taken from each patient after pupillary dilatation. Blood biochemical tests for glycosylated hemoglobin (HbA1c) and fasting plasma glucose levels were run on all patients. All cases underwent ophthalmological examinations including best corrected visual acuity (BCVA), anterior and posterior segment examinations under slit-lamp, intraocular pressure (IOP) (applanation tonometer model AT 900; Haag-Streit, Switzerland), and central macular thickness measured by OCT Visual acuity was measured with an Early Treatment Diabetic Retinopathy Study chart at 4 meters. Each subject gave written informed consent to participate in the study. Ethic Committee approval was obtained from local committee.
Participiants
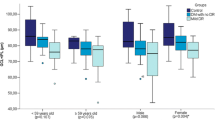
The study group included 62 patients (124 eyes; 39 female, 23 male, mean age: 55.06 ± 9.77 years) who had type 2 diabetes mellitus without clinical retinopathy and a control group of 60 patients (120 eyes; 35 female, 25 male, mean age: 55.78 ± 10.34 years) (Table 1). Inclusion criteria for the study group included: no visible findings of diabetic retinopathy (hard-soft exudates, microaneurysms) on retina at slit-lamp fundus examination with a +78 D lens, type 2 diabetes mellitus, no other problems (such as hypertension, uveitis), and no history of ophthalmologic trauma, intravitreal injection, high refractive errors (spherical equivalent; between: +1.00 D to −1.00 D) or use of drugs(s) for retinal problems. Inclusion criteria for the control group patients included: no ophthalmologic or systemic problems, no history of intraocular surgery or treatment of the retina, and no high refractive errors (spherical equivalent: between −1.0 D to +1.0 D). Exclusion criteria for both groups were visible retinopathy or uveitis, hypertension, or previous ophthalmologic surgery. In the study group, the duration of diabetes mellitus ranged from 0 – 20 years and the average was 7.19 ± 4.87 years. Five patients were newly diagnosed, 19 patients had been diagnosed for 1–5 years, 23 patients had been diagnosed for 6–10 years, 9 patients had been diagnosed for 11–15 years, and 6 patients had been diagnosed for more than 15 years. In the study group; five patients were newly diagnosed, 49 patients were undergoing insulin treatment, and 8 patients were taking oral antidiabetic drugs (Table 2). Both groups were compared based on mean age, central macular thickness, fasting plasma glucose, and HbA1c levels.
Statistical analysis
The NCSS (Number Cruncher Statistical System) 2007 and the PASS 2008 Statistical Software (Utah, USA) programs were used to evaluate the results of the study.
Descriptive statistical methods (mean, standard deviation) and Student’s t- test were used together to compare the data from the two groups and the parameters that showed normal distribution. The Mann Whitney U test was used to compare parameters of the two groups that did not show normal distribution. A Chi-square test was used to compare the quality of the data. Pearson correlation analyses were conducted to evaluate the relationship between the parameters showing normal distribution and Spearman’s rho correlation analyses have been used to evaluate correlation between the parameters not showing normal distribution. A value of p<0.05 was considered significant.
Results
Best corrected vision (BCVA) was 0.00 (log MAR) in both groups. No significant differences were found for the mean age, IOP, or gender distribution (Table 1).
The mean HbA1c level was 8.92 ± 2.58% in the study group, and 5.07 ± 0.70% in the control group. The mean level of HbA1c was statistically higher in the study group than in the control group (Table 1, p=0.001). Fasting plasma glucose level was statistically higher in the study group than in the control group (Table 1, p=0.01). The duration of diabetes mellitus was 7.19 ± 4.8 (range: 0–20) years. The mean of CMT was 232.12 ± 24.41 μm in the study group and 227.19 ± 29.94 μm in the control group (Table 1). The CMT was thicker in the study group than in the control group but this difference was not statistically significant.
No relationship was found between CMT and fasting plasma glucose level in the study (p=0.483) and control (p=0.399) groups. No relationship was found between CMT and HbA1c level in the study (p=0.550), and control (p=0.997; Table 3).
Discussion
We found no studies in the literature which reviewed CMT, fasting plasma glucose level, and level of HbA1c less than HbA1c 8%.
Several previous studies [12]–[17] determined that optical coherence tomography can help in the evaluation of macular edema in diabetic or non-diabetic patients, and also help in the follow-up of the patients during treatment to establish quantitative or qualitative responses to therapy.
We reviewed the relationship between central macular thickness, HbA1c, and fasting plasma glucose levels in patients with type 2 diabetes without clinical diabetic retinopathy. Optical Coherence Tomography (OCT) was used for objective measurement and monitoring of central macular thickness. Browning and Hee, et al. [18, 19] described that a change in the OCT measurements greater than 10% of the baseline thickness is likely to represent a true change in macular thickness. Glycosylated hemoglobin is a parameter that can be used to follow up hyperglycemia over the long term. Moon, at al [20] suggested that a high baseline HbA1c and a large reduction in HbA1c were risk factors for increase in macular thickness. Yeung, et al [21], showed that HbA1c level positively correlated with macular thickness in patients with type1 and 2 diabetes of10 or more years’ duration without diabetic macular edema. Chou, Moreira at al [22]. showed that a HbA1c level of 8% or above was associated with an increase in macular thickness in diabetic patients with diabetic retinopathy. Yeung, at al. [21]–[23] concluded that meticulous diabetes control may slow the progression of early diabetic retinopathy and may play an important role in preventing macular dysfunction. In type 1 and 2 diabetes patients, strict follow-up of plasma glucose level could reduce the progression and development of diabetic retinopathy.
The purpose of this study was to examine central macular thickness in patients with type 2 diabetes mellitus without retinopathy. This study showed the following four results: 1) The mean central macular thickness is thicker in diabetic patients without diabetic retinopathy than in healthy subjects, but this difference was not statistically significant; 2) No positive relationship was found between fasting plasma glucose level and the central macular thickness in patients with diabetes mellitus without retinopathy; 3) Central macular thickness was not increased by mild or high levels of HbA1c (8.92 ± 2.59%); and 4) Central macular thickness was not affected by the duration of diabetes mellitus in patients with diabetes type 2 without retinopathy. There are limitations to our study. One of these is the small sample size in both groups and another is that no patients had diabetes mellitus for longer than 20 years.
Conclusion
Our opinion is that the truly effective parameter on macular thickness is vascular permeability in patients with diabetes mellitus.
In this study, glycosylated HbA1c and fasting plasma glucose levels were significantly higher in diabetic patients without retinopathy than in the control group, although there was no difference in central macular thickness between the two groups.
References
Girach A, Lund-Andersen H: Diabetic macular oedema: a clinical overview. Int J Clin Pract. 2007, 61: 88-97. 10.1111/j.1742-1241.2006.01211.x.
Gardner TW, Larsen M, Girach A, Zhi X: Protein Kinase C Diabetic Retinopathy Study (PKC-DRS2) Study Group. Diabetic macular oedema and visual loss: relationship to location, severity and duration. Acta Ophthalmol. 2009, 87: 709-713. 10.1111/j.1755-3768.2009.01545.x.
Sakata K, Funatsu H, Harino S, Noma H, Hori S: Relationship of macular microcirculation and retinal thickness with visual acuity in diabetic macular edema. Ophthalmology. 2007, 114: 2061-2069. 10.1016/j.ophtha.2007.01.003.
Yahia SB, Kahloun R, Jelliti B, Khairallah M: Branch retinal artery occlusion associated with Behçet disease. Ocul Immunol Inflamm. 2011, 19: 293-295. 10.3109/09273948.2011.582219.
Ogino K, Tsujikawa A, Nakamura H, Miyamoto K, Murakami T, Muraoka Y, Yoshimura N: Focal macular electroretinogram in macular edema secondary to central retinal vein occlusion. Invest Ophthalmol Vis Sci. 2011, 52: 3514-3520. 10.1167/iovs.10-7142.
Browning DJ, McOwen MD, Bowen RM, O'Marah TL: Comparison of the clinical diagnosis of diabetic macular edema with diagnosis by optical coherence tomography. Ophthalmology. 2004, 111: 712-715. 10.1016/j.ophtha.2003.06.028.
Virgili G, Menchini F, Murro V, Peluso E, Rosa F, Casazza G: Optical coherence tomography (OCT) for detection of macular oedema in patients with diabetic retinopathy. Cochrane Database Syst Rev. 2011, 7: CD008081-
Ibrahim MA, Sepah YJ, Symons RC, Channa R, Hatef E, Khwaja A: Spectral- and time-domain optical coherence tomography measurements of macular thickness in normal eyes and in eyes with diabetic macular edema. Eye (Lond). 2012, 26: 454-462. 10.1038/eye.2011.293.
Medina FJ, Callén CI, Rebolleda G, Muñoz-Negrete FJ, Callén MJ, Valle FG: Use of Nonmydriatic Spectral-Domain Optical Coherence Tomography for Diagnosing Diabetic Macular Edema. Am J Ophthalmol. 2012, 153: 536-543. 10.1016/j.ajo.2011.08.008.
Suzuma K, Yamada Y, Liu M, Tsuiki E, Fujikawa A, Kitaoka T: Comparing central retinal thickness in diabetic macular edema measured by two different spectral-domain optical coherence tomography devices. Jpn J Ophthalmol. 2011, 55: 620-624. 10.1007/s10384-011-0085-4.
Kwon SI, Hwang DJ, Seo JY, Park IW: Evaluation of changes of macular thickness in diabetic retinopathy after cataract surgery. Korean J Ophthalmol. 2011, 25: 238-242. 10.3341/kjo.2011.25.4.238.
Udaondo P, Díaz-Llopis M, García-Delpech S, Salom D, Romero FJ: Intravitreal plasmin without vitrectomy for macular edema secondary to branch retinal vein occlusion. Arch Ophthalmol. 2011, 129: 283-287. 10.1001/archophthalmol.2011.8.
Moreira RO, Trujillo FR, Meirelles RM, Ellinger VC, Zagury L: Use of optical coherence tomography (OCT) and indirect ophthalmoscopy in the diagnosis of macular edema in diabetic patients. Int Ophthalmol. 2001, 24: 331-336.
Schneeberg AE, Göbel W: Diagnosis and follow-up of non-diabetic macular edema with optical coherence tomography (OCT). Ophthalmologe. 2003, 100: 960-966. 10.1007/s00347-003-0822-2.
Song JH, Lee JJ, Lee SJ: Comparison of the short-term effects of intravitreal triamcinolone acetonide and bevacizumab injection for diabetic macular edema. Korean J Ophthalmol. 2011, 25: 156-160. 10.3341/kjo.2011.25.3.156.
Takatsuna Y, Yamamoto S, Nakamura Y, Tatsumi T, Arai M, Mitamura Y: Long-term therapeutic efficacy of the subthreshold micropulse diode laser photocoagulation for diabetic macular edema. Jpn J Ophthalmol. 2011, 55: 365-369. 10.1007/s10384-011-0033-3.
Vemala R, Koshy S, Sivaprasad S: Qualitative and quantitative OCT response of diffuse diabetic macular oedema to macular laser photocoagulation. Eye (Lond). 2011, 25: 901-908. 10.1038/eye.2011.84.
Browning DJ, Fraser CM, Propst BW: The variation in optical coherence tomography-measured macular thickness in diabetic eyes without clinical macular edema. Am J Ophthalmol. 2008, 145: 889-893. 10.1016/j.ajo.2008.01.007.
Hee MR, Puliafito CA, Wong C, Duker JS, Reichel E, Rutledge B: Quantitative assessment of macular edema with optical coherence tomography. Arch Ophthalmol. 1995, 113: 1019-1029. 10.1001/archopht.1995.01100080071031.
Moon SW, Kim HY, Kim SW, Oh J, Huh K, Oh IK: The change of macular thickness measured by optical coherence tomography in relation to glycemic control in diabetic patients. Graefes Arch Clin Exp Ophthalmol. 2011, 249: 839-848. 10.1007/s00417-010-1562-z.
Yeung L, Sun CC, Ku WC, Chuang LH, Chen CH, Huang BY: Associations between chronic glycosylated haemoglobin (HbA1c) level and macular volume in diabetes patients without macular oedema. Acta Ophthalmol. 2010, 88: 753-758. 10.1111/j.1755-3768.2009.01711.x.
Chou TH, Wu PC, Kuo JZ, Lai CH, Kuo CN: Relationship of diabetic macular oedema with glycosylated haemoglobin. Eye (Lond). 2009, 23: 1360-1363. 10.1038/eye.2008.279.
Rosenstock J, Friberg T, Raskin P: Effect of glycemic control on microvascular complications in patients with type I diabetes mellitus. Am J Med. 1986, 81: 1012-1018. 10.1016/0002-9343(86)90398-0.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2415/13/11/prepub
Acknowledgements
Thanks to Celeste Krauss (and her team) who provided writing in good medical English CEO of http://www.Mededit.net
Thanks to Bendisah Karaer for helping to transfer of participiants to room of Optic Coherence Tomography.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors have no finacial competing interests.
Authors’ contributions
All authors conceived of and designed the experimental protocol. MD and EO contributed to the study design and did critical revision of the manuscript for important intellectual content. MD, EO and BD participated in the eye examinations. EO and EC collected the data. All authors read and approved the final manuscript.
An erratum to this article can be found at http://dx.doi.org/10.1186/s12886-015-0114-z.
The corresponding author submitted this article to the Journal of Ophthalmology although it was under review by BMC Ophthalmology. The article was subsequently accepted and published by the Journal of Ophthalmology and then by BMC Ophthalmology. As it has been brought to the attention of the Editor that duplicate submission and publication have taken place, the Editor has made the decision to retract the article published in BMC Ophthalmology.
A retraction note to this article can be found online at http://dx.doi.org/10.1186/s12886-015-0114-z.
An erratum to this article is available at http://dx.doi.org/10.1186/s12886-015-0114-z.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Demir, M., Oba, E., Dirim, B. et al. RETRACTED ARTICLE: Cental macular thickness in patients with type 2 diabetes mellitus without clinical retinopathy. BMC Ophthalmol 13, 11 (2013). https://doi.org/10.1186/1471-2415-13-11
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2415-13-11