
Abstract
Background
Immunosuppression is used to treat cardiac sarcoidosis, despite limited data. FDG PET/CT is used for detecting cardiac inflammation in patients with CS, yet there is variability in interpretation of FDG PET/CT. Our aim was to compare quantitative and qualitative interpretation of FDG PET/CT for CS in defining the FDG response to immunosuppression.
Methods and Results
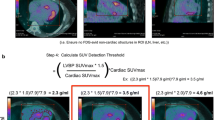
Patients with CS (N = 43 total studies from 17 patients) had serial FDG PET/CT studies before/after immunosuppression. FDG uptake was analyzed qualitatively (visually; FDG-positive segments) and quantitatively (SUVmax; cardiac metabolic volume and activity (CMV, CMA); volume above SUV thresholds 2.7 and 4.1 g/mL). Complete resolution of FDG uptake was common using CMA (10/17), CMV (10/17), but a 2.7 g/mL SUV threshold (13/17) and SUVmax (14/17) were more likely to define partial responses. In six patients imaged after a reduction in immunosuppression, 4/6 had a rebound quantitative FDG uptake.
Conclusions
Quantitative interpretation of FDG PET/CT in CS can detect changes in FDG uptake in response to immunosuppression. Further studies are needed to see if quantitative changes in FDG uptake are associated with improved outcomes.





Similar content being viewed by others

Abbreviations
- CS:
-
Cardiac sarcoidosis
- CMA:
-
Cardiac metabolic activity
- CMV:
-
Cardiac metabolic volume
- FDG:
-
Fluorodeoxyglucose
- PET:
-
Positron emission tomography
- SUV:
-
Standardized uptake values
References
Hamzeh N, Steckman DA, Sauer WH, Judson MA. Pathophysiology and clinical management of cardiac sarcoidosis. Nat Rev Cardiol 201. doi:10.1038/nrcardio.2015.22.
Sadek MM, Yung D, Birnie DH, Beanlands RS, Nery PB. Corticosteroid therapy for cardiac sarcoidosis: A systematic review. Can J Cardiol 2013;29:1034–41. doi:10.1016/j.cjca.2013.02.004.
Ohira H, Birnie DH, Pena E, Bernick J, Mc Ardle B, Leung E, et al. Comparison of 18F-fluorodeoxyglucose positron emission tomography (FDG PET) and cardiac magnetic resonance (CMR) in corticosteroid-naive patients with conduction system disease due to cardiac sarcoidosis. Eur J Nucl Med Mol Imaging 2015. doi:10.1007/s00259-015-3181-8.
Orii M, Hirata K, Tanimoto T, Ota S, Shiono Y, Yamano T, et al. Comparison of cardiac MRI and 18F-FDG positron emission tomography manifestations and regional response to corticosteroid therapy in newly diagnosed cardiac sarcoidosis with complete heart block. Heart Rhythm 2015. doi:10.1016/j.hrthm.2015.06.032.
Birnie DH, Sauer WH, Bogun F, Cooper JM, Culver DA, Duvernoy CS, et al. HRS expert consensus statement on the diagnosis and management of arrhythmias associated with cardiac sarcoidosis. Heart Rhythm 2014. doi:10.1016/j.hrthm.2014.03.043.
Hamzeh NY. Management of cardiac sarcoidosis in the United States. Chest 2012;141:154–9. doi:10.1378/chest.11-0263.
Ahmadian A, Brogan A, Berman J, Sverdlov AL, Mercier G, Mazzini M, et al. Quantitative interpretation of FDG PET/CT with myocardial perfusion imaging increases diagnostic information in the evaluation of cardiac sarcoidosis. J Nucl Cardiol 2014. doi:10.1007/s12350-014-9901-9.
Blankstein R, Osborne M, Naya M, Waller A, Kim CK, Murthy VL, et al. Cardiac positron emission tomography enhances prognostic assessments of patients with suspected cardiac sarcoidosis. J Am Coll Cardiol 2014;63:329–36. doi:10.1016/j.jacc.2013.09.022.
Yamagishi H, Shirai N, Takagi M, Yoshiyama M, Akioka K, Takeuchi K, et al. Identification of cardiac sarcoidosis with (13)N-NH(3)/(18)F-FDG PET. J Nucl Med 2003;44:1030–6.
Waller AH, Blankstein R. Quantifying myocardial inflammation using F18-fluorodeoxyglucose positron emission tomography in cardiac sarcoidosis. J Nucl Cardiol 2014. doi:10.1007/s12350-014-9921-5.
Okumura W, Iwasaki T, Toyama T, Iso T, Arai T, Oriuchi N, et al. Usefulness of fasting 18F-FDG PET in identification of cardiac sarcoidosis. J Nucl Med 2004;45:1989–98.
Mc Ardle BA, Birnie DH, Klein R, de Kemp RA, Leung E, Renaud J, et al. Is there an association between clinical presentation and the location and extent of myocardial involvement of cardiac sarcoidosis as assessed by 18F- fluorodoexyglucose positron emission tomography? Circ Cardiovasc Imaging 2013;6:617–26. doi:10.1161/CIRCIMAGING.112.000289.
Tahara N, Tahara A, Nitta Y, Kodama N, Mizoguchi M, Kaida H, et al. Heterogeneous myocardial FDG uptake and the disease activity in cardiac sarcoidosis. JACC Cardiovasc Imaging 2010;3:1219–28. doi:10.1016/j.jcmg.2010.09.015.
Osborne MT, Hulten EA, Singh A, Waller AH, Bittencourt MS, Stewart GC, et al. Reduction in 18F-fluorodeoxyglucose uptake on serial cardiac positron emission tomography is associated with improved left ventricular ejection fraction in patients with cardiac sarcoidosis. J Nucl Cardiol 2013. doi:10.1007/s12350-013-9828-6.
Ishimaru S, Tsujino I, Takei T, Tsukamoto E, Sakaue S, Kamigaki M, et al. Focal uptake on 18F-fluoro-2-deoxyglucose positron emission tomography images indicates cardiac involvement of sarcoidosis. Eur Heart J 2005;26:1538–43. doi:10.1093/eurheartj/ehi180.
Rist RJ, Naftalin RJ. Dexamethasone inhibits the hexose monophosphate shunt in activated rat peritoneal macrophages by reducing hexokinase-dependent sugar uptake. Biochem J 1991;278:129–35.
Norton JM, Munck A. In vitro actions of glucocorticoids on murine macrophages: Effects on glucose transport and metabolism, growth in culture, and protein synthesis. J Immunol 1980;125:259–66.
Relationship with industry
Dr Miller has consulting relationships with GE, Inc. and Bracco, Inc and research funding from Bracco, Inc., which are unrelated to the current study.
Disclosure
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
See related editorial, doi:10.1007/s12350-016-0624-y.
Rights and permissions
About this article

Cite this article
Ahmadian, A., Pawar, S., Govender, P. et al. The response of FDG uptake to immunosuppressive treatment on FDG PET/CT imaging for cardiac sarcoidosis. J. Nucl. Cardiol. 24, 413–424 (2017). https://doi.org/10.1007/s12350-016-0490-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-016-0490-7