
Abstract
Background
Fat embolism syndrome (FES) is commonly reported in the setting of long bone and pelvic fractures, but the etiology and pathogenesis are unclear. The aim of this study was to identify clinical characteristics and laboratory findings that may place orthopedic trauma patients at a higher risk of developing FES.
Methods
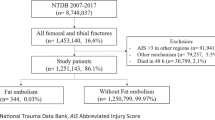
Electronic medical records were reviewed of all patients aged 18–89 years from 2015 to 2020 with a mention of FES in the patient chart who met Gurd and Wilson’s criteria for diagnosis after experiencing orthopedic trauma. A 3:1 matched pair analysis was performed between FES patients and those with similar age, gender, and FES-associated fracture (femur, tibia, humerus, or pelvis fracture).
Results
18 patients with FES who met inclusion criteria were identified. Hypomagnesemia (OR = 7.43), hyperphosphatemia (OR = 6.24), hypoalbuminemia (OR = 3.78), blunt traumatic mechanism of injury (OR = 7.16) and a greater number of bones fractured (Avg/SD = 2.89/1.53) were seen more often in FES patients (all p-values < 0.05).
Conclusion
Findings of this study suggest that patients with hypomagnesemia, hyperphosphatemia, hypoalbuminemia, a blunt trauma mechanism of injury, and an increased number of bones fractured are at increased risk for the development of FES. This may be related to their roles in physiologic oncotic pressure and inflammatory response, and thus further investigation of these variables is necessary for the evaluation of FES prevention.
Level of evidence
Level 3.
Similar content being viewed by others

References
Gurd, A. R., & Wilson, R. I. (1974). The fat embolism syndrome. Journal of Bone and Joint Surgery. British Volume, 56B(3), 408–416.
Levy, D. (1990). The fat embolism syndrome. A review. Clinical Orthopaedics and Related Research, 261, 281–286.
Talbot, M., & Schemitsch, E. H. (2006). Fat embolism syndrome: History, definition, epidemiology. Injury, 37(Suppl 4), S3-7. https://doi.org/10.1016/j.injury.2006.08.035 ((Erratum In: Injury 2007Oct;38(10):1224)).
Baker, P. L., Pazell, J. A., & Peltier, L. F. (1971). Free fatty acids, catecholamines, and arterial hypoxia in patients with fat embolism. Journal of Trauma, 11(12), 1026–1030. https://doi.org/10.1097/00005373-197112000-00006.
Gossling, H. R., & Pellegrini, V. D., Jr. (1982). Fat embolism syndrome: a review of the pathophysiology and physiological basis of treatment. Clinical Orthopaedics and Related Research, 165, 68–82.
Scarpino, M., Lanzo, G., Lolli, F., & Grippo, A. (2019). From the diagnosis to the therapeutic management: Cerebral fat embolism, a clinical challenge. International Journal of General Medicine, 4(12), 39–48. https://doi.org/10.2147/IJGM.S177407.
Shaikh, N. (2009). Emergency management of fat embolism syndrome. Journal of Emergencies, Trauma, and Shock, 2(1), 29–33. https://doi.org/10.4103/0974-2700.44680.
Kwiatt, M. E., & Seamon, M. J. (2013). Fat embolism syndrome. International Journal of Critical Illness and Injury Science, 3(1), 64–68. https://doi.org/10.4103/2229-5151.109426.
Mazur, A., Maier, J. A., Rock, E., Gueux, E., Nowacki, W., & Rayssiguier, Y. (2007). Magnesium and the inflammatory response: potential physiopathological implications. Archives of Biochemistry and Biophysics, 458(1), 48–56. https://doi.org/10.1016/j.abb.2006.03.031 ((Epub 2006 Apr 19)).
Yamada, S., Tokumoto, M., Tatsumoto, N., Taniguchi, M., Noguchi, H., Nakano, T., et al. (2014). Phosphate overload directly induces systemic inflammation and malnutrition as well as vascular calcification in uremia. American Journal of Physiology. Renal Physiology, 306(12), F1418–F1428. https://doi.org/10.1152/ajprenal.00633.2013 ((Epub 2014 May 7)).
Jono, S., McKee, M. D., Murry, C. E., et al. (2000). Phosphate regulation of vascular smooth muscle cell calcification. Circulation Research, 87(7), e10.
Soeters, P. B., Wolfe, R. R., & Shenkin, A. (2019). Hypoalbuminemia: Pathogenesis and clinical significance. Journal of Parenteral and Enteral Nutrition, 43(2), 181–193. https://doi.org/10.1002/jpen.1451 ((Epub 2018 Oct 4)).
Stein, P. D., Yaekoub, A. Y., Matta, F., & Kleerekoper, M. (2008). Fat embolism syndrome. American Journal of the Medical Sciences, 336(6), 472–477. https://doi.org/10.1097/MAJ.0b013e318172f5d2.
Bolliger, S. A., Muehlematter, K., Thali, M. J., & Ampanozi, G. (2011). Correlation of fat embolism severity and subcutaneous fatty tissue crushing and bone fractures. International Journal of Legal Medicine, 125(3), 453–458. https://doi.org/10.1007/s00414-011-0563-8 ((Epub 2011 Mar 19)).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical standard statement
Our instutition’s IRB approved a HIPPA waiver for this study on January 8, 2020 since it met all criteria for waiver approval.
Informed consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lowery, A., Naran, V., Ames, R. et al. Risk Stratification Algorithm for Orthopedic Trauma Patients at Risk for Fat Embolism Syndrome. JOIO 55, 879–885 (2021). https://doi.org/10.1007/s43465-021-00365-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43465-021-00365-x