
Abstract
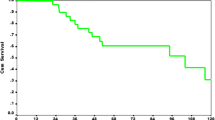
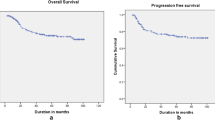
Cervical cancer usually presents in advanced stages and is treated with chemoradiation. About 15–20 % patients present with local recurrence after chemoradiation. Radical surgical resection is the only treatment modality offering long term survival benefit in recurrent cervical cancer. The most common surgical option for these patients is pelvic exenteration. Radical hysterectomy may be done for patients with a small centrally located recurrence in the cervix with no infiltration of adjacent structures. The aim of this study was to evaluate the morbidity and survival outcome following radical hysterectomy and pelvic exenteration for recurrent cancer cervix. We retrospectively reviewed the medical records of our patients who underwent surgery for cancer cervix recurrence from January 2010 to December 2014. The postoperative morbidity was considered early if it happened in the initial 30 days of surgery and late if it occurred after 30 days. All patients were followed up till February 2015. Survival analysis was done using Kaplan- Meir method. Between January 2010 and December 2014, 20 patients with recurrent cervical cancer underwent radical surgical resection. The median age of the study group was 43 years (range 28–63 years). Seventeen patients had squamous cell carcinoma and 3 had adenocarcinoma. 13 underwent pelvic exenteration and 7 patients underwent radical type 2 hysterectomy with bilateral pelvic lymphnode dissection. In the exenteration group, 8 patients had anterior exenteration, 4 had total exenteration and one had posterior exenteration. Urinary diversion was done by ileal conduit in 8 patients, double barrel colostomy in two and wet colostomy in two patients. There were no immediate postoperative deaths. Operating time, blood transfusions needed and hospital stay was more in the exenteration group compared to radical hysterectomy patients. After pelvic exenteration post-operative complications were seen in 76.9 % of which the most common was of the urinary tract including 3 patients with pyelonephritis, 5 had renal insufficiency and 2 patients developed urinary fistulae. Post-operative morbidity was lower in radical hysterectomy patients. There were two patients in the hysterectomy group who developed vault recurrence while none in the exenteration group had local recurrence. The median follow up time was 19 months (range 9–53 months).Three year overall survival for the entire cohort was 43 %. Median survival time for the exenteration group was 28 months which was significantly higher than 14 months for the radical hysterectomy group. This study shows that radical surgical resection is feasible with good survival outcome and acceptable morbidity in recurrent cancer cervix patients. Radical hysterectomy can be done in selected patients but pelvic exenteration has better long-term survival but with the potential for both short- & long-term complications.


Similar content being viewed by others

References
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM (2010) Esti-mates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127:2893–2917
Chiva LM, Lapuente F, Cortijio LG, Martin AG, Rojo A, Gracia JF, et al. (2008) Surgical treatment of recurrent cervical cancer: state of the art and new achievements. Gynecol Oncol 110:S60–S66
Hong JH, Tsai CS, Lai CH, Chang TC, Wang CC, Chou HH, et al. (2004) Recurrent squamous cell carcinoma after definitive radiotherapy. Int J Radiat Oncol Biol Phys 60:249–257
Cardon I, Van Gorp T, Amat F, Leunen K, Neven P, Vergot I (2007) Chemotherapy for recurrent cervical cancer. Gynecol Oncol 107(1):S113–S118
Gadducci A, Tana R, Cosio S, Cionini L (2010) treatment options in recurrent cervical cancer (review). Oncol Lett 1:3–11
Landoni F, Maneo A, Colombo A, et al. (1997) Randomised study of radical surgery versus radiotherapy for stage ib-iia cervical cancer. Lancet 350:535–540
Kasamatsu T, Onda T, Yamada T, Tsunematsu R (2005) Clinical aspects and prognosis of pelvic recurrence of cervical carcinoma. Int J Gynecol Obstet 89:39–44
Brunschwig A. Complete excision of pelvic viscera for advanced carcinoma. Cancer 1948;1:177–183.
Pawlik TM, Skibber JM, Rodriguez-Bigas MA (2006) Pelvic exenteration for advanced pelvic malignancies. Ann Surg Oncol 13:612–623
Hockel M, Dornhofer N (2006) Pelvic Exenteration for Gynaecological Tumours: Achievements and Unanswered Questions. Lancet Oncol 7:837–847
Peiretti M, Zapardiel I, Zanagnolo V, Landoni F, Morrow CP, Maggioni A (2012) Management of recurrent cervical cancer: a review of the literature. Surg Oncol 21:e59–e66
Goldberg GL, Sukumvanich P, Einstein MH, Smith HO, Anderson PS, Fields AL (2006) Total pelvic exenteration: the albert einstein college of medicine montefiore medical center experience (1987 to 2003). Gynecol Oncol 101:261–268
Sharma S, Odunsi K, Driscoll D, Lele S (2005) Pelvic exenterations for gynecological malignancies: twenty-year experience at roswell park cancer institute. Int J Gynecol Cancer 15:475–482
Berek JS, Howe C, Lagasse LD, Hacker NF (2005) Pelvic exenteration for recurrent gynecologic malignancy: survival and morbidity analysis of the 45-year experience at UCLA. Gynecol Oncol 99:153–159
Pawlik TM, Skibber JM, Rodriguez-Bigas MA (2006) pelvic exenteration for advanced pelvic malignancies ann. Surg Oncol 13:612–623
Höckel M (2006) Ultra-radical compartmentalized surgery in gynaecological oncology. Eur J Surg Oncol 32:859–865
Terán-Porcayo MA, Zeichner-Gancz I, Gomez del-Castillo RAC, Beltrán-Ortega A, Solorza-Luna G (2006) “Pelvic exenteration for recurrent or persistent cervical cancer,”. Med Oncol 23(2):219–223
Maneo A, Landoni F, Cormio G, Colombo A, Mangioni C (1999) Radical hysterectomy for recurrent or persistent cervical cancer following radiation therapy. Int J Gyne col Cancer 9(4):295–301
R Ramamurthy, A Duraipandian, Morbidity and outcome of pelvic exenteration in locally advanced pelvic malignancies. Indian J Surg Oncol. 2012; 3(3): 231–235
Pandey D, Zaidi S, Mahajan V, Kannan R (2004) Pelvic exenteration: a perspective from a regional cancer center in India. Indian J Cancer 41(3):109–114
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Rema, P., Mathew, A.P., Suchetha, S. et al. Salvage Surgery for Cervical Cancer Recurrences. Indian J Surg Oncol 8, 146–149 (2017). https://doi.org/10.1007/s13193-015-0472-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13193-015-0472-2