
Abstract
Background
Spontaneous pneumocephalus in the nontraumatic setting is distinctly unusual. Pneumocephalus from central nervous system infection with Clostridium septicum has been rarely reported, and more commonly reflects a later stage of abscess formation. We present an unusual case of invasive C. septicum infection without an associated diagnosed malignancy presenting with rapidly progressive CNS pathology and resultant early pneumocephalus.
Methods
Medical records, radiologic imaging, and microbiological specimens of a case were reviewed.
Results
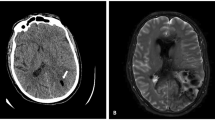
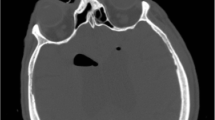
A 66-year-old male presented with a history of two witnessed generalized tonic–clonic seizures on awakening. He was found unresponsive at the scene by paramedics and subsequently intubated. There was no reported antecedent symptomatology, such as headache, fever, chills, focal weakness, and speech or gait disturbances. Medical history was remarkable only for diet-controlled hypertension. Computed tomography (CT) head imaging revealed an abnormal right parietal hypodensity. The patient was evaluated per the acute stroke protocol but was not deemed a candidate for intervention or thrombolytic therapy given the uncertainty of his clinical presentation; intravenous antibiotics were administered for possible sepsis. Follow-up CT imaging of the head performed 8 h later revealed right parieto-temporal pneumocephalus with extensive cerebral edema and effacement of basilar cisterns. Neurosurgical intervention was not deemed appropriate given the catastrophic nature of his injury and the patient subsequently expired 14 h after presentation. Blood cultures grew gram-positive rods in three of four bottles identified as C. septicum.
Conclusions
Clostridium septicum is an uncommon and often fatal cause of nontraumatic pneumocephalus. This underscores the need for a high index of clinical suspicion in cases with unexplained pneumocephalus, as early diagnosis remains the key to survival. In survivors of C. septicum infection, subsequent colonoscopy should be considered to exclude undiagnosed or occult gastrointestinal malignancy.



Similar content being viewed by others

References
Ragland RL, Knorr JR, Lee GM, DeGirolami U, Gelber ND. Clostridium septicum meningoencephalitis: an unusual presentation of occult rectal carcinoma. Am J Neuroradiol. 1992;13:1487–8.
Marangou AG, Joske RA, Kaard AO, Thomas W. Cerebral abscess due to Clostridium septicum. J R Soc Med. 1992;85:641.
Seder CW, Kramer M, Long G, Uzieblo MR, Shanley CJ, Bove P. Clostridium septicum aortitis: report of two cases and review of the literature. J Vasc Surg. 2009;49(5):1304–9.
Stevens DL, Musher DM, Watson DA, et al. Spontaneous, nontraumatic gangrene due to Clostridium Septicum. Rev Infect Dis. 1990;12(2):286–96.
Foga MM, McGinn GJ, Kroeker MA, Guzman R. Sepsis due to Clostridium septicum: case report. Can Assoc Radiol J. 2000;51(2):85–9.
Johnson S, Driks MR, Tweten RK, et al. Clinical courses of seven survivors of Clostridium septicum infection and their immunologic responses to alpha toxin. Clin Infect Dis. 1994;19(4):761–4.
Alpern RJ, Dowell VR. Clostridium septicum infections and malignancy. JAMA. 1969;209(3):385–8.
Kornbluth AA, Danzig JB, Bernstein LH. Clostridium septicum infection and associated malignancy. Medicine. 1989;68:30–7.
Calabek B, Hinterholzer G, Neuwirth-Senautka G, et al. Clostridium Septicum encephalitis: a case report, pathogensis of encephalitis (2011), D. Hayasaka (ed), ISBN: 978-953-307-741-3, InTech. http://www.intechopen.com/books/pathogenesis-of-encephalitis/clostridium-septicum-encephalitis-a-case-report
Roeltgen D, Shugar G, Towfighi J. Cerebritis due to Clostridium septicum. Neurology. 1980;30:1314–6.
Gorse GJ, Slater LM, Sobol E, Kim RC, Wishnow RM, Cesario TC. CNS Infection and Bacteremia due to Clostridium septicum. Arch Neurol. 1984;41:882–4.
Chiang V, Adelson PD, Poussaint TY, Hand M, Churchwell KB. Brain Abscesses caused by Clostridium septicum as a complication of hemolytic-uremic syndrome. Pediatr Infect Dis J. 1995;14(1):72–4.
Cheng YT, Huang CT, Leu HS, Chen JS, Kiu MC. Central nervous system infection due to Clostridium septicum: a case report and review of the literature. Infection. 1997;25:171–4.
Bhogal P, Bhatnagar G, Manieson J, Booth T, Prendergast C. An unusual case of pneumocephalus. BMG Case Rep. 2011;. doi:10.1136/bcr.06.2010.3106.
Randall JM, Hall K, Coulthard MG. Diffuse pneumocephalus due to Clostridium septicum cerebritis in haemolytic uraemic syndrome: CT demonstration. Neuroradiology. 1993;35:218–20.
Martin SE, Allen SD, Faught P, Hawley DA, Bonnin JM, Hattab EM. A 2-year old boy with hemolytic uremic syndrome and pneumocephalus. Brain Pathol. 2012;22:121–4.
Markam JW. Clinical features of pneumocephalus based upon a survey of 284 cases with report of 11 additional cases. Acta Neurochir. 1967;16:1–78.
Hwang T, Fremaux R, Sears ES, et al. Confirmation of cerebral air embolism with computerized tomography. Ann Neurol. 1983;13:214–5.
Broughton RA, Lee EY. Clostridium Septicum sepsis and meningitis as a complication of the hemolytic-uremic syndrome. Clin Pediatr. 1993;32:750–2.
Dirks C, Horn H, Christensen L, Pedersen C. CNS infection with Clostridium septicum. Scand J Infect Dis. 2000;32:320–2.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Financial Disclosures
None.
Rights and permissions
About this article

Cite this article
Katyal, A., Dmello, D. Clostridium septicum Pneumocephalus. Neurocrit Care 24, 264–267 (2016). https://doi.org/10.1007/s12028-015-0192-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-015-0192-z