
Abstract
Purpose
Left ventricular (LV) phase dyssynchrony parameters based on gated myocardial perfusion imaging varied among software programs. The aim of this study was to determine normal ranges and factors affecting phase parameters.
Methods
Normal databases were derived from the Japanese Society of Nuclear Medicine working group (n = 69). The programs were Emory Cardiac Toolbox with SyncTool (ECTb), Quantitative Gated SPECT (QGS), Heart Function View (HFV), and cardioREPO (cREPO); parameters of phase standard deviation (PSD), 95% bandwidth, and entropy were compared with parameters with ECTb as a reference.
Results
PSD (degree) was 5.3 ± 3.3 for QGS (P < .0001), 5.4 ± 2.5 for HFV (P < .0001), and 10.3 ± 3.2 for cREPO (P = n. s.) compared with 11.5 ± 5.5 for ECTb. Phase bandwidth with three programs differed significantly from ECTb. Gender differences were significant for all programs, indicating larger variation in males. After adjustment of LV volumes between genders, the difference disappeared except for QGS. The phase parameters showed wider variations in patients with the lower ejection fraction (EF) and larger LV volumes, depending on software types.
Conclusion
Based on normal ranges of phase dyssynchrony parameters in four software programs, dependency on genders, LV volume, and EF should be considered, indicating the need for careful comparison among different software programs.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In nuclear cardiology, phase analysis of timing of contraction has been used since the 1980s in a gated blood-pool study.1 Fourier analysis of pixel-based time-activity curves provided phase and amplitude of the fundamental frequency, and it has been used for quantifying regional ventricular wall motion.2,3 Using a combination of phase and amplitude, hypokinesis was defined as decreased amplitude with a normal phase, akinesis as severely reduced (nearly zero) amplitude, and dyskinesis as delayed phase. In addition, phase propagation sequence analysis in conditions such as bundle branch block, ventricular pacing, and pre-excitation syndromes can be characterized by the specific propagation patterns of phases in both ventricles in planar and tomographic studies.4-7 However, after the advent of gated myocardial perfusion imaging (MPI) along with quantitative gated single-photon emission computed tomography (SPECT) software as Quantitative Gated SPECT (QGS; Cedars Sinai Medical Center, USA) and Emory Cardiac Toolbox (ECTb, Emory University, USA),8,9 the use of gated blood-pool studies was decreased and the phase analysis lost its popularity. ECTb-SyncTool (Syntermed, USA) successfully used phase analysis in gated SPECT studies as commercially available software.10
Since several software packages are now available in Japan, the purpose of this study was to determine the normal values of each software program, including cardioREPO (cREPO; FUJIFILM RI Pharma, Tokyo, Japan; collaboration with EXINI Diagnostics, Lund, Sweden) and Heart Function View (HFV; Nihon Medi-Physics, Tokyo, Japan) in comparison with ECTb. The normal database was prepared from the Japanese Society of Nuclear Medicine (JSNM) working group database 2007.11,12
Methods
Databases Used for the Analysis
The JSNM working group created normal databases for MPI in 2007, and the electrocardiographic gated 99mTc-methoxy-isobutylisonitrile (MIBI) or 99mTc-tetrofosmin studies at resting condition with 16 frames per cardiac cycle were used.11 A standard dose of 555 to 925 MBq in Japan was used in all institutions. A total of 69 datasets were available from the database (36 male and 33 female subjects), which were obtained by rotating Anger camera system. All the patients showed no perfusion defect as assessed by visual and quantitative scoring with summed score of ≤3 with a 17-segment 5-point (0-4) model. The databases included subjects without underlying cardiac diseases and no medications for diabetes and hypertension. Subjects with inappropriate arrhythmia for gating and wall motion abnormality were excluded. Mean age was 56 ± 13 years including 36 male and 33 female subjects. Body mass index was 22.5 ± 2.6 and 22.7 ± 2.7 for male and female subjects, respectively. All the images were 64 × 64 matrices and acquired with either 180° or 360° rotation. The databases were prepared as a short-axis image set of gated and non-gated data. The gated short-axis images at rest showed sufficient maximum myocardial count of 123 ± 64 counts/pixel. No study showed visual flickering of the data due to count drop of the last frames. The reconstruction parameters for MPI were standardized as described elsewhere.11 All the MPI data were reconstructed by the filtered back-projection method. Neither attenuation correction nor scatter correction was used.
Left Ventricular (LV) Ejection Fraction (EF) and Volumes for Gated SPECT Study
Parameters for baseline cardiac function included left LVEF, end-diastolic volume (EDV), and end-systolic volume (ESV). All the analyses were performed using standard software settings of ECTb, QGS, HFV, and cREPO. Regarding ventricular edge detection, ECTb used an anatomically based 3-dimensional model for ventricular edge detection assuming that at end-diastole, LV myocardial thickness is 1 cm.9,13 QGS software used an ellipsoid shape and iterative process to fit the myocardial walls.8,14 The algorithm of HFV used the “modified threshold method”,15 and the method of cREPO based on the active-shape model.16,17 All of these processing algorithms were specifically developed and refined thereafter.13,14 Software versions used in this study were version 2008 for QGS, version 3.2 for ECTb, version 1.0 for cREPO, and version 1.1 for HFV.
Dyssynchrony Analysis
Fourier analysis was applied to extract the phase and amplitude of the fundamental frequency of the regional time-activity curves.1,18 In gated MPI, the activity change reflects wall thickening during a cardiac cycle due to partial volume effects. Although the precise algorithm for calculating regional curves and segmentation differed among software programs, the following parameters have been commonly used. The phase value was defined as an amount of shift of sine (or cosine) curves using the fundamental frequency of the Fourier fitting (Fig. 1A), and a phase histogram was created to see the distribution pattern of phase values. Based on the histogram analysis, standard deviation of the phase (PSD, unit: degree) and 95% width of the histogram or bandwidth (unit: degree) were calculated (Fig. 1B). Entropy is an index of “disorder” defined by summation of [f i *log(f i )]/Log(n)], where f and n are frequency in the i th bin and number of bins, respectively.19,20 The entropy shows a range of 0-1 (0-100%), corresponding to complete order to disorder. All the analyses were performed automatically at first, and when statistical noise was included in the basal part of the phase polar map, manual adjustment of the base was added. Phase map smoothing function was used for ECTb, and basal circular removal function was used for cREPO when they were required. Minor manual adjustment of the basal border was performed in <10% of the patients for QGS, cREPO, and HFV, and ~30% for ECTb.

Parameters calculated with gated SPECT study. A phase value is calculated based on original data points (A). A histogram is created to obtain PSD and 95% bandwidth (B). Septal and lateral segments are shown to calculate variations of time to end-systole (C)
In addition, cREPO provided 17-segment-based regional time-activity curves and its regional variations similar to the “cardioGRAF” software (FUJIFILM RI Pharma, Co. Ltd, Japan), which has been used for heart failure and resynchronization therapy.21,22 After calculating regional counts in each segment, 17 time-activity curves were created to calculate time to the end-systolic frame (TES, unit: degree) using the fundamental wave plus the second harmonic component. The maximum difference among segmental TES (MDTES: unit, %) was calculated after division by 360°. The standard deviation of TES (SDTES) was also calculated (unit, %). The difference of TES between the lateral segment (average of anterolateral and inferolateral segments) and the septum (average of anteroseptal and inferoseptal segments) (DTES-LS: unit, %) was calculated (Fig. 1C).
Statistical Analysis
All the data are expressed as mean and standard deviation (SD). Mean values were compared by the analysis of variance. Scatterplot matrix was calculated for all combinations of the four software programs, and pairwise correlation coefficients and p values were calculated. Gender difference was also calculated for all phase parameters. Linear regression line was calculated with the least square method. To compare parameters for gender differences in the small and larger LV, non-parametric Wilcoxon test was used for the four groups, and only males with the smaller LV and females with the larger LV were compared. Statistical analysis was performed using JMP 10.0 software (SAS Institute Inc., Cary, NC, USA). A P value <.05 was considered significant.
Results
The mean EF was 69.2 ± 6.5%, 77.1 ± 6.3%, 73.2 ± 5.3%, and 71.7 ± 6.4% for QGS, ECTb, cREPO, and HFV, respectively (Table 1). Both EDV and ESV were the highest in cREPO. For all pairwise comparisons of EF, the correlation coefficient ranged from 0.53 (QGS vs cREPO) to 0.76 (HFV vs cREPO) (P < .0001 for all combinations).
Regarding phase parameters (Table 2), the bandwidth was the highest in cREPO, followed by ECTb, QGS, and HFV (P < .0001 vs ECTb for all). The PSD was comparable for ECTb and cREPO (P = n. s.), which was higher than that of QGS (P < .0001) and HFV (P < .0001). Phase entropy was higher in cREPO than that in QGS (P < .0001).
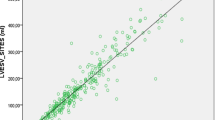
When pairwise comparison was performed for the phase bandwidth, significant correlation was observed between ECTb and cREPO [r = 0.38, 95% confidence interval (CI) = 0.16-0.57, P = .0012] (Fig. 2C), and between cREPO and HFV (r = 0.33, CI 0.10-0.52, P = .0063) (Fig. 3A). Similarly, for PSD, significant correlation was observed between cREPO and HFV (r = 0.36, CI 0.13-0.55, P = .0027) (Fig. 3B). The phase entropy showed significant correlation between QGS and cREPO (r = 0.39, CI 0.17-0.58, P = .0008) (Fig. 3C). Other combinations did not show significant correlation, since all values were in normal ranges.

Relationship of phase bandwidth and PSD compared with those with ECTb. Upper panels show bandwidth in QGS, HFV, and cREPO vs ECTb. Lower panels show PSD between two software programs. The linear regression equation is written when the P value is <.10. The shaded area indicates confidence limits for the regression line. Red circles and blue squares denote male and female data points, respectively

Relationship of phase bandwidth, PSD, and phase entropy between two software programs. Panels (A) and (B) show bandwidth and PSD for HFV vs cREPO, and panel ( C) shows phase entropy for QGS vs cREPO. Marks and lines are the same as in Fig. 2
Gender difference of phase parameters was significant, and male subjects showed larger phase deviations (Table 3). In the phase bandwidth, QGS, cREPO, and HFV showed higher values in males than in females (P = .0014-.010), and ECTb also showed higher tendency in males (P = .078). The PSD was consistently higher (P = .002-.043) in males than in females. The phase entropy parameter was also higher in males, indicating larger disorder in the male database (P < .0001). When phase bandwidth and PSD were plotted versus EDV, positive correlations were obtained for QGS, HFV, and cREPO (Fig. 4). The relationship between phase parameters and LVEF was examined. Regarding phase bandwidth, significant correlation with LVEF was observed in QGS (r = −0.46, P < .0001) and HFV (r = −0.55, P < .0001). The relationship between PSD and LVEF showed that correlation coefficients ranged from −0.24 to −0.53 (P < .0001 to .048) (Fig. 5). Phase entropy and LVEF showed negative correlation: −0.44 (P = .0002) in QGS and −0.31 (P = .009) in cREPO. However, the relationship between phase parameters and body weight were not significant in all software programs. Parameters of TES using a 17-segment model were given only with cREPO (Table 4). Although the values were slightly higher in males, no significant gender difference was observed.

Relationship between EDV and PSD using ECTb (A), QGS (B), HFV (C), and cREPO (D). The shaded area indicates confidence limits for the regression line. Marks and lines are the same as in Fig. 2

Relationship between LVEF and PSD using ECTb (A), QGS (B), HFV (C), and cREPO (D). The marks and lines are the same as in Fig. 2
To evaluate the effect of small hearts on phase parameters, male subjects with the lower LV volume (EDV <85 mL, median value) and female subjects with the higher LV volumes (EDV ≥65 mL, median value) were compared (Table 5). Although both EDV and EF calculated by QGS software did not differ significantly, PSD (P = .040) and entropy (P = .020) showed significant difference between genders with QGS. A slightly higher tendency (P = .05 to .010) was observed in males than females regarding PSD by ECTb, bandwidth by QGS, and bandwidth and PSD by HFV.
Discussion
When Fourier phase analysis has been used in gated myocardial SPECT studies, it has been noticed that normal values depended on the technology of data acquisition and processing as well as software algorithms. Since new software, namely, cREPO and HFV has been available in Japan, normal values based on JSNM working group databases are presented and compared with more commonly used software of ECTb and QGS. In this comparative study of normal values, phase parameters differ significantly among software programs and are not considered to be interchangeable. Both phase bandwidth and PSD were higher in ECTb and cREPO than in QGS and HFV. Gender differences and dependency on the LV volume and LVEF should also be considered for clinical applications.
Phase analysis was developed in the 1980s and has been used in gated blood-pool study and subsequently in gated SPECT. Initial applications were to detect ventricular asynergy and conduction abnormalities including bundle branch block and pre-excitation syndrome.1-3,5,7 However, Fourier phase analysis has been used for gated MPI, which used regional myocardial count. The difference in these methods is that the blood-pool phase analysis yields insight into wall motion, while MPI phase analysis focuses on the timing and amplitude of wall thickening or count changes. Chen and Garcia developed the first successful software, and the results have been found to be promising in LV mechanical dyssynchrony analysis and cardiac resynchronization therapy (CRT).10,18 Similar software for dyssynchrony analysis has also been developed in Japan using segmental regional variation of TES, which showed that the combined use of regional variation of contraction timing and perfusion in the inferolateral segments was useful for evaluating the effect of CRT.15,21 The phase analysis was also applicable for evaluating multi-vessel disease and ischemic and non-ischemic etiologies with stress MPI.23,24
Several dyssynchrony parameters have been proposed. Although the distribution of phase values is nearly symmetrical in normal subjects, it is not a simple Gaussian distribution in patients with dyssynchrony. PSD may not be appropriate for characterizing the widely distributed and sometimes multi-modal distributions in phase histograms. The 95% bandwidth includes nearly a whole range of histogram distribution by excluding possible outlier phase values, and it has worked well in a number of studies. Therefore, we compared these common parameters of PSD and 95% bandwidth in the four software programs. The entropy, which is defined as a term of physics, was considered to be a promising parameter in gated blood-pool study for indication of CRT.19 Random distribution in the dilated left ventricle with reduced contractility, which cannot be reflected by simple PSD and bandwidth, may fit the use of entropy.
The fair correlation among software programs was apparently due to narrow range of distribution, since only functionally normal patients were included. If abnormal patients with LV dyssynchrony were included, correlation coefficient would be calculated as higher. Therefore, we cannot directly apply the linear regression equations that were presented in this study for converting the phase values in the patient population including the abnormal phase. The reliability of phase and cross-calibration between software types should be evaluated by including a large number of abnormal patients. Moreover, the normal upper limit should not be used to indicate the optimal threshold for resynchronization, because the cutoff point for predicting good response to CRT was higher, for example 135 degrees for histogram bandwidth and 43 degrees for PSD by ECTb.25
Several factors may influence the distribution of phase depending on gender, total accumulated count or noise, amount of injected radionuclide, stress or rest, and number of frames per cardiac cycle. The perfusion pattern in addition to post-stress and resting conditions were also determinants of phase values.26 Interestingly, all phase parameters showed the higher variation in male subjects, which has been also presented by an American population, showing 38.7 ± 11.8° and 30.6 ± 9.6° for bandwidth in males and females, respectively, and 14.2 ± 5.1° and 11.8 ± 5.2° for PSD.18 The reason may be related to myocardial count accumulated in various sizes of the heart. If the total injection dose was similar, the larger heart might have accumulated less myocardial count per myocardium volume (count/cm3). When the same acquisition and processing filters were applied in both genders, the overall effects may become smoother images in the female condition. Phase parameters showed larger variation in patients with either lower LVEF or larger LV volumes in four software programs. The difference in phase parameters became smaller between genders after adjustment of volumes, but a slight difference still remained. Generally, the higher exercise level in male subjects than in female subjects may also be a concern. Physiologically, it is not a plausible explanation that male hearts contract more dyssynchronously and disorderly than female hearts, but the gender difference actually existed in the routine acquisition and processing conditions.
Based on the results of this study, phase parameters cannot be interchangeably used among four software programs. However, when we analyzed normal values, there seem to be similarities between ECTb and cREPO, and between QGS and HFV. The ventricular models used for detecting myocardial walls significantly influence EF and volumes as well as measured pixel-based counts. The calculated phase parameters might have been influenced by the count detection algorithm on the myocardial walls, filtering of the images, number of angular sampling, filtering of time-activity curves, and so on. In general, images with smoothing or low-pass filtering, either temporal or spatial domain, result in the lower noise and hence the smaller bandwidth and PSD. Although we could not strictly define the effect confounding factors on phase values in each software program, we should carefully deal with the differences in software in clinical applications.
There are some limitations in this study. Since the JSNM working group database was prepared as the short-axis images from multiple institutions, we could not strictly define acquisition and processing conditions. However, the database reflects clinically acceptable image quality with optimal gating, and the selection criteria of the normal database were clearly defined.11,12 Since Anger camera images without attenuation correction and filtered back-projection reconstruction were used, currently used computed tomography-based attenuation correction images and new equipment such as D-SPECT could not be included. In this study, we cannot evaluate all the related factors, as the number of patients was limited in the database. Since the JSNM working group is collecting a larger number of normal databases at present, more precise analysis is indicated using the revised databases and by including diseased patients who showed abnormality in phase distribution.
New Knowledge Gained
All normal values for phase dyssynchrony with currently available software programs were given in this study. Phase analysis parameters derived from MPI depend on software programs, due to their specific algorithms for calculating phase bandwidth, PSD, and entropy. Gender differences were observed in all software programs, and the values showed higher variations in males than in females and, in addition, in patients with the larger LV volumes and the lower LVEF. Although the results of phase analysis cannot be interchangeably used in the same subjects, such dependency on gender and functional conditions should be considered.
Abbreviations
- ECTb:
-
Emory Cardiac Toolbox
- QGS:
-
Quantitative Gated SPECT
- HFV:
-
Heart Function View
- cREPO:
-
cardioREPO
- LV:
-
Left ventricle
- PSD:
-
Phase standard deviation
- EF:
-
Ejection fraction
- EDV:
-
End-diastolic volume
- ESV:
-
End-systolic volume
- TES:
-
Time to end-systole
References
Links JM, Douglass KH, Wagner HN Jr. Patterns of ventricular emptying by Fourier analysis of gated blood-pool studies. J Nucl Med 1980;21:978-82.
Brateman L, Buckley K, Keim SG, Wargovich TJ, Williams CM. Left ventricular regional wall motion assessment by radionuclide ventriculography: A comparison of cine display with Fourier imaging. J Nucl Med 1991;32:777-82.
Adachi I, Akagi H, Umeda T, Suwa M, Komori T, Ogura Y, et al. Gated blood pool SPECT improves reproducibility of right and left ventricular Fourier phase analysis in radionuclide angiography. Ann Nucl Med 2003;17:711-6.
Nakajima K, Bunko H, Tada A, Tonami N, Hisada K, Misaki T, et al. Nuclear tomographic phase analysis: Localization of accessory conduction pathway in patients with Wolff-Parkinson-White syndrome. Am Heart J 1985;109:809-15.
Nakajima K, Bunko H, Tonami N, Taki J, Nanbu I, Shiire Y, et al. Length-based Fourier analysis in the pre-excitation syndrome. J Nucl Med 1986;27:1131-7.
Muramatsu T, Matsumoto K, Nishimura S. Efficacy of the phase images in Fourier analysis using gated cardiac POOL-SPECT for determining the indication for cardiac resynchronization therapy. Circ J 2005;69:1521-6.
Machac J, Horowitz SF, Fagerstrom R, Levine R, Goldsmith SJ. Characterization and automatic identification of ECG conduction abnormalities using segmental multiharmonic Fourier analysis of gated blood-pool scintigrams. Eur J Nucl Med 1985;11:210-6.
Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med 1995;36:2138-47.
Faber TL, Cooke CD, Folks RD, Vansant JP, Nichols KJ, DePuey EG, et al. Left ventricular function and perfusion from gated SPECT perfusion images: An integrated method. J Nucl Med 1999;40:650-9.
Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by phase analysis of ECG-gated myocardial perfusion SPECT imaging: Development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol 2005;12:687-95.
Nakajima K, Kumita S, Ishida Y, Momose M, Hashimoto J, Morita K, et al. Creation and characterization of Japanese standards for myocardial perfusion SPECT: Database from the Japanese Society of Nuclear Medicine Working Group. Ann Nucl Med 2007;21:505-11.
Nakajima K. Normal values for nuclear cardiology: Japanese databases for myocardial perfusion, fatty acid and sympathetic imaging and left ventricular function. Ann Nucl Med 2010;24:125-35.
Garcia EV, Faber TL, Cooke CD, Folks RD, Chen J, Santana C. The increasing role of quantification in clinical nuclear cardiology: The Emory approach. J Nucl Cardiol 2007;14:420-32.
Germano G, Kavanagh PB, Slomka PJ, Van Kriekinge SD, Pollard G, Berman DS. Quantitation in gated perfusion SPECT imaging: The Cedars-Sinai approach. J Nucl Cardiol 2007;14:433-54.
Nakae I, Hayashi H, Matsumoto T, Mitsunami K, Horie M. Clinical usefulness of a novel program “Heart Function View” for evaluating cardiac function from gated myocardial perfusion SPECT. Ann Nucl Med 2014;28:812-23.
Lomsky M, Richter J, Johansson L, Hoilund-Carlsen PF, Edenbrandt L. Validation of a new automated method for analysis of gated-SPECT images. Clin Physiol Funct Imaging 2006;26:139-45.
Nakajima K, Okuda K, Nystrom K, Richter J, Minarik D, Wakabayashi H, et al. Improved quantification of small hearts for gated myocardial perfusion imaging. Eur J Nucl Med Mol Imaging 2013;40:1163-70.
Chen J, Henneman MM, Trimble MA, Bax JJ, Borges-Neto S, Iskandrian AE, et al. Assessment of left ventricular mechanical dyssynchrony by phase analysis of ECG-gated SPECT myocardial perfusion imaging. J Nucl Cardiol 2008;15:127-36.
O’Connell JW, Schreck C, Moles M, Badwar N, DeMarco T, Olgin J, et al. A unique method by which to quantitate synchrony with equilibrium radionuclide angiography. J Nucl Cardiol 2005;12:441-50.
Van Kriekinge SD, Nishina H, Ohba M, Berman DS, Germano G. Automatic global and regional phase analysis from gated myocardial perfusion SPECT imaging: Application to the characterization of ventricular contraction in patients with left bundle branch block. J Nucl Med 2008;49:1790-7.
Takahashi N, Yamamoto A, Tezuka S, Ishikawa M, Abe J, Amitani K, et al. Assessment of left ventricular dyssynchrony during development of heart failure by a novel program using ECG-gated myocardial perfusion SPECT. Circ J 2008;72:370-7.
Keida T, Ohira H, Fujita M, Chinen T, Nakamura K, Kato T, et al. Quantitative assessment of dyssynchrony using ECG-gated SPECT myocardial perfusion imaging prior to and following cardiac resynchronization therapy. Circ J 2009;73:1550-3.
Hida S, Chikamori T, Tanaka H, Igarashi Y, Shiba C, Usui Y, et al. Diagnostic value of left ventricular dyssynchrony after exercise and at rest in the detection of multivessel coronary artery disease on single-photon emission computed tomography. Circ J 2012;76:1942-52.
Igarashi Y, Chikamori T, Hida S, Tanaka H, Shiba C, Usui Y, et al. Usefulness of phase analysis to differentiate ischemic and non-ischemic etiologies of left ventricular systolic dysfunction in patients with heart failure. Circ J 2014;78:141-50.
Henneman MM, Chen J, Dibbets-Schneider P, Stokkel MP, Bleeker GB, Ypenburg C, et al. Can LV dyssynchrony as assessed with phase analysis on gated myocardial perfusion SPECT predict response to CRT? J Nucl Med 2007;48:1104-11.
Singh H, Patel CD, Sharma P, Naik N, Singh S, Narang R. Does perfusion pattern influence stress-induced changes in left ventricular mechanical dyssynchrony on thallium-201-gated SPECT myocardial perfusion imaging? J Nucl Cardiol 2015;22:36-43.
Acknowledgements
The study was performed as part of the JSNM working group activity of “Creation of common databases in nuclear cardiology and cross-calibration among software programs (2014-2015),” and supported partly by the JSNM fund and JSPS Grants-in-Aid for Scientific Research (C) in Japan (No. 15K09947, PI: K. Nakajima). Authors would like to thank Syntermed, Inc. (Atlanta, GA, USA) for kindly allowing us to use ECTb with SyncTool software. We also would like to thank Mr. Ronald Belisle for his editorial assistance.
Disclosures
K Nakajima has a collaborative research work with FUJIFILM RI Pharma Co. Ltd, Tokyo, Japan, which developed cardioREPO software, and has also been involved in the development of Heart Function View by Nihon Medi-Physics, Co. Ltd, Tokyo, Japan. E. Garcia receives royalties from the sale of phase analysis tools with the Emory Cardiac Toolbox (Syntermed Inc., Atlanta, GA, USA). The terms of this arrangement are managed by Emory University’s conflict of interest committee.
Author information
Authors and Affiliations
Corresponding author
Additional information
See related editorial, doi:10.1007/s12350-016-0438-y.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Nakajima, K., Okuda, K., Matsuo, S. et al. Comparison of phase dyssynchrony analysis using gated myocardial perfusion imaging with four software programs: Based on the Japanese Society of Nuclear Medicine working group normal database. J. Nucl. Cardiol. 24, 611–621 (2017). https://doi.org/10.1007/s12350-015-0333-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12350-015-0333-y