
Abstract
Objectives
The aim of this study was to describe a nationwide system for pre-marketing follow-up (cohort temporary utilization authorization [ATU] protocol; i.e., ‘therapeutic utilization’) of a new taste-masked formulation of sodium phenylbutyrate (NaPB) granules (Pheburane®) in France and to analyze safety and efficacy in this treated cohort of patients with urea cycle disease (UCD).
Methods
In October 2012, a cohort ATU was established in France to monitor the use of Pheburane® on a named-patient basis. All treated UCD patients were included in a follow-up protocol developed by the Laboratory (Lucane Pharma) and the French Medicines Agency (ANSM), which recorded demographics, dosing characteristics of NaPB, concomitant medications, adverse events, and clinical outcome during the period of treatment. Following the granting of the Marketing Authorization in Europe, the cohort ATU was terminated approximately 1 year after its initiation, as the product was launched on the French market.
Results
The ease of administration and acceptability were much better with the new taste-masked formulation than with the previous treatment. No episodes of metabolic decompensation were observed over a treatment period ranging from 3 to 11 months with Pheburane® and the range of ammonia and glutamine plasma levels improved and remained within the normal range. In all, no adverse events were reported with Pheburane® treatment.
Conclusions
The recently developed taste-masked formulation of NaPB granules improved the quality of life for UCD patients. This may translate into improved compliance, efficacy, and safety, which may be demonstrated either in further studies or in the post-marketing use of the product.
Similar content being viewed by others


Sodium phenylbutyrate (NaPB) is a well known long-term treatment of urea cycle disease (UCD) |
NaPB has an offensive odor and taste which may compromise compliance |
Because of difficulty taking the active principle, patients are often administered the drug via nasogastric or gastrostomy tube |
Pheburane® is a new effective taste-masked presentation of NaPB |
This study reports the 1-year clinical experience of patients with UCD with a new tasteless formulation of NaPB in situ |
The experience is positive on efficacy and safety endpoints |
1 Introduction
It is evident that in rare disorders, new drugs not yet approved for marketing must be monitored for safety and effectiveness in the everyday clinical setting. The named patients programs, and in particular in France the cohort temporary utilization authorization (cohort ATU) program, serve this purpose. Sodium phenylbutyrate (NaPB), the unmodified active principle in Pheburane®, has been in clinical use for many years and its safety and efficacy as a waste nitrogen alternative to urea nitrogen in the treatment of urea cycle disorders is well established [1]. Other new derivatives with distinct pharmacological characteristics (e.g., glyceryl tributyrate) [2] have been developed to overcome the well known taste issue of NaPB. Our aim in this paper is to report the findings of a nationwide cohort ATU for patients with urea cycle disorders (UCD) treated with a tasteless formulation of NaPB, Pheburane®, between October 2012 and October 2013.
UCD are extremely rare inherited deficiencies of one of the enzymes involved in the cycle for the removal of nitrogen produced from protein breakdown. In France, the current estimate is approximately 40 patients under treatment with NaPB granules amongst a total of about 100 patients with UCD receiving NaPB. The pharmacological treatment of UCD centers on alternative nitrogen scavenging pathways where hippurate and phenylacetylglutamine, the respective metabolites of benzoate and NaPB, substitute to urea for waste nitrogen excretion [3]. Sodium phenylbutyrate has been used since 1987 as an investigational new drug (IND) and was approved for marketing in the US in 1996 and in the European Union in 1999. Two presentations (both uncoated) were available: 500 mg tablets and powder/granules 94 % w/w. It is well recognized that NaPB has a notoriously offensive taste [1, 4]. This has been confirmed by electronic tongue and real-time dissolution in vitro studies as well as by studies in healthy volunteers [5]. In September 2012, the French medicines agency (ANSM) granted a cohort ATU for a tasteless oral granule formulation of NaPB, Pheburane®, allowing its use in UCD patients who could not tolerate the marketed product due to its unpalatability. The pharmaceutical company (Lucane Pharma) had the opportunity to give input to and review the cohort ATU protocol. Pheburane® was granted market authorization in the EU on 31 July 2013 and the ANSM advised that the last date for inclusion in the cohort ATU should be 31 October 2013. Hence, the cohort ATU has spanned a period of 1 year.
2 Methods
2.1 Patient Inclusion
Inclusion of patients in the cohort ATU protocol required the diagnosis and treatment of UCD initiated by one of the national reference centers of inherited metabolic diseases. All patients with UCD are treated at a similar level of healthcare—by pediatrician specialists with knowledge in the management of UCD. The patient should have been previously treated with at least one oral nitrogen scavenger (NS). The NS could have been either the marketed NaPB medication or sodium benzoate. In the latter case, before being admitted to the cohort ATU protocol, administration of the marketed NaPB product had to be attempted.
2.2 Switch Protocol
If admitted, patients could then be switched from the product on the market to Pheburane®. No systematic examination was scheduled, patients being generally followed up at the reference center every 6 to 12 months. Because of the unscheduled follow-up, a possible a posteriori finding was that, in spite of a request for inclusion, patients (or their parents) had not complied with the cohort ATU.
Every patient was identifiable by a unique personal number issued by Lucane Pharma following the request for inclusion of the patient in the cohort ATU made by the treating physician together with the center’s pharmacist. Patients/parents were informed about this inclusion by their treating physician and all gave informed consent. Lucane Pharma’s registries and sharing of patients’ personal information were authorized by the ‘Commission Nationale Informatique et Libertés’ (CNIL, authorization no. 1603498 v 0).
Prior to the development of Pheburane, a survey was carried out in pediatric UCD patients receiving any of the marketed formulations of NaPB, as authorized by the CNIL (authorization no. DR-2012-505). This survey was aimed at the evaluation of the palatability and ease or difficulty of administration of the available medicine. The survey included patient/parent questionnaires, as well as patients’ taste evaluations if possible. Evaluations of the global acceptability of the taste were carried out using 100 mm-visual analog scales (VAS) after repeated intakes of the tested drug on 3 consecutive days. Some of the patients in this survey were subsequently included in the cohort ATU and the same evaluations of taste and global acceptability were repeated with the patients/parents when receiving Pheburane®. For the others, who generally tolerated the existing formulation(s) of NaPB, clinical information is also available and presented here. As the inclusion in the future cohort ATU was not pre-determined, these latter patients can be regarded as a control population. The present paper also reports some of the taste and safety data obtained during a study in healthy volunteers which established the bioequivalence of Pheburane® versus the granule formulation of NaPB available on the market, and has been previously reported [5]. In this cross-over study, a comparative taste evaluation was carried out using VAS ratings on global acceptance and three typical characteristics of the taste (i.e., bitterness, saltiness, and sweetness) which were repeated over three distinct time points: just after, 30 minutes after and 2 hours after a single 5 g oral dose of the study drug.
In the cohort ATU, data collection and reporting were compulsory for all prescribers following approval of inclusion by Lucane Pharma on behalf of the ANSM, confirming compliance with the cohort ATU protocol.
2.3 Outcome Measures
Assessment of effectiveness was established from the endpoints of acceptability, ease of administration of the product, ranges of biological values (ammonia, glutamine) and the number of hyperammonemia episodes.
The rating of acceptability (as well as that of bitterness and other taste characteristics cf. above) was measured on 100 mm-VAS in healthy volunteers. In each individual the difference in ratings following Pheburane® minus licensed product was calculated. In UCD patients, acceptability was one item of a questionnaire completed by the treating physician for inclusion of the patient in the cohort ATU. Moreover, patients who had previously taken part in the survey described above also repeated the questionnaire and the acceptability VAS on 3 consecutive days when receiving Pheburane®.
A combined parameter of ‘ease of administration’ took into account the need to reformulate the product and/or to mix the product with taste flavoring agents such as calomel syrup, and/or the need to use gastrostomy or nasogastric tube for all or some of the daily intakes in order to administer the product.
Finally, the numbers of episodes of hyperammonemia during the previous 6-month period when receiving the licensed NaPB formulation, compared with those reported for the longest period of follow-up available with Pheburane®, were recorded together with the respective ranges of laboratory values of ammonia and glutamine.
All patients recruited in the cohort ATU and all healthy volunteers participating in the bioequivalence study were included in the assessment of treatment safety. In the bioequivalence study, adverse events were coded according to the Medical Dictionary for Regulatory Activities (MedDRA), Version 13.0. Recorded adverse reactions with drug administration included, in particular, reports of taste disturbances (dysgeusia or ageusia) and/or of vomiting, regurgitation, or emesis at time of drug intake.
2.4 Statistical Analysis
The healthy volunteers’ taste assessments of the study products were compared using an analysis of variance with sequence, product, period, and product*period effects, using SAS/STAT® software with a two-sided 5 % significance level. For the cohort ATU, the cut-off date for the follow-up data was 31 December 2013, and mainly descriptive statistics were applied using Excel software; Wilcoxon’s tests were performed when appropriate.
3 Results
3.1 Acceptability of the Product in Comparison with that of the Marketed Product
Following a single 5 g oral dose, there was a dramatic increase in acceptability in 10 out of 13 healthy subjects (Fig. 1). Only one subject has no value having withdrawn from the study immediately after receiving the licensed product. The analysis of variance of the differences of the means was statistically significant (p < 0.05).

Differential (Pheburane®–marketed NaPB) individual rating of acceptability just after drug intake in healthy volunteers
From the mean (standard error [SE]) results of bitterness (the main taste characteristic of NaPB) and general acceptability (Fig. 2), it is clear that there was an inverse relationship between general acceptability and bitterness (correlation not tested). Mean acceptability increased by a factor of two. At the same time, mean perceived bitterness decreased by a factor of five.

Mean (SE) visual analogue scale ratings of acceptability and bitterness just after drug intake in healthy volunteers, and acceptability in urea cycle disorder (UCD) patients
The perception of taste characteristics of bitterness and saltiness was significantly lower (p < 0.05) just after the dose of Pheburane® than just after that of the licensed product. As expected, measurement of sweetness was the same with both products which indicates that the VAS was discriminatory. Scores of bitterness, sweetness, or saltiness at 30 minutes or at 2 hours after drug intake were not significantly different between each drug (data not shown).
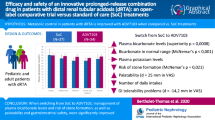
A total of 26 patients from nine centers were proposed for inclusion in the cohort ATU in order to receive Pheburane®. Of the 25 admitted (Table 1), 17 patients (70 %) were included during the first half of the year and 8 during the second half. Because of reluctance from their mother, two sisters who were requested cohort ATU treatment were in fact not treated in one and only for 1 week in the other. For an unknown reason, two siblings were not treated despite request for inclusion in the cohort ATU. Another patient was included in the cohort ATU but actually not treated because of a different appreciation of the actual need between treating physicians. Therefore follow-up data are available in a total of 20 patients, the majority (14) of whom have been switched from the NaPB granule formulation on the market. Another male patient presenting with a diagnosis of lysinuric protein intolerance (LPI), and aged only 1 week, was denied inclusion on safety grounds.
The UCD diagnoses included ornithine trans-carbamylase deficiency (15), arginosuccinate synthase deficiency (5), carbamoyl phosphate synthase type I deficiency (2), arginosuccinate lyase deficiency (1), hyperornithinemia-hyperammonemia-homocitrullinuria (1), and lysinuric protein intolerance (1). There was a majority of female patients (16). Clinical assessment at entry suggests that a subset of patients had severe illness while the others were mildly affected, with 7 patients presenting with neurologic impairment or epilepsy, 11 with developmental delay, 6 with liver impairment, and 20 acute hyperammonemic episodes in the 6 months before entering the cohort ATU in a total of 10 patients (rate ranging between one and three episodes/patient).
Pheburane® was given orally in all patients at doses between 1.5 and 15 g/day for 1–11 months; the mean (SD) daily dose was 5.2 (3.3) g corresponding to 211 (112) mg/kg at entry. The daily dose was administered in three or four intakes per day as recommended. Mean (SD) exposure to Pheburane® was 15.0 (8.5) patient-years, as compared with 50.9 (51.8) patient-years on marketed NaPB. Patients were receiving the same co-medication as before once treated with Pheburane®. Co-treatment was with benzoate (n = 15; mean [SE] dose = 5.7 [1.3] g/day), and/or citrulline (n = 11; 4.2 [1.3] g/day) and/or arginine (n = 12; 1.6 [0.3] g/day).
The main entry criterion into the cohort ATU was the unacceptability of the NaPB formulation(s) on the market. The patient could either not take the drug (even if reformulated) or required administration, for instance, via nasogastric tubing or gastrostomy. The reason why administration of the prescribed dose was limited was difficulty with the taste of NaPB. The marketed NaPB product was reported as unacceptable in all 25 ATU patients. Out of the 25 patients, four reported that it was totally impossible to take marketed NaPB and they were not treated with the latter product after a challenge test with the marketed product confirmed that these patients cannot accept it. A single patient out of 25 admitted to the cohort ATU reported difficulty with the granularity of Pheburane® on the first intake and suspended treatment; however, Pheburane® was secondarily resumed with no such further problem. After 6 months of inclusion, a single patient discontinued from the cohort ATU for a reported issue with granularity. Comparative data available from 9 UCD patients receiving doses of 2.5–10 g/day highlight a dramatic change in acceptability, even more pronounced than that in healthy volunteers (Fig. 2).
3.2 Ease of Administration
Before inclusion in the cohort ATU, when patients were receiving the licensed NaPB product, its administration required re-formulation into capsules (2/25), or through nasogastric tube (4/25) or gastrostomy (1/25). Conversely, no additional measure was required to administer Pheburane®, which is simply taken orally in all patients in the ATU follow-up (Table 2).
3.3 Number of Hyperammonemic Episodes
In the cohort ATU, the number of hyperammonemic episodes decreased from 20 reported in 10 patients in the previous 6 months under the licensed NaPB to zero in the same patients over a period of 3–11 months treatment with Pheburane® (Table 3). The group of patients that had not reported decompensations before Pheburane® did not have any decompensations since starting Pheburane® either. Moreover, the median ranges (IQR) of plasma ammonia (NH3) and glutamine (Gln) values were significantly lower after having switched from the NaPB on the market to Pheburane®, with values of 124 (68–221) and 1,027 (905–1310) vs 49 (39.5–54.5) and 845 (707–1075) (p = 0.019 and p = 0.028, Wilcoxon’s test), respectively, in 11 ATU patients with before/after measures of these biochemical parameters following 7 and 4 months’ treatment. As assessed by the maximal plasma ammonia and glutamine levels reported in the period before instauration of Pheburane® and during the follow-up under the drug, the metabolic control appears to be significantly improved with Pheburane® (Fig. 3).

Box–whisker plots of maximal plasma ammonia values in the 6-month period before inclusion in the cohort ATU and then under Pheburane®
3.4 Taste Disturbance and Vomiting
In the healthy volunteers study there were 5/14 reports of taste disturbance and 1/14 of severe vomiting after the marketed product compared with 0/13 after Pheburane® (one female subject dropped out immediately after severe vomiting following the marketed product during the first period of the trial).
In the ATU, no patient has reported any adverse event, notably no vomiting following administration of Pheburane® has been reported. This is in contrast to 4/25 patients complaining of vomiting reflexes when receiving marketed NaPB prior to entry into the cohort ATU.
4 Discussion
The new granule formulation of NaPB (Pheburane®) has been shown to be effectively taste-masked as demonstrated in vitro as well as in healthy volunteers [5, 6]. These studies confirmed that the coating on the Pheburane® granules was effective in preventing the active substance from interacting with the taste receptors before swallowing. As shown in three out of four control subjects not included in the cohort ATU (survey data not shown) with the use of crushed and/or encapsulated tablets, the historical product is acceptable as long as the daily dose is not too high and the age of the patient is compatible with swallowing tablet formulations. However, data from the cohort ATU in comparison with historical treatment characteristics indicate that the quality of life of UCD patients and their families has greatly improved with Pheburane® as assessed on the ease of administration of the drug and on the meaningfully reduced incidence of adverse events, notably vomiting and dysgeusia, which impair patients’ well-being and/or their acceptance/compliance with pharmaceutical treatments. Patients who cannot be treated with NaPB or had to use alternative methods (reformulation, nasogastric tube, and gastrostomy) were treated with Pheburane® in the cohort ATU without any problem, representing a dramatic improvement in the care and the ability to use the appropriate prescribed and registered medication (NaPB) for these children. The product was simply and normally taken by mouth in all patients in the cohort ATU follow-up as well as in 4/4 patients under other countries’ national named patient programs (data not shown). Safety of the drug is excellent as also confirmed from experience in other patients in Sweden and in Turkey (personal communication) who received Pheburane® under a named patients program prior to marketing approval.
It has been reported that taste disturbance is associated with oral ingestion of NaPB. This adverse event and vomiting associated with drug intake constitute unpleasant adverse events, and both are reported as ‘frequent’ in the Summary of Product Characteristics (SmPC) of NaPB [7]. Moreover, dysgeusia/ageusia can also compromise the flavor of food, an additional problem in a UCD patient where feeding is already very difficult due to restrictions in the diet and need for supplementation.
Dysgeusia or vomiting at drug intake occurs, as shown, even with single doses of NaPB. Other data supporting this fact include the report of vomiting at intake of licensed NaPB in one patient on a named patient program in Turkey [8], in one control patient not included in the cohort ATU (survey data not shown), as well as in one healthy volunteer [5]. The absence of such vomiting reflex following drug intake with Pheburane® obviates the need for re-dosing and therefore the risk of overdose, or the risk of under-dosing should the dose not be re-administered adequately. As a consequence, though this could not be demonstrated in the cohort ATU given the limited number of patients and duration, fewer adverse effects of over/under-dosing might be expected with Pheburane®.
Analysis of concomitant drug treatment showed a high proportion (~60 %) of sodium benzoate users. This may indicate that the NS treatment is carried out carefully by prescribing a low total daily dose of licensed NaPB that is bearable and actually approximately half that recommended in the SmPC as seen before [9], together with supplementation with benzoate. Whether the availability of a taste-masked formulation of NaPB translates into higher doses being able to be used and/or less use of benzoate could not be assessed in the present cohort ATU. The concomitant medications have not been modified in these 25 patients during the follow-up. Though 5/25 patients (20 %) were given a higher dose of Pheburane® than that of licensed NaPB or were dose-increased within the follow-up, it cannot be ascertained on such small numbers that this was due to the more acceptable formulation.
The magnitude of the clinical effectiveness in this nationwide pre-marketing cohort ATU program is similar to the efficacy reported in previous clinical studies. In seminal clinical trials of NS in UCD [10, 11] and other long-term retrospective studies in ornityltranscarbamylase deficiency (OTC) [12], surviving patients have presented intercurrent episodes of hyperammonemia. For instance, in a total of 97.6 patient-years of treatment (corresponding to IND phases involving the specific use of NaPB), a total of 70 episodes were reported in 25 patients [10]. On average, the surviving patients have had one episode per year; however, the mean was 2.8 episodes/patient (and 0.7 episode/patient-year) showing a wide variability in the frequency of episodes in individual arginosuccinate synthase deficiency patients, as also observed in OTC [11]. In recent studies, lower rates were reported, with 24 hyperammonemic crises in 15 patients in the year under sodium phenylbutyrate and 15 crises in 12 patients under glyceryl tributyrate [13]. In the cohort ATU, the number of hyperammonemic episodes decreased from 20 in 10 patients (mean [SE] = 0.9 [0.4] and range 1–3 episodes/patient) in the previous 6 months under the licensed NaPB—which corresponds to figures observed before [10, 11, 13]—to none over a period of 3–11 months’ treatment with Pheburane®. Though the cohort ATU protocol was not designed to collect any measurement of compliance or quality of life, the surrogate endpoint of decreased rate of hyperammonemic decompensations may indicate a better compliance and improved quality of life with Pheburane®, as also expected with other tasteless products [13, 14]. It is possible that due to their inability to tolerate NaPB, the patient cohort has been treated suboptimally prior to treatment with Pheburane®. Whether this is related to the product’s characteristics, notably its absence of taste at intake, or whether this is due to increased attention to dosing due to inclusion in the cohort ATU cannot be evaluated and warrants further studies.
References
Brusilow SW, Maestri NE. Urea cycle disorders: diagnosis, pathophysiology, and therapy. Adv Pediatr. 1996;43:127–70.
Lee B, Rhead W, Diaz GA, et al. Phase 2 comparison of a novel ammonia scavenging agent with sodium phenylbutyrate in patients with urea cycle disorders: safety, pharmacokinetics and ammonia control. Mol Genet Metab. 2010;100(3):221–8.
Brusilow W, Tinker J, Batshaw ML. Amino acid acylation: a mechanism of nitrogen excretion in inborn errors of urea synthesis. Science. 1980;207:659–61.
Dover GJ, Brusilow S, Charache S. Induction of fetal hemoglobin production in subjects with sickle cell anemia by oral sodium Phenylbutyrate. Blood. 1994;84(1):339–43.
Guffon N, Kibleur Y, Copalu W, et al. Developing a new formulation of sodium phenylbutyrate. Arch Dis Child. 2012;97:1081–5.
Rieder M. How sweet it isn’t: a new formulation of sodium phenylbutyrate and the challenge of palatability for medicines for children. Arch Dis Child. 2012;97(12):1080.
Summary of Product Characteristics, AMMONAPS® 940 mg/g granules, Swedish Orphan International AB, Sweden.
Kalkan-Uçar S, Atik-Altınok Y, Köse M, et al. A case report of the use of Pheburane in one argininosuccinic aciduria patient. SSIEM Barcelona 2013. P.
Dobbelaere D. European experience with sodium phenylbutyrate: a new treatment paradigm. Swedish Orphan International AB, Sweden. Urea Cycle Disorders Symposium. Barcelona. January 2007.
Maestri NE, Clissold DB, Brusilow SW. Long-term survival of patients with argininosuccinate synthetase deficiency. J Pediatr. 1995;127(6):929–35.
Maestri NE, Brusilow SW, Clissold DB, et al. Long-term treatment of girls with ornithine transcarbamylase deficiency. N Engl J Med. 1996;335(12):855–9.
Burlina AB, Ogier H, Korall H, et al. Long-term treatment with sodium phenylbutyrate in ornithine transcarbamylase-deficient patients. Mol Genet Metab. 2001;72(4):351–5.
Diaz GA, Krivitzky LS, Mokhtarani M, et al. Ammonia control and neurocognitive outcome among urea cycle disorder patients treated with glycerol phenylbutyrate. Hepatology. 2013;57(6):2171–9.
Cederbaum S, Lemons C, Batshaw ML. Alternative pathway or diversion therapy for urea cycle disorders now and in the future. Mol Genet Metab. 2010;100(3):219–20.
Competing interests
YK is the medical director at Lucane Pharma, the marketing authorization holder for Pheburane®. None of the other authors (DD, MB, AB, and NG) have any competing interest.
Funding: this work received no specific grant from any funding agency in the public, commercial or not-for-profit sector.
All authors made substantial contributions to the acquisition and interpretation of data for the work, revised the manuscript critically, agreed to give final approval of the version to be published, and are in agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Kibleur, Y., Dobbelaere, D., Barth, M. et al. Results from a Nationwide Cohort Temporary Utilization Authorization (ATU) Survey of Patients in France Treated with Pheburane® (Sodium Phenylbutyrate) Taste-Masked Granules. Pediatr Drugs 16, 407–415 (2014). https://doi.org/10.1007/s40272-014-0081-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40272-014-0081-5