
Abstract
OBJECTIVE: This study examined the prevalence, impact on health-related quality of life (HRQoL), and outcome of physical symptoms in depressed patients during 9 months of anti-depressant therapy.
DESIGN: Open-label, randomized, intention-to-treat trial with enrollment occurring April through November 1999.
SETTING: Thirty-seven primary care clinics within a research network.
PATIENTS: Five hundred seventy-three depressed patients started on one of three selective serotonin reuptake inhibitors (SSRIs) by their primary care physician and who completed a baseline interview.
INTERVENTIONS: Patients were randomized to receive fluoxetine, paroxetine, or sertraline.
MEASUREMENTS AND MAIN RESULTS: Outcomes assessed included physical symptoms, depression, and multiple domains of HRQoL. Prevalence of physical symptoms was determined at baseline and after 1, 3, 6, and 9 months of treatment. Stepwise linear regression models were used to determine the independent effects of physical symptoms and depression on HRQoL domains.
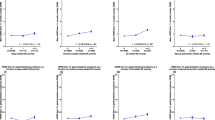
Of the 14 physical symptoms assessed, 13 were present in at least a third to half of the patients at baseline. Each symptom showed the greatest improvement during the initial month of treatment. In contrast, depression continued to show gradual improvement over a 9-month period. Physical symptoms had a predominant effect on pain (explaining 17% to 18% of the variance), physical functioning (13%), and overall health perceptions (13% to 15%). Depression had the greatest impact on mental (26% to 45%), social (14% to 32%), and work functioning (9% to 32%).
CONCLUSIONS: Physical symptoms are prevalent in depressed patients and initially improve in the first month of SSRI treatment. Unlike depression, however, improvement in physical symptoms typically plateaus with minimal resolution in subsequent months.
Similar content being viewed by others


References
Kroenke K, Spitzer RL, Williams JB, et al. Physical symptoms in primary care: predictors of psychiatric disorders and functional impairment. Arch Fam Med. 1994;3:774–9.
Katon W, Kleinman A, Rosen G. Depression and somatization: a review. Part I. Am J Med. 1982;72:127–35.
Katon W, Kleinman A, Rosen G. Depression and somatization: a review. Part II. Am J Med. 1982;72:241–7.
Kroenke K, Jackson JL, Chamberlin J. Depressive and anxiety disorders in patients presenting with physical complaints: clinical predictors and outcome. Am J Med. 1997;103:339–47.
Kroenke K. Patients presenting with somatic complaints: epidemiology, psychiatric comorbidity and management. Int J Methods Psychiatr Res. 2003;12:34–43.
Sullivan M, Katon W. Somatization. APS J. 1993;3:141–59.
Mathew RJ, Weinman ML, Mirabi M. Physical symptoms of depression. Br J Psychiatry. 1981;139:293–6.
Simon G, VonKorff M. Somatization and psychiatric disorder in the NIMH Epidemiologic Catchment Area Study. Am J Psychiatry. 1991;11:1494–500.
Katon W, Sullivan M, Walker E. Medical symptoms without identified pathology: relationship to psychiatric disorders, childhood and adult trauma, and personality traits. Ann Intern Med. 2001;134:917–25.
Kirmayer LJ, Robbins JM, Dworkind M, Yaffe MJ. Somatization and the recognition of depression and anxiety in primary care. Am J Psychiatry. 1993;5:734–41.
Bridges KW, Goldberg DP. Somatic presentations of DSM III psychiatric disorders in primary care. J Psychosom Res. 1985;29:563–9.
Kirmayer L, Robbins J. Patients who somatize in primary care: a longitudinal study of cognitive and social characteristics. Psychol Med. 1996;26:937–51.
Simon G, VonKorff M, Piccinelli M, Fullerton C, Omel J. An international study of the relation between somatic symptoms and depression. N Engl J Med. 1999;341:1329–35.
Kroenke K, Jackson JL. Outcomes in general medical patients presenting with common symptoms: a prospective study with a 2-week and a 3-month follow-up. Fam Pract. 1998;5:398–403.
Kroenke K, West SL, Swindle R, et al. Similar effects of paroxetine, fluoxetine, and sertraline in primary care: a randomized trial. JAMA. 2001;286:2947–55.
Simon GE, Revicki D, VonKorff M. Telephone assessment of depression severity. J Psychiatr Res. 1993;27:247–52.
Katon W, Robinson P, VonKorff M, et al. A multifaceted intervention to improve treatment of depression in primary care. Arch Gen Psychiatry. 1996;53:924–32.
Unützer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA. 2002;288:2836–45.
Spitzer RL, Kroenke K, Williams JBW. Patient Health Questionnaire Study Group. Validity and utility of a self-report version of PRIME-MD. JAMA. 1999;282:1737–44.
Kroenke K, Spitzer RL, Williams JBW. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–13.
Kroenke K, Spitzer RL, Williams JB. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med. 2002;64:258–66.
Ware JE. SF-36 Health Survey: Manual and Interpretation Guide. Boston, Mass: The Health Institute, New England Medical Center; 1993.
Ware JE, Gandek B. The SF-36 Health Survey: development and use in mental health research and the IQOLA project. Int J Ment Health. 1994;23:49–73.
Lerner D, Amick B III, Glaxo Wellcome, Inc. Work Limitations Questionnaire. Boston, Mass: The Health Institute, New England Medical Center; 1998.
Stewart AL, Ware JE. Measuring Functioning and Well-Being: The Medical Outcomes Study Approach. Durham, NC: Duke University Press; 1992.
Spitzer RL, Williams JBW, Kroenke K, et al. Utility of a new procedure for diagnosing mental disorders in primary care: the PRIME-MD 1000 study. JAMA. 1994;272:1749–56.
Moos RH, Cronkite RC, Finney JW. Health and Daily Living Form Manual. Palo Alto, Calif: Mind Garden; 1990.
VonKorff M, Wagner EH, Saunders K. A chronic disease score from automated pharmacy data. J Clin Epidemiol. 1992;45:197–203.
Clark DO, Von Korff M, Saunders K, et al. A chronic disease score with empirically derived weights. Med Care. 1995;33:783–95.
Unutzer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA. 2002;288:2836–45.
Widmer RB, Cadoret RJ. Depression in primary care: changes in pattern of patient visits and complaints during a developing depression. J Fam Pract. 1978;7:293–302.
Widmer RB, Cadoret RJ. Depression in family practice: changes in pattern of patient visits and complaints during subsequent developing depressions. J Fam Pract. 1979;9:1017–21.
Bair MJ, Robinson RL, Katon W, Kroenke K. Exploring depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163:2433–45.
Bair MJ, Robinson RL, Eckert GJ, Stang PE, Crogan TW, Kroenke K. Impact of pain on depression treatment response in primary care. Psychosom Med. 2002;66:17–22.
O’Malley PG, Jackson JL, Tomkins G, Santoro J, Balden E, Kroenke K. Antidepressant therapy for unexplained symptoms and symptom syndromes: a critical review. J Fam Pract. 1999;48:980–93.
Kroenke K, Swindle R. Cognitive-behavioral therapy for somatization and symptom syndromes: a critical review of clinical trials. Psychother Psychosom. 2000;69:205–15.
Allen LA, Escobar JI, Lehrer PM, Gara M, Woolfolk RL. Psychosocial treatments for multiple unexplained physical symptoms: a review of literature. Psychosom Med. 2002;64:939–50.
Author information
Authors and Affiliations
Corresponding author
Additional information
The ARTIST trial was supported by a grant from Eli Lilly. Work on this paper was also supported by Grant T-32 PE15001 from the Health Resources and Service Administration.
Rights and permissions
About this article
Cite this article
Greco, T., Eckert, G. & Kroenke, K. The outcome of physical symptoms with treatment of depression. J GEN INTERN MED 19, 813–818 (2004). https://doi.org/10.1111/j.1525-1497.2004.30531.x
Issue Date:
DOI: https://doi.org/10.1111/j.1525-1497.2004.30531.x