
Abstract
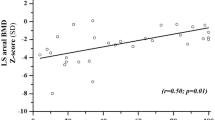
Friedreich ataxia (FRDA) is the most common inherited neurodegenerative ataxia. Apart from predominant neurological features an involvement of the skeletal system in terms of scoliosis and foot deformities is frequent. Disease-related falls, mobility restrictions, and wheelchair-dependency in later disease stages might additionally compromise bone structure in FRDA. The aim of this pilot study was to systematically evaluate the bone status in a representative FRDA cohort. Twenty-eight FRDA patients became enrolled in this cross-sectional study. Neurological assessment, a questionnaire comprising the history of fractures and osteoporosis as well as osteodensitometric measurements complemented with general and bone-specific laboratory parameters were performed. The WHO Fracture Risk Assessment tool (FRAX®) was applied, calculating the 10-year risk of suffering an osteoporotic fracture. Six patients (21.4 %) presented with a bone mineral density below the expected range for age in at least one of the examined sites (femoral neck, lumbar spine, and forearm) irrespective of their gender. Corresponding Z scores were significantly lower compared to normative values for the femoral neck and lumbar spine. Vitamin D status was insufficient in 11 and deficient in 8 FRDA patients. There was a strong negative correlation between ataxia severity, GAA repeat expansion and bone density in the femoral neck of FRDA patients. This is the first report of an increased rate of low bone mineral density in FRDA. Given the increased risk of falls, this data rectifies routine bone mineral density measurements in FRDA which may help to initiate therapeutic interventions to prevent this condition.


Similar content being viewed by others


References
Campuzano V, Montermini L, Molto MD, Pianese L, Cossee M, Cavalcanti F, et al. Friedreich’s ataxia: autosomal recessive disease caused by an intronic GAA triplet repeat expansion. Science. 1996;271:1423–7.
Harding AE. Friedreich's ataxia: a clinical and genetic study of 90 families with an analysis of early diagnostic criteria and intrafamilial clustering of clinical features. Brain. 1981;104:589–620.
Pandolfo M. Friedreich ataxia: the clinical picture. J Neurol. 2009;256 Suppl 1:3–8.
Durr A, Cossee M, Agid Y, Campuzano V, Mignard C, Penet C, et al. Clinical and genetic abnormalities in patients with Friedreich's ataxia. N Engl J Med. 1996;335:1169–75.
Milbrandt TA, Kunes JR, Karol LA. Friedreich's ataxia and scoliosis: the experience at two institutions. J Pediatr Orthop. 2008;28:234–8.
Labelle H, Tohme S, Duhaime M, Allard P. Natural history of scoliosis in Friedreich's ataxia. J Bone Joint Surg Am. 1986;68:564–72.
Schöls L, Amoiridis G, Przuntek H, Frank G, Epplen JT, Epplen C. Friedreich’s ataxia. Revision of the phenotype according to molecular genetics. Brain. 1997;120:2131–40.
Delatycki MB, Holian A, Corben L, Rawicki HB, Blackburn C, Hoare B, et al. Surgery for equinovarus deformity in Friedreich's ataxia improves mobility and independence. Clin Orthop Relat Res. 2005;430:138–41.
Geoffroy G, Barbeau A, Breton G, Lemieux B, Aube M, Leger C, et al. Clinical description and roentgenologic evaluation of patients with Friedreich's ataxia. Can J Neurol Sci. 1976;3:279–86.
NIH Consensus Development Panel on Osteoporosis Prevention DaT. Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001;285:785–95.
Bianchi ML. Osteoporosis in children and adolescents. Bone. 2007;41:486–95.
Smith ÉM, Comiskey CM, Carroll M. A study of bone mineral density in adults with disability. Arch Phys Med Rehabil. 2009;90:1127–35.
van den Bos F, Speelman AD, van Nimwegen M, van der Schouw YT, Backx FJ, Bloem BR, et al. Bone mineral density and vitamin D status in Parkinson’s disease patients. J Neurol. 2013;260:754–60.
Schmitz-Hubsch T, du Montcel ST, Baliko L, Berciano J, Boesch S, Depondt C, et al. Scale for the assessment and rating of ataxia: development of a new clinical scale. Neurology. 2006;66:1717–20.
Looker AC, Johnston Jr CC, Wahner HW, Dunn WL, Calvo MS, Harris TB, et al. Prevalence of low femoral bone density in older U.S. women from NHANES III. J Bone Miner Res. 1995;10:796–802.
Kelly TL, Wilson KE, Heymsfield SB. Dual energy X-ray absorptiometry body composition reference values from NHANES. PLoS One. 2009;4:e7038.
Lewiecki EM, Gordon CM, Baim S, Leonard MB, Bishop NJ, Bianchi ML, et al. International Society for Clinical Densitometry 2007 Adult and Pediatric Official Positions. Bone. 2008;43:1115–21.
Kanis JA, Oden A, Johansson H, Borgstrom F, Strom O, McCloskey E. FRAX and its applications to clinical practice. Bone. 2009;44:734–43.
McCloskey E, Kanis JA. FRAX updates 2012. Curr Opin Rheumatol. 2012;24:554–60.
Kanis JA, Burlet N, Cooper C, Delmas PD, Reginster JY, Borgstrom F, et al. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int. 2008;19:399–428.
Watts NB. Fundamentals and pitfalls of bone densitometry using dual-energy X-ray absorptiometry (DXA). Osteoporos Int. 2004;15:847–54.
Dachverband Osteologie e.V. DVO Guideline 2009 for Prevention, Diagnosis and Therapy of Osteoporosis in Adults. Osteologie. 2011;20:55–74.
Tangpricha V, Pearce EN, Chen TC, Holick MF. Vitamin D insufficiency among free-living healthy young adults. Am J Med. 2002;112:659–62.
Holick MF. Optimal vitamin D status for the prevention and treatment of osteoporosis. Drugs Aging. 2007;24:1017–29.
Schulz JB, Boesch S, Bürk K, Dürr A, Giunti P, Mariotti C, et al. Diagnosis and treatment of Friedreich ataxia: a European perspective. Nat Rev Neurol. 2009;5:222–34.
Kanis JA, Johansson H, Oden A, McCloskey EV. Assessment of fracture risk. Eur J Radiol. 2009;71:392–7.
Parkinson MH, Boesch S, Nachbauer W, Mariotti C, Giunti P. Clinical features of Friedreich's ataxia: classical and atypical phenotypes. J Neurochem. 2013;126:103–17.
Acknowledgments
We gratefully thank our FRDA patients for participating in this study. Furthermore, we thank Prof. Hanno Ulmer from the Department of Medical Statistics, Innsbruck Medical University for his consulting statistical service. AE, WN and SB are members of the European Friedreich's Ataxia Consortium for Translational Studies (EFACTS).
Conflict of Interest
The authors declare no financial or other conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Eigentler, A., Nachbauer, W., Donnemiller, E. et al. Low Bone Mineral Density in Friedreich Ataxia. Cerebellum 13, 549–557 (2014). https://doi.org/10.1007/s12311-014-0568-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12311-014-0568-1